O documento descreve o coma, suas causas, mecanismos, avaliação e tratamento. As principais informações são:
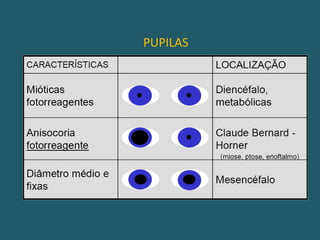
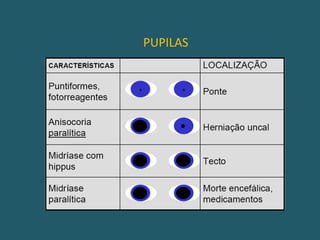
1) O coma é uma síndrome decorrente de lesões cerebrais difusas ou localizadas no tronco cerebral ou córtex;
2) As causas mais comuns são lesões metabólicas (65%) seguidas de lesões supratentoriais (20%) e infratentoriais (13%);
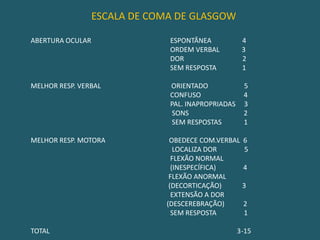
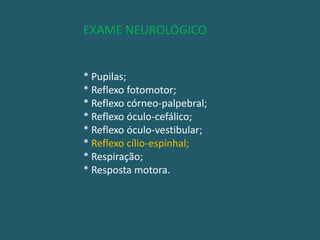
3) A avaliação inclui exame físico, escala de Glasgow, exames de imagem e laboratoriais para identificar










































![Exame neuro infantil[1].2](https://cdn.slidesharecdn.com/ss_thumbnails/exameneuroinfantil1-2-120322123912-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)










































