Baixado 135 vezes
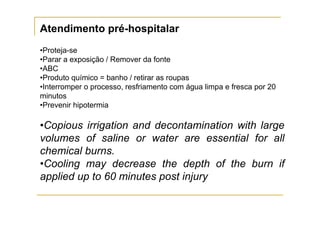
![TC= [(F – 32)/9] x 5
71
60
54
44](https://image.slidesharecdn.com/tratamentodacrianaqueimada-110808174544-phpapp02/85/Tratamento-da-crianca-queimada-21-320.jpg)
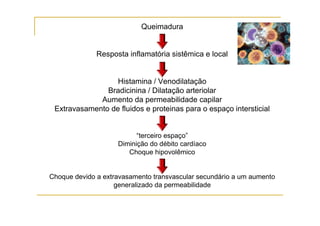
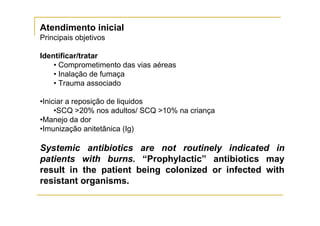

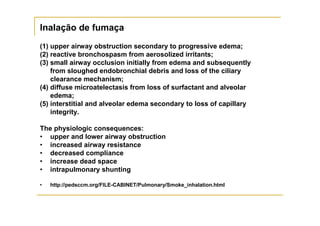
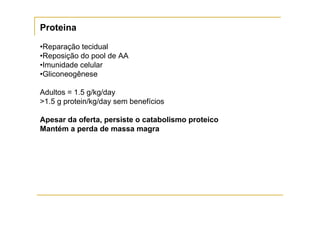
![Review Article
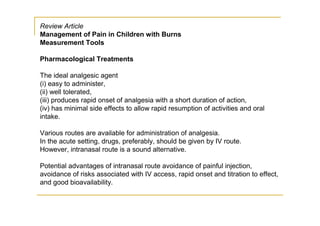
Management of Pain in Children with Burns
Measurement Tools
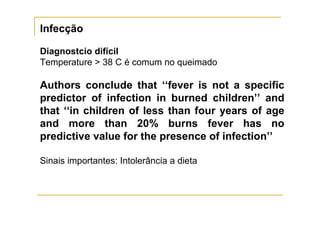
Faces/Ladder Scale.
Wong-Baker FACES Pain
Rating Scale is recommended for children
≥3 years of age].
The faces/ladder scale
should be explained to the child
What the child states as
their pain score—either from using
the numbers or faces on a scale
of 0–10—should then be
documented.](https://image.slidesharecdn.com/tratamentodacrianaqueimada-110808174544-phpapp02/85/Tratamento-da-crianca-queimada-62-320.jpg)
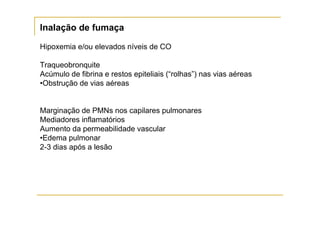
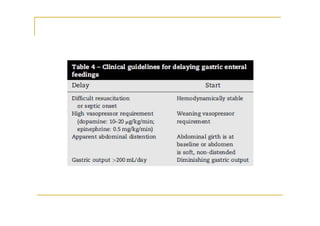
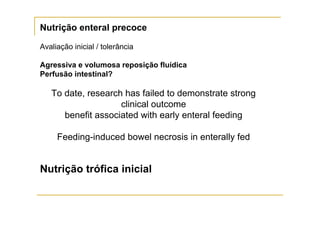
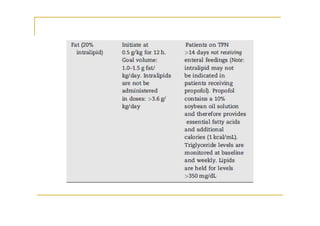

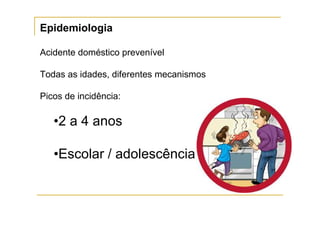
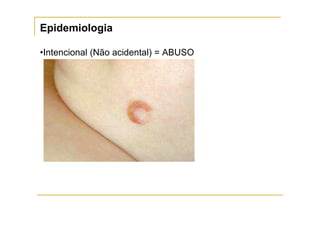
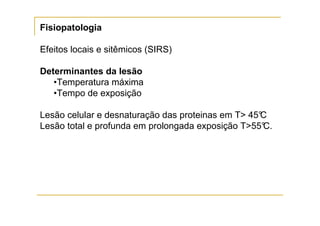
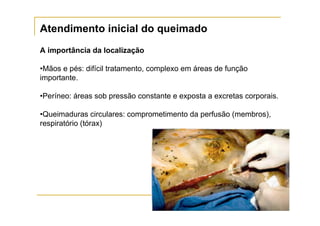
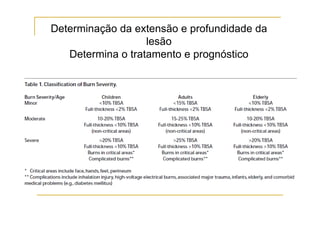
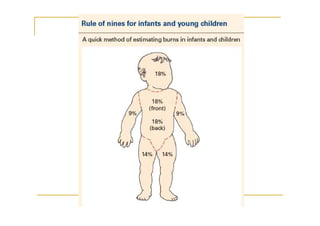
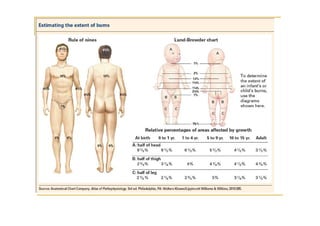
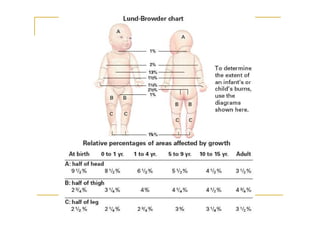
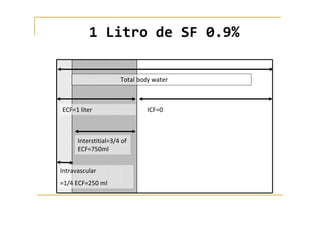
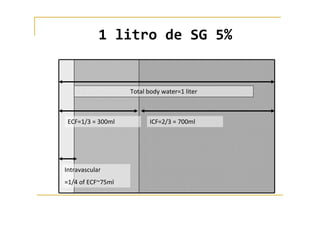
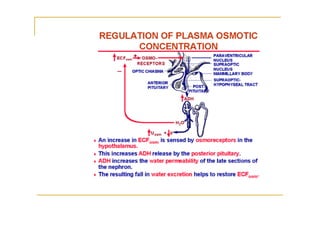
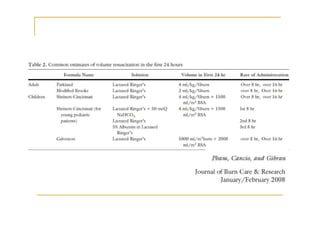
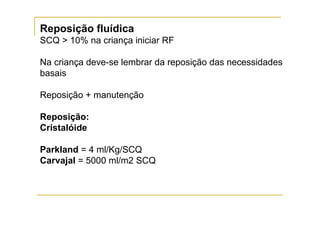
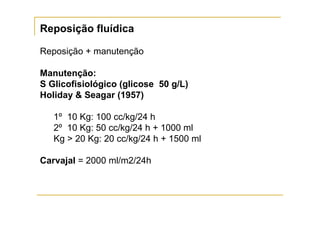
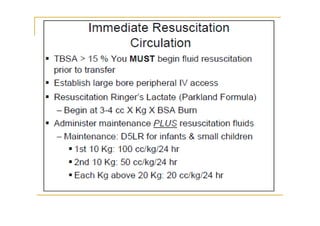
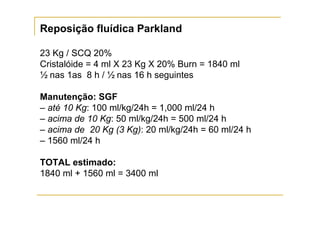
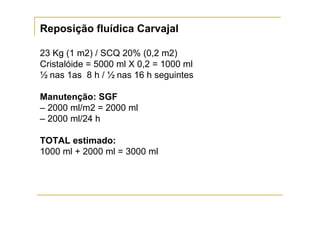
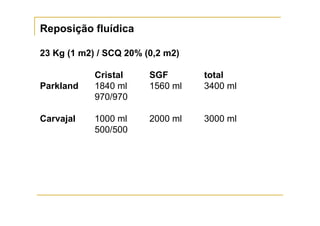
O documento discute o tratamento da criança queimada, incluindo: 1) A importância do atendimento inicial e da reposição fluida adequada para prevenir o choque; 2) As formulas de Parkland e Carvajal para calcular a reposição fluida inicial baseada na superficie corporal queimada; 3) A necessidade de monitorar cuidadosamente a resposta ao tratamento e ajustar a reposição fluida de acordo com os sinais vitais e urinários da criança.


![Pediatria Aula Emergencias Pediatricas[ Revisado]](https://cdn.slidesharecdn.com/ss_thumbnails/pediatriaaulaemergenciaspediatricasrevisado-090828124616-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)












































![Cardiac and respiratory support 2017 [modo de compatibilidade]](https://cdn.slidesharecdn.com/ss_thumbnails/cardiacandrespiratorysupport2017mododecompatibilidade-170828132402-thumbnail.jpg?width=640&height=640&fit=bounds)


















