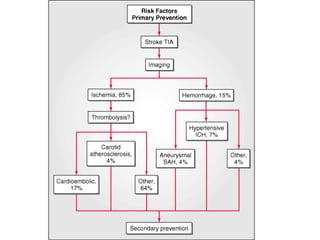
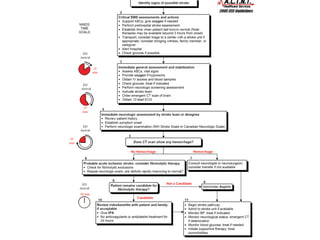
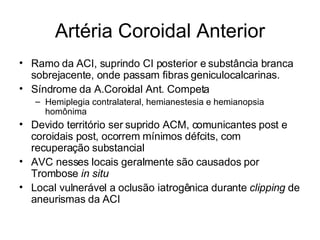
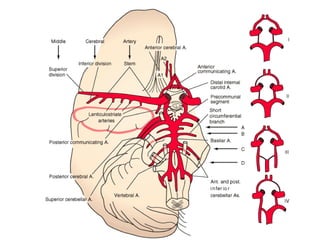
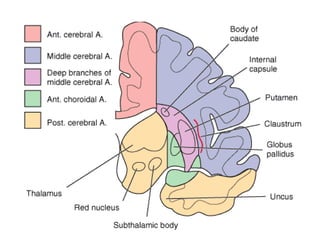
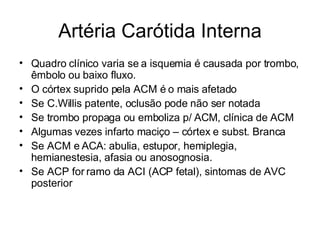
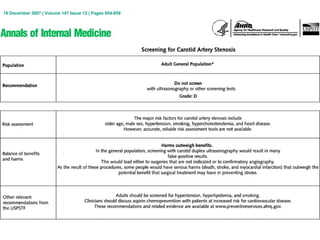
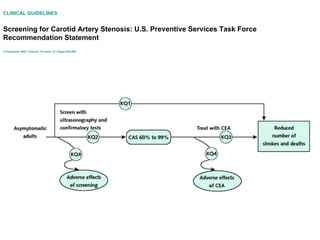
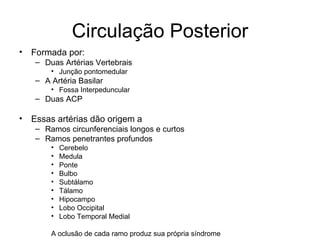
Este documento discute a semiologia de acidente vascular cerebral isquêmico, descrevendo as principais artérias cerebrais e os sintomas associados à oclusão de cada uma. Detalha os principais exames para triagem pré-hospitalar de AVC e apresenta um estudo comparando os resultados do tratamento urgente versus não urgente após um AIT ou AVC menor.

![Incidence and prognosis of transient neurological attacks. JAMA 298:2877, 2007 CONTEXT: Transient neurological attacks (TNAs) are attacks with temporary (<24 hours) neurological symptoms. These symptoms can be focal, nonfocal, or a mixture of both. The prognostic significance of TNAs with focal symptoms (better known as transient ischemic attacks [TIAs]) is well understood. Conversely, hardly anything is known about the prognostic significance of TNAs with nonfocal or mixed symptoms. OBJECTIVE: To study the incidence and prognosis of focal TNAs (or TIAs), nonfocal TNAs, and mixed TNAs. DESIGN, SETTING, AND PARTICIPANTS: The study population comprised 6062 community-dwelling Rotterdam Study participants who were aged 55 years or older and free from stroke, myocardial infarction, and dementia at baseline (1990-1993). They were followed up for events until January 1, 2005. We analyzed the associations between incident TNAs and subsequent adverse events with age- and sex-adjusted Cox regression models. MAIN OUTCOME MEASURES: Stroke, ischemic heart disease, or dementia. RESULTS: During 60 535 person-years, 548 participants developed TNA (282 focal, 228 nonfocal, and 38 mixed). The incidence rate per 1000 person-years was 4.7 (95% confidence interval [CI], 4.1-5.2) for focal TNA, 3.8 (95% CI, 3.3-4.3) for nonfocal TNA, and 0.6 (95% CI, 0.4-0.9) for mixed TNA. Participants with focal TNA were at higher risk of subsequent stroke than participants without TNA (n = 46 vs 540; hazard ratio [HR], 2.14; 95% confidence interval [CI]; 1.57-2.91) but had an equal risk of ischemic heart disease and dementia. Nonfocal TNA patients were at higher risk of stroke (27 vs 540; HR, 1.56; 95% CI, 1.08-2.28) and dementia (30 vs 552; HR, 1.59; 95% CI, 1.11-2.26) than participants without TNA. Mixed TNA patients were at higher risk of stroke (6 vs 540; HR, 2.48; 95% CI, 1.11-5.56), ischemic heart disease (8 vs 779; HR, 2.26; 95% CI, 1.07-4.78), vascular death (8 vs 594; HR, 2.54; 95% CI, 1.31-4.91), and dementia (7 vs 552; HR, 3.46; 95% CI, 1.72-6.98) than participants without TNA. CONCLUSION: Patients who experience nonfocal TNAs, and especially those with mixed TNAs, have a higher risk of major vascular diseases and dementia than persons without TNA](https://image.slidesharecdn.com/semiologia-do-ave-isqumico-20022008-1203618673234386-5/85/Semiologia-Do-AVE-IsqueMico-20-02-2008-49-320.jpg)
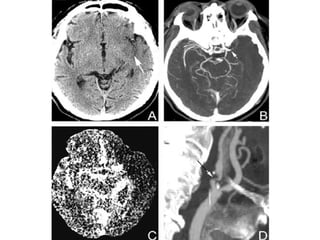
![Impact of abnormal diffusion-weighted imaging results on short-term outcome following transient ischemic attack. Archives of Neurology 64:1105, 2007 OBJECTIVE: To characterize short-term prognoses among patients with transient ischemic attack (TIA) and normal diffusion-weighted imaging (DWI) results, TIA patients with abnormal DWI results (transient symptoms associated with infarction [TSI]), and patients with completed ischemic stroke (IS). DESIGN: Retrospective study. PATIENTS: We reviewed patient medical records between January 2003 and December 2004 with International Classification of Diseases, Ninth Revision codes for TIA at admission, resolution of neurological symptoms within 24 hours, magnetic resonance imaging within 48 hours, and a discharge diagnosis of TIA or IS. A random sample of 50 IS patients was selected from all IS admissions and discharges by International Classification of Diseases, Ninth Revision codes. Demographic, clinical, radiographic, and in-hospital outcome data were recorded. Three diagnostic categories were created: TIA with normal DWI results, TSI, and IS. Multivariate logistic regression was used to estimate the association between diagnostic category and rate of in-hospital stroke or recurrent TIA among the 3 groups. RESULTS: We identified 146 classic TIA (25% with TSI) and 50 IS cases. There were 4 recurrent TIAs and 6 strokes among patients with TSI (27.0%); 3 recurrent TIAs and no strokes among patients with normal DWI results (2.8%); and 1 recurrent stroke and no TIAs among IS patients (2.0%). Transient symptoms associated with infarction was independently associated with in-hospital recurrent TIA or stroke (adjusted odds ratio, 11.2; P < .01). CONCLUSIONS: Transient symptoms associated with infarction is associated with a greater rate of early recurrent TIA and stroke than both IS and TIA with normal DWI results. These data suggest that TSI may be a separate clinical entity with unique prognostic implications.](https://image.slidesharecdn.com/semiologia-do-ave-isqumico-20022008-1203618673234386-5/85/Semiologia-Do-AVE-IsqueMico-20-02-2008-51-320.jpg)



































































