O Papel da Hipófise na Regulação do Crescimento
•
1 gostou•264 visualizações

A bolsa de Rathke, um divertículo da cavidade oral primitiva (ectoderma oral) da origem à adeno-hipófise. A neurohipófise ou (hipófise posterior) se origina do ectoderma neural da base do cérebro, que também se envolve no terceiro ventrículo. A adeno-hipófise normalmente constitui 80% do peso da hipófise e é dividida nos lobos anterior, intermediário e infundibular. Em humanos, o lobo anterior é o maior componente e abriga a maioria das células produtoras de hormônios.

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (17)
Semelhante a O Papel da Hipófise na Regulação do Crescimento
Semelhante a O Papel da Hipófise na Regulação do Crescimento (20)
Mais de Van Der Häägen Brazil
Mais de Van Der Häägen Brazil (20)
Último
Último (11)
O Papel da Hipófise na Regulação do Crescimento
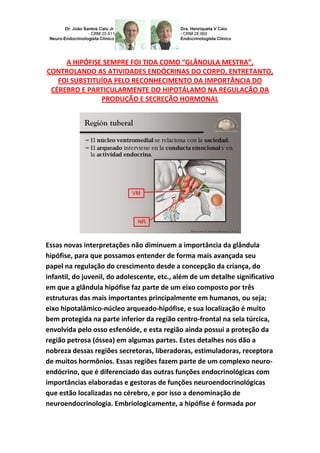
- 1. A HIPÓFISE SEMPRE FOI TIDA COMO “GLÂNDULA MESTRA”, CONTROLANDO AS ATIVIDADES ENDÓCRINAS DO CORPO, ENTRETANTO, FOI SUBSTITUÍDA PELO RECONHECIMENTO DA IMPORTÂNCIA DO CÉREBRO E PARTICULARMENTE DO HIPOTÁLAMO NA REGULAÇÃO DA PRODUÇÃO E SECREÇÃO HORMONAL Essas novas interpretações não diminuem a importância da glândula hipófise, para que possamos entender de forma mais avançada seu papel na regulação do crescimento desde a concepção da criança, do infantil, do juvenil, do adolescente, etc., além de um detalhe significativo em que a glândula hipófise faz parte de um eixo composto por três estruturas das mais importantes principalmente em humanos, ou seja; eixo hipotalâmico-núcleo arqueado-hipófise, e sua localização é muito bem protegida na parte inferior da região centro-frontal na sela túrcica, envolvida pelo osso esfenóide, e esta região ainda possui a proteção da região petrosa (óssea) em algumas partes. Estes detalhes nos dão a nobreza dessas regiões secretoras, liberadoras, estimuladoras, receptora de muitos hormônios. Essas regiões fazem parte de um complexo neuro- endócrino, que é diferenciado das outras funções endocrinológicas com importâncias elaboradas e gestoras de funções neuroendocrinológicas que estão localizadas no cérebro, e por isso a denominação de neuroendocrinologia. Embriologicamente, a hipófise é formada por
- 2. fontes distintas. A bolsa de Rathke, um divertículo da cavidade oral primitiva (ectoderma oral) da origem à adeno-hipófise. A neurohipófise ou (hipófise posterior) se origina do ectoderma neural da base do cérebro, que também se envolve no terceiro ventrículo. A adeno- hipófise normalmente constitui 80% do peso da hipófise e é dividida nos lobos anterior, intermediário e infundibular. Em humanos, o lobo anterior é o maior componente e abriga a maioria das células produtoras de hormônios. A bolsa de Rathke, que dá origem à adeno-hipófise, pode ser identificada no embrião de 3 mm durante a terceira semana de gravidez. As células produtoras de GH-hormônio de crescimento podem ser encontradas na adeno-hipófise pela nona semana de gravidez, e conexões vasculares entre o lobo anterior da hipófise e o hipotálamo se desenvolvem por volta deste período, apesar de que a produção de hormônio possa ocorrer na hipófise na ausência de conexões com o hipotálamo. Os Somatotrófos geralmente podem ser demonstrados na hipófise de recém-nascidos anencefálicos. Mesmo assim, parece provável que a iniciação do desenvolvimento da hipófise anterior seja dependente de respostas de fatores indutores do ectoderma oral do diencéfalo ventral. Uma complexa integração da expressão temporalmente ordenada e geograficamente restrita de múltiplos peptídeos sinalizadores
- 3. extracelulares e de fatores de transcrição regulares intracelulares deste processo de desenvolvimento. A hipófise em desenvolvimento e o hipotálamo estão anatomicamente próximos, ou melhor, em justaposição, e seus desenvolvimentos embriológicos provavelmente são codependentes. Alguns dos fatores diencefálicos que foram identificados como críticos na formação e padronização da bolsa de Rathke, que, em roedores, é iniciada no oitavo dia embriônico (e8), são as proteínas morfogenética 4 e 2 de ossos (BMP4/2), Wnt5a e fator de crescimento 8 de fibroblasto (FGF8). O sinal dorsal neuroepitelial, BMP4, é necessário para o “compromisso do órgão” da hipófise, enquanto o gradiente BMP2 (ventral) e FGF8 (dorsal) determinam os fenótipos das células hipofisárias (isto é, linhas dependentes de Gonadotrófos e Pit-1, Somatotrófos, Lactotrófos e Tireotrófos [ventral], e Metanotrófos e Corticotrófos [dorsal]). Parece que a interação recíproca de pelo menos 2 fatores de transcrição, ou seja, o Pit-1 e o GATA-2, são importantes para implementar os sinais de determinação celular BMP2 e FGF8. Estudos de explantes em roedores demonstraram que se a bolsa de Rathke é removida do ectoderma oral no (e 10. 5) e incubada em meio de cultura apropriada, a diferenciação de cada tipo célula hipofisária continua, indicando que, nesse ponto, a organogênese da hipófise anterior não é mais dependente de sinais do hipotálamo, porém esses sinais continuam criticamente envolvidos na produção de hormônios hipofisários dando sequência na liberação hormonal. Para se ter uma idéia da importância da adeno-hipófise principalmente para humanos, 50% da glândula que tem o tamanho de uma ervilha, só
- 4. secreta GH-hormônio de crescimento e os outros 50% secreta todos os outros hormônios hipofisários; TRH HORMONIO LIBERADOR DO TSH, CRH HORMÔNIO LIBERADOR DO ACTH, GnRH HORMÔNIO LIBERADOR DE GONADOTROFINAS, PRH HORMÔNIO LIBERADOR DE PROLACTINA, SOMATOSTATINA HORMÔNIO INIBIDOR DO GH E TSH, PIF HORMÔNIO INIBIDOR DA PROLACTINA E DE DOPAMINA. HOW CHILDREN AND YOUTH CHILDREN GROW; LOGISTICS AND ENDOCRINE CONTROL OF GROWTH-NEUROENDOCRINE. THE HYPOPHYSIS ALWAYS BEEN LIKE AS "MASTER GLAND" CONTROLLING THE ACTIVITIES OF ENDOCRINE BODY, HOWEVER WAS REPLACED BY THE RECOGNITION OF THE IMPORTANCE OF THE BRAIN AND PARTICULARLY THE HYPOTHALAMUS IN REGULATION OF PRODUCTION AND HORMONE SECRETION. PHYSIOLOGY- ENDOCRINOLOGY-NEUROENDOCRINOLOGY-GENETICS-ENDOCRINE- PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO. These new interpretations not diminish the importance of the pituitary gland, so we can understand more advanced form of its role in regulating growth from conception, child, infant, teen, etc., plus a significant detail in the pituitary gland part of a shaft comprising three structures of the most important especially in humans, namely: hypothalamic-pituitary-arcuate nucleus axis, and their locations are very well protected in the bottom of the center-frontal region of sella, the sphenoid bone involved it, this region still has the protection of the petrous region (bone) in some parts.
- 5. These details give us the nobility of these secretory regions, liberating, stimulating, and receiving many hormones. These regions are part of a complex neurological and endocrine, which is differentiated from other endocrine functions with elaborate amounts and management of neuroendocrine functions that are located in the brain, and so the name of neuroendocrinology. Embryologically, the pituitary gland is formed by different sources. The Rathke's pouch, is a diverticulum of the primitive oral cavity (oral ectoderm) of the anterior pituitary origin. The neurohypophysis or (posterior pituitary) originates from the neural ectoderm of the base of the brain, which also involves the third ventricle. The adeno pituitary normally constitutes 80% of the weight of the pituitary and is divided into anterior, intermediate and infundibular lobes. In humans, the anterior lobe is the largest component and local the majority of hormone producing cells. Rathke's pouch, the origin of the anterior pituitary, can be identified in the embryo of 3 mm during the third week of pregnancy. Cells producing growth hormone, GH may be found in the anterior pituitary at ninth week of pregnancy, and vascular connections between the anterior lobe of the pituitary and hypothalamus develops around this time, although hormone production may occur in the pituitary in the absence of connections with the hypothalamus. Somatotrophs can usually be demonstrated in the pituitary gland of anencephalic newborns. Even so, it seems likely that the initiation of development of the anterior pituitary is dependent on the oral ectoderm factors inducing ventral midbrain responses. A
- 6. complex integration of the expression temporally and geographically restricted ordered multiple peptides of intracellular and extracellular signaling factors that regulate transcription development process. The developing pituitary and the hypothalamus are anatomically in close juxtaposition, and their embryological developments are probably codependent. Diencephalic some of the factors that have been identified as critical in the formation and patterning of Rathke's pouch, which in rodents is initiated on the eighth day embryonic (e8) are the bone morphogenetic proteins 4 and 2 bone (BMP4/2), and Wnt5a fibroblast growth 8 (FGF8) factor. The dorsal neuroepithelial signal, BMP4, it is necessary to "compromise organ" in the pituitary gland while the gradient BMP2 (ventral) and FGF8 (dorsal) determine the phenotypes of pituitary cells (e.g., lines dependent Gonadotrophs and Pit-1, Somatotrophs, Lactotrophs, Thyrotrophs [ventral], and Metanotrophs and Corticotrophs [dorsal]). It seems that the reciprocal interaction of at least two transcription factors, Pit-1 and GATA-2, it is important to implement the signals of cell determination BMP2 and FGF8. Explant studies in rodents showed that the Rathke pouch is removed from the oral ectoderm (e 10. 5) and incubated in an appropriate culture medium,
- 7. differentiation of each pituitary cell type remains, indicating that, at this point, pituitary organogenesis former is not dependent on signals from the hypothalamus, but these signs are still critically involved in the production of pituitary hormones giving sequence in hormone release. To get an idea of the importance of the anterior pituitary primarily for humans, 50% of the gland about the size of a pea, only secret GH - GROWTH HORMONE AND THE OTHER 50% SECRET ALL OTHER PITUITARY HORMONES; HRT HORMONE RELEASING THE TSH, ACTH RELEASING CRH HORMONE, GnRH GONADOTROPIN-RELEASING HORMONE, PRH RELEASING PROLACTIN HORMONE, SOMATOSTATIN INHIBITOR OF GH AND TSHHORMONE, PROLACTIN INHIBITOR PIF AND DOPAMINE HORMONE. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna CRM 28930 Como saber mais: 1. O diagnóstico é através da medição de testosterona, hormônio luteinizante (LH), hormônio folículo-estimulante (FSH) e por testes de estimulação com gonadotrofina coriônica humana (hCG) ou hormônio liberador de gonadotrofina (GnRH)... http://hormoniocrescimentoadultos.blogspot.com 2. O tratamento depende da causa, existem 3 tipos de hipogonadismo: o hipogonadismo 1º a que daremos mais ênfase devido às complexidades dessa síndrome, o hipogonadismo 2º e um tipo causado pela ação dos androgênios defeituosos, principalmente devido à atividade do receptor defeituoso de andrógeno... http://longevidadefutura.blogspot.com
- 8. 3. Hipogonadismo 1º, também chamado hipogonadismo hipergonadotrófico, causa danos às células de Leydig, prejudica a produção de testosterona, danifica os túbulos seminíferos, ou faz as duas coisas, leva à oligospermia ou azoospermia e resultado elevado de gonadotrofinas... http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Serge AMSELEM, bases moleculares e celulares das doenças genéticas, Inserm U 654, Armand-Trousseau Hospital, Paris; Jean-Claude CAREL, endocrinologia pediátrica e diabetologia, Inserm U 690, Robert Debré Hospital, Paris; Nicolas de Roux, Inserm U 690, Robert Debré Hospital, Paris; Tarik Issad, Departamento de Biologia Celular, René Descartes University, Instituto Cochin, CNRS / Inserm, Paris; Stefania MACCARI, Laboratório de Estresse Perinatal, da Universidade de Lille 1, Villeneuve d'Ascq; Vincent PREVOT, Desenvolvimento e plasticidade do cérebro pós-natal, Jean-Pierre Aubert Research Center, Inserm U 837, Universidade de Lille 2, Lille; Charles SUSANNE, Laboratório de Antropologia, Universidade Livre de Bruxelas, na Bélgica; Françoise ROVILLÉ-Sausse, UMR 5145 Eco-Antropologia, Museu Nacional de História Natural, Paris; Fabienne BONNIN, associado Científica, Inserm centro laudo pericial coletiva, Xavier Bichat-Faculdade de Medicina, Paris; Catherine Chenu, associado Científica, Inserm centro laudo pericial coletiva, Xavier Bichat- Faculdade de Medicina, Paris; Jeanne ÉTIEMBLE, Diretor, Inserm centro laudo pericial coletiva, Xavier Bichat- Faculdade de Medicina, Paris; Cécile GOMIS, Secretário, Inserm centro laudo pericial coletiva, Xavier Bichat- Faculdade de Medicina, Paris; Anne-Laure Pellier, associado Científica, Inserm centro laudo pericial coletiva, Xavier Bichat-Faculdade de Medicina, Paris; Chantal RONDET-Grellier, Documentalista, Inserm coletiva centro laudo pericial, Xavier Bichat-Faculdade de Medicina, Paris; Marie-Josèphe SAUREL-CUBIZOLLES, Expert avaliação associado, Inserm coletiva centro laudo pericial, Xavier Bichat-Faculdade de Medicina, Paris. Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr google.com/+JoãoSantosCaioJrvdh
- 9. google.com/+VANDERHAAGENBRAZILvdh Video http://youtu.be/woonaiFJQwY VAN DER HAAGEN BRAZI Instagram https://instagram.com/clinicascaio/ Google Maps: http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl=pt&sll=- 23.578256,46.645653&sspn=0.005074,0.009645&ie =UTF8&ll=-23.575591,-46.650481&spn=0,0&t = h&z=17