Transferir como PDF, PPTX


![0.6
0.4
0.0
0.2
Probability
0.8
1.0
were unknown in that cohort [3]. In the Children’s Cancer Group however, and long-term outcomes were not r
study 5912, the DECAL regimen was given to 68 patients with theless, perhaps in part because of the encour
recurrent NHL with a 50% response rate, which was independent of studies ICE has become a commonly employe
A study of rituximab histologic subtype. OS carboplatin, and etoposide chemotherapy in children with
and ifosfamide, was 33% at 2 years but only 2/13 patients pediatric patients with relapsed NHL.
recurrent/refractory B‐celldescribed as non‐Hodgkin lymphoma and mature B‐cell acutepatients enrolled
The small number of
with BL were (CD20+) long-term survivors [5]. Kung et al.
lymphoblastic a 71% CR/PR A report fromOncology Group trial Oncology Group conclusions regarding the t
reported leukemia: rate in a Pediatric the Children's of preclude definitive
the combination of rituximab and ICE chemo
the response rate observed (60%) appears to b
to previous reports of other salvage regime
impressive in view of the prior, intensive con
received by the patients. Many with OR we
consolidative therapy with SCT, and the prop
alive and free of disease at last follow-up
previously published series of such patients
DLBCL group, two of the survivors did n
consolidation therapy with SCT.
Patients enrolled in this trial had a very sho
not respond to salvage therapy, while those w
disease had a chance at successful retrieval
perhaps more effective relapse therapy, the
response to initial retrieval therapy and su
diseases such as Hodgkin lymphoma, may
high-grade B-cell malignancies as well.
The commercial availability of rituxim
opportunity to combine it with chemotherapy
0.0
0.5
1.0
1.5
2.0
2.5
3.0
ICE, for use in relapsed or refractory high-gr
Years
outside the setting of a clinical trial. The curr
Survival
Number Number Number
because it provides controlled data regardin
Time interval Estimate SE failed Censored at risk
regimen as well as some response data.
0-1 year
0.4286 0.1145
11
1
20
rituximab and ICE chemotherapy was delivere
1-2 years
0.3750 0.2096
1
5
8
or excessive toxicity. Infusion-related toxicit
2-3 years
0.3750
.
0
2
2
but manageable, and no patient experienc
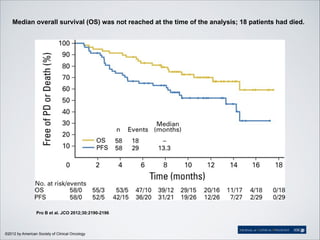
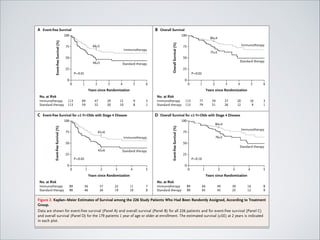
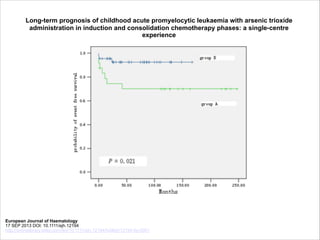
Fig. 1. Overall survival: All eligible patients.
reactions that have been reported in patients w
Pediatr Blood Cancer DOI 10.1002/pbc
Pediatric Blood & Cancer
Volume 52, Issue 2, pages 177-181, 24 SEP 2008 DOI: 10.1002/pbc.21753
http://onlinelibrary.wiley.com/doi/10.1002/pbc.21753/full#fig1](https://image.slidesharecdn.com/terapiaalvopediatria-131027103738-phpapp01/85/Terapia-alvo-na-cancerologia-pediatrica-12-320.jpg)
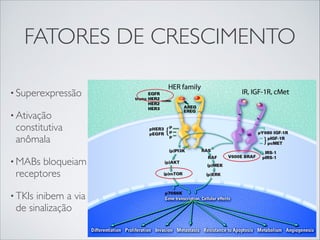
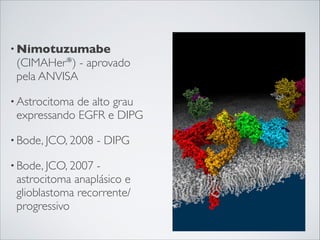
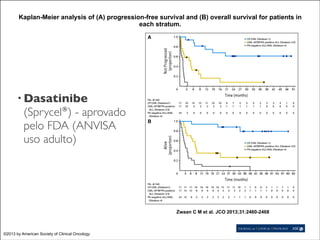
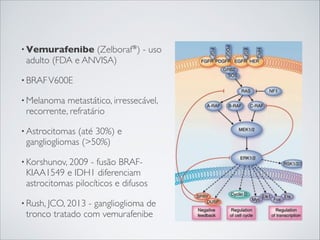

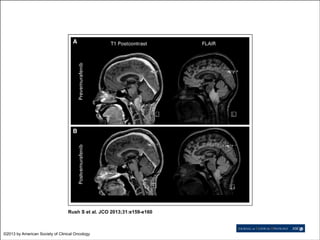
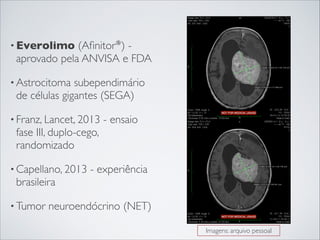
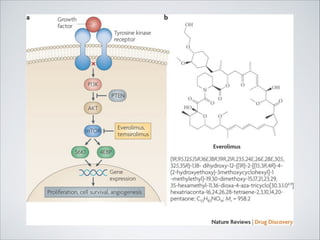
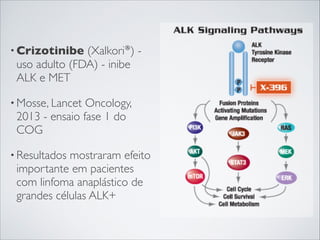
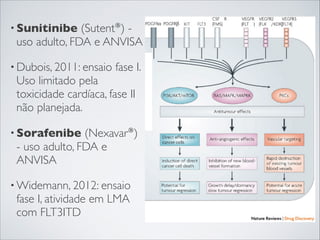


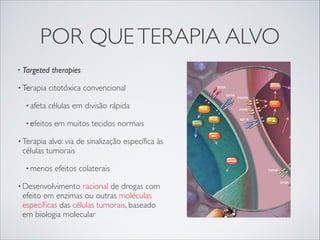
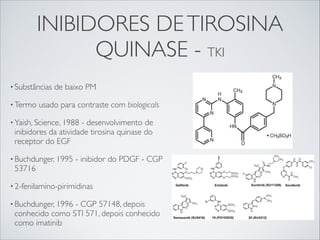
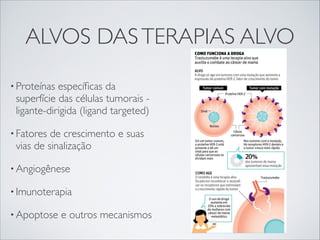
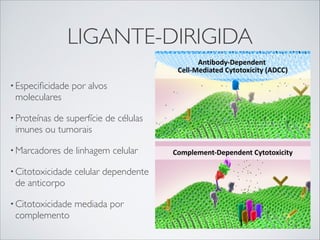
O documento discute as terapias alvo em pediatria, destacando três pontos: 1) as terapias alvo afetam vias de sinalização específicas de células tumorais, causando menos efeitos colaterais que a quimioterapia convencional; 2) exemplos de terapias alvo incluem anticorpos monoclonais, inibidores de tirosina quinase e medicamentos que inibem fatores de crescimento; 3) ensaios clínicos em crianças estão avaliando o potencial das terapias








































































