BAIXA ESTATURA/CRESCER:IMPORTÂNCIA ÍMPAR DA ADENO-HIPÓFISE CRESCIMENTO DE CRIANÇA/INFANTIL/JUVENIL.
•Transferir como DOCX, PDF•
0 gostou•690 visualizações

O documento discute a importância da glândula hipofisária, especialmente no que se refere à produção do hormônio do crescimento. A hipófise anterior, responsável pelo hormônio do crescimento, é o tecido mais vascularizado entre os mamíferos. Uma deficiência no hormônio do crescimento pode levar a problemas de baixa estatura em crianças.
![lobo posterior e dos seios cavernosos para a circulação geral. O sistema
porta-hipofisário dos capilares permite controlar a função da adeno-
hipófise por meio dos hormônios hipotalâmicos hipofiotróficos,
secretados para dentro dos vasos porta-hipofisários. Isso fornece uma
conexão curta e direta com a adeno-hipófise a partir do hipotálamo
ventral e da eminência mediana. Também pode existir fluxo retrógado
entre a hipófise e o hipotálamo, dando origem a um possível mecanismo
de feedback direto entre os hormônios hipofisários e seus centros de
controle neuroendócrinos. Atualmente, técnicas imunocitoquímicas e de
microscopia eletrônica permitiram a classificação das células por meio
de seus produtos secretórios específicos: células somatotrópicas (que
secretam hormônios de crescimento [GH]), células lactotróficas (que
secretam prolactina [PRL]), células tireotróficas (que secretam
tireotrofina [TRH]), células corticotróficas (que secretam ACTH e
peptídeos relacionados) e células gonadotróficas (que secretam o
hormônio luteinizante [LH]
e o folículo-estimulante
[FSH]).
O desenvolvimento da
glândula hipofisária e a
origem dos tipos celulares
distintos a partir de células
primordiais comuns é
controlado por conjunto
limitado de fatores
transcricionais, mais
precisamente Prop1 e Pit 1.
As células individuais
secretoras de hormônios originam-se em uma ordem específica de
linhagens distintas. Anormalidades dos fatores de transcriçãodahipófise
e específicos da linhagem têm sido associadas ao desenvolvimento de
hipopituitarismo. Hipopituitarismo é uma doença endócrina
caracterizada pela diminuição da secreção de um ou mais dos oito](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a BAIXA ESTATURA/CRESCER:IMPORTÂNCIA ÍMPAR DA ADENO-HIPÓFISE CRESCIMENTO DE CRIANÇA/INFANTIL/JUVENIL.
Semelhante a BAIXA ESTATURA/CRESCER:IMPORTÂNCIA ÍMPAR DA ADENO-HIPÓFISE CRESCIMENTO DE CRIANÇA/INFANTIL/JUVENIL. (20)
Mais de Van Der Häägen Brazil
Mais de Van Der Häägen Brazil (20)
Último
Último (8)
BAIXA ESTATURA/CRESCER:IMPORTÂNCIA ÍMPAR DA ADENO-HIPÓFISE CRESCIMENTO DE CRIANÇA/INFANTIL/JUVENIL.
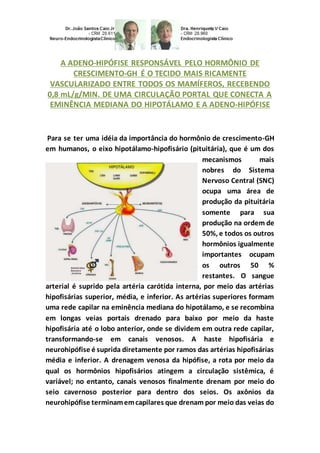
- 1. A ADENO-HIPÓFISE RESPONSÁVEL PELO HORMÔNIO DE CRESCIMENTO-GH É O TECIDO MAIS RICAMENTE VASCULARIZADO ENTRE TODOS OS MAMÍFEROS, RECEBENDO 0,8 mL/g/MIN. DE UMA CIRCULAÇÃO PORTAL QUE CONECTA A EMINÊNCIA MEDIANA DO HIPOTÁLAMO E A ADENO-HIPÓFISE Para se ter uma idéia da importância do hormônio de crescimento-GH em humanos, o eixo hipotálamo-hipofisário (pituitária), que é um dos mecanismos mais nobres do Sistema Nervoso Central (SNC) ocupa uma área de produção da pituitária somente para sua produção na ordem de 50%, e todos os outros hormônios igualmente importantes ocupam os outros 50 % restantes. O sangue arterial é suprido pela artéria carótida interna, por meio das artérias hipofisárias superior, média, e inferior. As artérias superiores formam uma rede capilar na eminência mediana do hipotálamo, e se recombina em longas veias portais drenado para baixo por meio da haste hipofisária até o lobo anterior, onde se dividem em outra rede capilar, transformando-se em canais venosos. A haste hipofisária e neurohipófise é suprida diretamente por ramos das artérias hipofisárias média e inferior. A drenagem venosa da hipófise, a rota por meio da qual os hormônios hipofisários atingem a circulação sistêmica, é variável; no entanto, canais venosos finalmente drenam por meio do seio cavernoso posterior para dentro dos seios. Os axônios da neurohipófise terminamemcapilares que drenam por meio das veias do
- 2. lobo posterior e dos seios cavernosos para a circulação geral. O sistema porta-hipofisário dos capilares permite controlar a função da adeno- hipófise por meio dos hormônios hipotalâmicos hipofiotróficos, secretados para dentro dos vasos porta-hipofisários. Isso fornece uma conexão curta e direta com a adeno-hipófise a partir do hipotálamo ventral e da eminência mediana. Também pode existir fluxo retrógado entre a hipófise e o hipotálamo, dando origem a um possível mecanismo de feedback direto entre os hormônios hipofisários e seus centros de controle neuroendócrinos. Atualmente, técnicas imunocitoquímicas e de microscopia eletrônica permitiram a classificação das células por meio de seus produtos secretórios específicos: células somatotrópicas (que secretam hormônios de crescimento [GH]), células lactotróficas (que secretam prolactina [PRL]), células tireotróficas (que secretam tireotrofina [TRH]), células corticotróficas (que secretam ACTH e peptídeos relacionados) e células gonadotróficas (que secretam o hormônio luteinizante [LH] e o folículo-estimulante [FSH]). O desenvolvimento da glândula hipofisária e a origem dos tipos celulares distintos a partir de células primordiais comuns é controlado por conjunto limitado de fatores transcricionais, mais precisamente Prop1 e Pit 1. As células individuais secretoras de hormônios originam-se em uma ordem específica de linhagens distintas. Anormalidades dos fatores de transcriçãodahipófise e específicos da linhagem têm sido associadas ao desenvolvimento de hipopituitarismo. Hipopituitarismo é uma doença endócrina caracterizada pela diminuição da secreção de um ou mais dos oito
- 3. hormônios normalmente produzidos pela glândula pituitária (hipófise), na base do cérebro. Se há diminuição da maioria dos hormônios pituitários, é usado o termo pan-hipopituitarismo. Os sinais e sintomas da doença variam de acordo com os hormônios afetados e a causa primária da anormalidade. O diagnóstico é feito através de exames de sangue, mas geralmente são necessários exames específicos e outras vistorias para que sejam identificadas as causas primárias e o tratamento a ser adotado. Os hormônios da glândula pituitária têm diferentes funções no corpo humano e, portanto, os sintomas do hipopituitarismodependemde qual hormônio é deficiente. Os sintomas podem ser sutis e a princípio são geralmente atribuídas a outras causas. Na maioria dos casos, três ou mais hormônios são deficientes. O problema mais comum é a insuficiência de hormônio do crescimento (GH)/de folículo-estimulante (FSH) e/ou do hormônio luteinizante (LH) levando a anormalidades no desenvolvimento sexual. A deficiência do hormônio do crescimento é mais comum em pessoas (humanos). A apoplexia, além de causar dor de cabeça e rápida perda de capacidade visual, pode também ser associada com a visão dupla, caso ocorra compressão dos nervos no seio cavernoso que controlam os músculos dos olhos. Na verdade a doença mais frequente (patologia) é a deficiência de GH–hormônio de crescimento, que leva à baixa estatura (altura) longitudinal, linear por deficiência de crescimento em criança, infantil, juvenil ou adolescente que tem comprometimento vitalício quando não tratada, em outras palavras, além dos problemas orgânicos não podemos nos esquecer dos problemas biopsicossociais de crianças até a fase adulta. Mas como vimos, em geral, devidoao entrelaçamentode todos os vasos arteriais e venosos mecanismos
- 4. locais de feedback e sistemas neurais secretores neuroendócrinos, em geral não são comprometidos apenas de um loco específico, mas simno geral, mais de três substâncias sãoenvolvidas nas disfunções de comando (neurotransmissoras) oureceptoras oque levaa um comprometimentodesastrosoquandonão são tomadas atitudes terapêuticaimediatas quandoindicadas e no tempoe no instante certos, como mostra a práticae pesquisas médicas. LOW HEIGHT/GROWTH:IMPORTANCEODD ANTERIOR PITUITARY IN GROWTH OF CHILD / CHILDREN / YOUTH. THE ANTERIOR PITUITARY RESPONSIBLEBY GROWTH HORMONE-GH IS MOREFABRIC HIGHLY VASCULARIZED AMONG ALL MAMMALS, RECEIVING 0.8 ML/G/MIN. PORTAL OF A MOVEMENTTHATCONNECT THE MEDIAN EMINENCETHEHYPOTHALAMUS AND ANTERIOR PITUITARY. PHYSIOLOGY-ENDOCRINOLOGY-NEUROENDOCRINOLOGY- GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISIONOF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO. To get an ideaof the importance of growth hormone-GH inhumans, the hypothalamic-pituitary axis (pituitary), whichis one of the noblest mechanisms of central nervous system(CNS) occupies aproductionarea of the pituitary only for its productionon the order of 50%, and all other important hormones occupy the other 50% remaining. Arterial bloodis suppliedby the internal carotidartery throughthe upper, middle, and inferior hypophyseal arteries. The upper arteries formacapillary network in the medianeminence of hypothalamus and recombines into long portal veins draindown through the shank tothe anterior pituitary lobe, where they divide capillary network toanother, turning invenous channels.
- 5. The pituitary stalk andneurohypophysis is directly supplied by branches of the middle and inferior hypophyseal arteries. The venous drainage of the pituitary, the route through which the pituitary hormones reach the systemic circulation, is variable; however, venous channels eventually drain through the cavernous sinus further into the sinuses. The axons terminate in the neurohypophysis capillaries that drain throughthe veinand the posterior lobe of the cavernous sinus into the general circulation. The door-pituitary system of capillaries allows controlling the function of the anterior pituitary through hypophisiotrofics hypothalamic hormones, secreted into the door- pituitary vessels. This provides a short and direct connection to the anterior pituitary from the ventral hypothalamus and the median eminence. There may also be retrograde flow from the pituitary gland and the hypothalamus, resulting in a possible means of direct feedback betweenpituitary hormones and their centers, neuroendocrine control. Currently, Immunocytochemical and Electron Microscopy Techniques allow the classificationof cells throughtheir specific secretory products: somatotropic cells (which secrete growth hormone [GH]), lactotrophics cells (which secrete prolactin [PRL]), thyrotrophics cells (which secrete thyrotrophin [TRH]), corticotrophics cells (which secrete ACTH and related peptides) and gonadotrophics cells (which secrete luteinizing hormone [LH] and follicle-stimulating hormone [FSH]). The development of the pituitary gland and the origin of cell types distinct from common primordial cells is controlledby limitedset of transcription factors, more
- 6. precisely Prop 1 and Pit 1. Secretory cells of individual hormones originate in a specific order of strains distinct. Abnormalities of the pituitary transcriptionand lineage-specific factors have been associated with the development of hypopituitarism. Hypopituitarism is an endocrine disorder characterizedby decreased secretion of one or more of the eight hormone normally produced by the pituitary (hypophyses), the base of the brain. If there is a reduction of most pituitary hormones, the term used is panhypopituitarism. Signs and symptoms vary according to the affected hormones and the primary cause of the abnormality. The diagnosis is made by blood tests, but specific tests are usually neededfor surveys and other primary causes, so the symptoms are identified and the treatment to be adopted. The pituitary gland hormones have different functions in the human body and hypopituitarism dependon which hormone is deficient. Symptoms may be subtle at first and are usually attributed to other causes. In most cases, three or more hormones are disabled. The most common problem is the lack of growth hormone (GH), follicle-stimulating hormone (FSH) and/or luteinizing hormone (LH) leading to abnormalities in sexual development. A deficiency of growth hormone is more common in people (human). Stroke and cause headache and rapid loss of vision, you may also be associated with double vision, if it occurs compression of the cavernous sinus nerves that control the eye muscles. Infact the most common disease (pathology) is the deficiency of GH-growth hormone, which leads tostunted(height) longitudinal or linear growth in children, infant, child or adolescent who has lifelong commitment disability if not
- 7. treated, inother words, beyond the physical problems we cannot forget the biopsychosocial problems of children into adulthood. But as we saw in general due to entanglement or imbrication of all arterial and venous vessels local feedback mechanisms andneuroendocrine secretory neural systems in general is not only committed to a specific place, but more generally over three substances are involved in the dysfunctions control neurotransmitter or receptor and which leads to a disastrous engagement when not taken immediate therapeutic action when indicated and certain moment in time and as shown in practice and medical research. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna CRM 28930 Como saber mais: 1. Baixaestaturalongitudinal oulinear:mesmona ausênciade restrição nutricional ou nanismopsicossocial completo, as interaçõesnegativas em uma família podem inibir o crescimentode criança, infantil e juvenil. É essencial levar emconsideraçãoadinâmica familiar na avaliação de uma criançacom crescimentoinadequado... http://hormoniocrescimentoadultos.blogspot.com 2. Bowlby (Edward John MostynBowlby foi um psicólogo, psiquiatrae psicanalistabritânico, notável por seuinteressenodesenvolvimento infantil e por seutrabalho pioneirona teoriado apego) reuniutal evidênciaempíricacomoexistianaépoca em toda a Europa e nos EUA, incluindoSpitz (1946) e Goldfarb(1943 1945)... http://longevidadefutura.blogspot.com
- 8. 3. Suas principais conclusões, que "lactentese crianças devem experimentar umarelaçãocalorosa, íntimae contínuacom a mãe (ou mãe substitutapermanente, babá) em que ambos encontramsatisfação e prazer", e quem não fazê-lopode ter significativas e irreversíveis consequências mentais paraa saúde, eram ambos controversos e influentes... http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Heinrichs C, Munson PJ, Counts DR, et al.: Patterns of human growth. Science.268: 442-447 1995; Lampl M, Veldhuis JD, Johnson ML: Saltation and stasis: a model of human growth.Science. 258: 801-803 1992; LamplM, Cameron N, Veldhuis JD, et al.: Patterns of human growth: response.Science. 268:445-447 1995; Tillmann V, Thalange NK, Foster PJ, et al.: The relationship between stature, growth, and short-term changes in height and weight in normal prepubertal children. Pediatr Res. 44:882-886 1998 ; Thalange NK, Foster PJ, Gill MS, et al.: Model of normal prepubertal growth. Arch Dis Child. 75:427-431 1996; Gelander L, Karlberg J, Albertsson -Wikland K: Seasonality in lower leg length velocity in prepubertal children. Acta Paediatr. 83:1249-1254 1994; Hermanussen M, Lange S, Grasedyck L: Growth tracks in early childhood. Acta Paediatr. 90:381-386 2001; Ogden CL, Kuczmarski RJ, Flegal KM, et al.: Centers for Disease Control and Prevention 2000 growth charts for the United States: improvements to the 1977 National Center for Health Statistics version. Pediatrics. 109:45-60 2002; Tanner JM, Davies PS: Clinical longitudinal standards for height and height velocity for North American children. J Pediatr. 107: 317-329 1985; Lyon AJ, Preece MA, Grant DB: Growth curve for girls with Turner syndrome. Arch Dis Child. 60:932-935 1985; Horton WA, Rotter JI, Rimoin DL, et al.: Standard growth curves for achondroplasia.J Pediatr. 93: 435-438 1978; CronkC, Crocker AC, Pueschel SM, et al.: Growth charts for children with Down syndrome: 1 month to 18 years of age. Pediatrics. 81:102-110 1988; Bayer LM, Bayley L: Growth Diagnosis: Selected Methods for Interpreting and Predicting Physical Development from One Year to Maturity. 1959 University of Chicago Press Chicago. Contato: Fones: 55 11 5087-4404 ou96197-0305 Nextel: ID:111*101625
- 9. Rua Estela, 515 - BlocoD - 12ºandar - Conj. 121/122 Paraiso - São Paulo - SP - Cep 04011-002 e-mails:drcaio@vanderhaagenbrasil.com drahenriqueta@vanderhaagenbrasil.com vanderhaagen@vanderhaagenbrasil.com Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr Video http://youtu.be/woonaiFJQwY Google Maps: http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl= pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie =UTF8&ll=-23.575591,- 46.650481&spn=0,0&t = h&z=17