Hypothalamus role in growth and development through neuroendocrinology
•
0 gostou•188 visualizações

O documento discute a importância do hipotálamo em relação aos hormônios, incluindo o hormônio do crescimento. O hipotálamo regula funções não endócrinas como a temperatura corporal e ingestão de alimentos, e está conectado a outras partes do sistema nervoso. Hormônios atravessam a barreira hematoencefálica e afetam o cérebro. A glândula pituitária é controlada pelo hipotálamo e regula outros órgãos através de hormônios.

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Hypothalamus role in growth and development through neuroendocrinology
Semelhante a Hypothalamus role in growth and development through neuroendocrinology (20)
Mais de Van Der Häägen Brazil
Mais de Van Der Häägen Brazil (20)
Último
Último (11)
Hypothalamus role in growth and development through neuroendocrinology
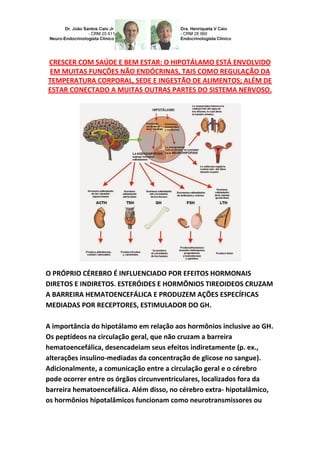
- 1. CRESCER COM SAÚDE E BEM ESTAR: O HIPOTÁLAMO ESTÁ ENVOLVIDO EM MUITAS FUNÇÕES NÃO ENDÓCRINAS, TAIS COMO REGULAÇÃO DA TEMPERATURA CORPORAL, SEDE E INGESTÃO DE ALIMENTOS; ALÉM DE ESTAR CONECTADO A MUITAS OUTRAS PARTES DO SISTEMA NERVOSO. O PRÓPRIO CÉREBRO É INFLUENCIADO POR EFEITOS HORMONAIS DIRETOS E INDIRETOS. ESTERÓIDES E HORMÔNIOS TIREOIDEOS CRUZAM A BARREIRA HEMATOENCEFÁLICA E PRODUZEM AÇÕES ESPECÍFICAS MEDIADAS POR RECEPTORES, ESTIMULADOR DO GH. A importância do hipotálamo em relação aos hormônios inclusive ao GH. Os peptídeos na circulação geral, que não cruzam a barreira hematoencefálica, desencadeiam seus efeitos indiretamente (p. ex., alterações insulino-mediadas da concentração de glicose no sangue). Adicionalmente, a comunicação entre a circulação geral e o cérebro pode ocorrer entre os órgãos circunventriculares, localizados fora da barreira hematoencefálica. Além disso, no cérebro extra- hipotalâmico, os hormônios hipotalâmicos funcionam como neurotransmissores ou
- 2. neurohormônios. Também são encontrados em outros tecidos, onde funcionam como hormônios (endócrinos, parácrinos ou autócrinos). Algumas características são únicas em humanos, que fazem toda a diferença, pois o hipotálamo está ligado à hipófise pelo núcleo arqueado; o tamanho da glândula hipofisária, constituída em 2/3 pelo lobo anterior, varia consideravelmente. Mede aproximadamente 15,10 e 6 mm e pesa de 500 a 900 mg; pode dobrar de tamanho durante a gestação. A sela túrcica tende a se igualar ao tamanho e ao formato da glândula e, por essa razão, apresenta um contorno bastante variável. Suprimento sanguíneo: a adeno-hipófise é o tecido mais ricamente vascularizado entre todos os tecidos dos mamíferos, recebendo 0,8 mL/g/min de uma circulação portal que conecta a eminência mediana do hipotálamo e a adeno-hipófise. O sangue arterial é suprida pela artéria carótida interna, por meio das artérias hipofisárias superior, média e inferior. As artérias hipofisárias superiores formam uma rede capilar na eminência mediana do hipotálamo, que se recombina em longas veias portais drenando para baixo por meio da haste hipofisária até o lobo anterior, onde se dividem em outra rede capilar, transformando-se em canais venosos. A haste hipofisária e a neuro-hipófise são supridas diretamente por ramos das artérias hipofisárias média e inferior. A
- 3. drenagem venosa da hipófise, a rota por meio da qual os hormônios hipofisários atingem a circulação sistêmica, é variável; no entanto, canais venosos finalmente drenam por meio do seio cavernoso posterior para dentro dos seios petrosos superiores e inferior para o bulbo e a veia jugular. Os axônios da neuro-hipófise terminam em capilares que drenam por meio das veias do lobo posterior e dos seios cavernosos para a circulação geral. O sistema porta-hipofisário dos capilares permite controlar a função da adeno-hipófise por meio dos hormônios hipotalâmicos hipofisiotróficos, secretados para dentro dos vasos porta- hipofisários. Isso fornece uma conexão curta e direta com a adeno- hipófise a partir do hipotálamo ventral e da eminência mediana. Também pode existir fluxo retrógrado entre a hipófise e o hipotálamo, dando origem a um possível meio de feedback direto entre os hormônios hipofisários e seus centros de controle neuroendócrino. Desenvolvimento e histologia da hipófise: as células da adeno-hipófise foram originalmente classificadas como células acidófilas, basófilas e cromófobas, com base na coloração com hematoxilina e eosina. Atualmente, técnicas imunocitoquímicas e de microscopia eletrônica permitiram a classificação das células por meio de seus produtos secretórios específicos: as células somatotróficas (que secretam hormônio de crescimento [GH]), as células lactotróficas (que secretam prolactina [PRL]), as células tireotróficas (que secretam tireotrofina [TSH]), as células corticotróficas (que secretam ACTH e peptídeos relacionados) e as células gonadotróficas (que secretam o hormônio luteinizante [LH] e o hormônio folículo-estimulante [FSH]).
- 4. O desenvolvimento da glândula hipofisária e a origem dos tipos celulares distintos a partir de células primordiais comuns é controlado por um conjunto limitado de fatores de transcrição, mais precisamente Prop 1 e Pit 1. As células individuais secretoras de hormônios originam-se em uma ordem específica e de linhagens distintas. Anormalidades dos fatores de transcrição da hipófise e específicos da linhagem têm sido associadas ao desenvolvimento de hipopituitarismo. Embora tradicionalmente a hipófise tenha sido concebida como uma glândula com células distintas e altamente especializadas que respondem a hormônios hipotalâmicos e periféricos específicos tornou- se claro que fatores locais (isto é, parácrinos) também desempenham um papel na fisiologia da hipófise normal. O valor significativo da adeno hipófise está diretamente proporcional à importância do GH à tal nível, que o GH representa 50% do volume de produção desta substância responsável pelo crescimento longitudinal em humanos. O GH está interligado a diversas substâncias imprescindíveis para o desenvolvimento humano, como por ex.: variantes tanto das subunidades α quanto β estão presentes na placenta, músculo e cérebro. Essas variantes podem explicar estudos de ligação competitivos anômalos. O mecanismo molecular para a formação de certos receptores ainda não foi identificado, nem é claro se eles se ligam diferenciadamente ao IGF-1, IGF-2 ou insulina. A formação de receptores
- 5. do IGF tipo 1 híbridos que contêm um hemirreceptor α-IGF ligado dissulfidricamente a um hemirreceptor α-insulina parece ser dependente do ligante, e estudos com anticorpos monoclonais específicos para insulina ou receptor do IGF tipo 1 sugerem que esses receptores se desenvolvem em células com receptores nativos abundantes, como os músculos e a placenta. Esses híbridos têm uma afinidade perto da normal para IGF-1, porém diminuída para insulina. A significância fisiológica desses receptores híbridos é desconhecida. GROW FROM PRENATAL PHASE, CHILD, INFANT, YOUTH, TEENS, PUBERTY, TO ADULT - NEUROENDOCRINOLOGY: THE HYPOTHALAMUS AS PART OF A LARGER SYSTEM. GROW WITH HEALTH AND WELFARE: THE HYPOTHALAMUS IS NOT INVOLVED IN MANY ENDOCRINE FUNCTIONS, SUCH AS TEMPERATURE REGULATING BODY, SEAT AND FOOD INTAKE; BESIDES BEING CONNECTED TO MANY OTHER PARTS OF THE NERVOUS SYSTEM. OWN BRAIN IS HORMONE EFFECTS INFLUENCED BY DIRECT AND INDIRECT. STEROIDS AND THYROID HORMONES CROSSE BLOOD-BRAIN BARRIER AND PRODUCE SPECIFIC ACTIONS MEDIATED BY RECEPTORS,
- 6. STIMULATOR OF GH. PHYSIOLOGY-ENDOCRINOLOGY,
- 8. (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO. The importance of the hypothalamus in relation to hormones including GH. The peptides in the general circulation, which do not cross the blood-brain barrier, triggering its effects indirectly (p. ex., insulin- mediated changes in blood glucose concentration). Additionally, communication between the general circulation and the brain may occur between the circumventricular organs, which are located outside the blood brain barrier. Furthermore, the extra-hypothalamic brain, hypothalamic hormones act as neurohormones or neurotransmitters. Are also found in other tissues, where they function as hormones (endocrine, paracrine or autocrine). Some features are unique to humans, who make all the difference, because the hypothalamus is linked to the pituitary gland arcuate nucleus; the size of the pituitary gland, formed by two-thirds by the anterior lobe varies considerably. Measures approximately 15, 10 and 6 mm and weighs 500-900 mg; can double in size during pregnancy. The sella turcica tends to match the size and shape of the gland and, therefore, has a quite variable contour. The blood supply to the anterior pituitary is the most richly vascularized tissue between all mammalian tissues, receiving 0.8 mL/g/min of a portal circulation that connects the median eminence of the hypothalamus and the anterior pituitary.
- 9. Arterial blood is supplied by the internal carotid artery, through the upper, middle and lower pituitary arteries. The superior hypophyseal artery form a capillary network in the median eminence of hypothalamus, which recombines long portal veins draining down through the shank to the pituitary anterior lobe, where they divide into another capillary network, becoming venous channels. The pituitary stalk and neurohypophysis are supplied directly by branches of the middle and inferior hypophyseal arteries. The venous drainage from the pituitary, the route through which the pituitary hormones reach the systemic circulation, is variable; however, eventually draining venous channels through the posterior cavernous sinus into the superior and inferior petrosal sinuses to the bulb and the jugular vein. The axons of the neurohypophysis end in capillaries that drain through the lobe and the posterior veins of the cavernous sinus into the general circulation. The door-pituitary system of capillaries allows you to control the function of the anterior pituitary through hipophisiotrofics hypothalamic hormones, secreted into the door-pituitary vessels. This provides a short and direct connection to the anterior pituitary from the ventral hypothalamus and the median eminence. There may also be retrograde flow from the pituitary gland and the hypothalamus, resulting in a possible means of direct feedback between pituitary hormones and their centers neuroendocrine control. Development and histology the anterior pituitary cells were originally classified as acidophilic cells, basophilic and cromófobas based on staining with hematoxylin and eosin. Currently, immunocytochemistry and electron microscopy techniques allow the classification of cells through their specific secretory products: somatotroph cells (which secrete growth [GH] hormone) lactotrophics cells (which secrete prolactin [PRL]), tireotrophics cells (which secrete thyrotropin [TSH]),
- 10. corticotrophics cells (which secrete ACTH and related peptides) and gonadotropic cells (which secrete luteinizing hormone [LH] and follicle- stimulating hormone [FSH]). The development of the pituitary gland and the origin of cell types distinct from common primordial cells is controlled by a limited set of transcription factors, specifically Prop 1 and Pit 1. The individual cells secreting hormones originate in a specific order and distinct lineages. Abnormalities of transcription and pituitary lineage-specific factors have been associated with the development of hypopituitarism. Although traditionally has been designed pituitary gland as a distinct and highly specialized cell that respond to specific hypothalamic hormones and peripheral, it became clear that local factors (e.g., paracrine) also play a role in the physiology of normal pituitary gland. The significant value of adeno hypophyses is directly proportional to the importance of GH to such a level, that GH is 50% of the production volume of the substance responsible for longitudinal growth in humans. GH this interconnected to various substances essential for human development, for ex.; variants of both α and β subunits as are present in the placenta, muscle and brain. These variants may explain anomalous competitive binding studies. The molecular mechanism for the formation of certain receptor has not been identified, nor is it clear whether they differentially bind to IGF-1, IGF-2 or insulin.
- 11. The formation of type 1 IGF receptors that contain a hybrid α-IGF hemirreceptor connected to a dissulfidricamente hemirreceptor α- insulin appears to be dependent on the binder and studies with monoclonal antibodies specific for insulin or type 1 IGF receptor suggest that these receptors are developed cells with abundant native receptors, such as muscle and placenta. These hybrids have an affinity near the normal IGF-1, but decreased to insulin. The physiological significance of this hybrid receptor is unknown. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna CRM 28930 Como saber mais: 1. Hoje, o hormônio do crescimento humano (hGH) é aprovado pelo FDA para o tratamento de baixa estatura devido à síndrome de Turner, insuficiência renal crônica, retardo de crescimento intrauterino, síndrome de Prader-Willi, baixa estatura familiar ou idiopática grave e este fato tomou corpo a partir de meados da década de 1980 até começo de 1990.... http://hormoniocrescimentoadultos.blogspot.com 2. Com o advento da tecnologia de preparação dessa substância biológica necessária e que todos temos em nossos organismos, através da engenharia genética onde se aplica a técnica de DNA–recombinante com a retirada do fator de reconhecimento do DNA a quem pertenciam os códigos, evitando o maior entrave que era a formação de príons, proteína anômala que se podia estabelecer mesmo que raramente e desenvolver a Doença de Creutzfeldt-Jakob (DCJ) que através de uma
- 12. enzima promovia a retirada do fator de conhecimento à quem pertencia o DNA anômalo... http://longevidadefutura.blogspot.com 3. A partir de então o GH passou a ser destingido como GH rDNA, e elevou essa doença provocada por incompatibilidade na rejeição do DNA humano para crescimento a uma condição basicamente desprezível por praticamente anular essa patologia (doença) que até então era um problema... http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Rasier G, Parent AS, Gérard A, Lebrethon MC, Bourguignon JP 2007 Early maturation of gonadotropin-releasing hormone secretion and sexual precocity after exposure of infantile female rats to estradiol or dichlorodiphenyltrichloroethane. Biol Reprod 77:734–742; Li S, Hursting SD, Davis BJ, McLachlan JA, Barrett JC 2003 Environmental exposure, DNA methylation and gene regulation. Lessons from diethylstilbestrol-induced cancers. Ann NY Acad Sci 983:161–169; McLachlan JA, Simpson E, Martin M 2006 Endocrine disrupters and female reproductive health. Best Pract Res Clin Endocrinol Metab 20:63–75; Darbre PD 2006 Environmental oestrogens, cosmetics and breast cancer. Best Pract Res Clin Endocrinol Metab 20:121–143; Fenton SE 2006 Endocrine-disrupting compounds and mammary gland development: Early exposure and later life consequences. Endocrinology 147:S18–S24; Newbold RR, Jefferson WN, Padilla-Banks E 2007 Long-term adverse effects of neonatal exposure to bisphenol A on the murine female reproductive tract. Reprod Toxicol 24:253–258; Crews D, McLachlan JA 2006 Epigenetics, evolution, endocrine disruption, health, and disease. Endocrinology 147:S4–S10; Anway MD, Skinner MK 2008 Transgenerational effects of the endocrine disruptor vinclozolin on the prostate transcriptome and adult onset disease. Prostate 68:517–529; Anway MD, Cupp AS, Uzumcu M, Skinner MK 2005 Epigenetic transgenerational actions of endocrine disruptors and male fertility. Science 308:1466–1469; Christiansen S, Scholze M, Axelstad M, Boberg J, Kortenkamp A, Hass U 2008 Combined exposure to anti-androgens causes markedly increased frequencies of hypospadias in the rat. Int J Androl 31:241–248; Shono T, Suita S, Kai H, Yamaguchi Y 2004 Short-time exposure to vinclozolin in utero induces testicular maldescent associated with a spinal nucleus alteration of the genitofemoral nerve in rat. J Pediatr Surg 39:217–219; Monosson E, Kelce WR, Lambright C, Ostby J, Gray Jr LE 1999 Peripubertal exposure to the antiandrogenic fungicide, vinclozolin, delays puberty, inhibits the development of androgen-dependent tissues, and alters androgen receptor function in the male rat. Toxicol Ind Health 15:65–79; Newbold RR, Hanson RB, Jefferson WN, Bullock BC, Haseman J, McLachlan JA 1998 Increased tumors but uncompromised fertility in the female descendants of mice exposed developmentally to diethylstilbestrol. Carcinogenesis 19:1655–1663; Kadlubar FF, Berkowitz GS, Delongchamp RR, Wang C, Green BL, Tang G, Lamba J, Schuetz E, Wolff MS 2003 The CYP3A4*1B variant is related to the onset of puberty, a known risk factor for the development of breast cancer. Cancer Epidemiol Biomarkers Prev 12:327–331. Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com
- 13. www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr google.com/+JoãoSantosCaioJrvdh google.com/+VANDERHAAGENBRAZILvdh Video http://youtu.be/woonaiFJQwY VAN DER HAAGEN BRAZI Instagram https://instagram.com/clinicascaio/ Google Maps: http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl=pt&sll=- 23.578256,46.645653&sspn=0.005074,0.009645&ie =UTF8&ll=-23.575591,-46.650481&spn=0,0&t = h&z=17