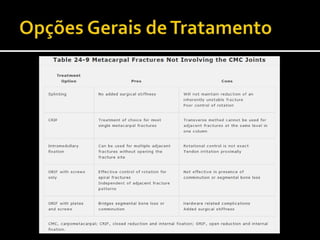
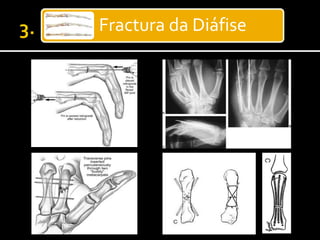
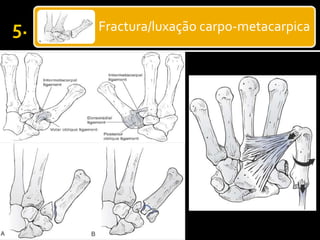
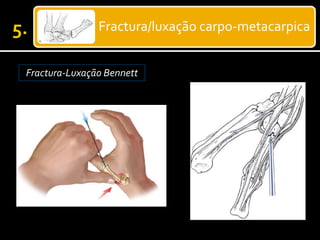
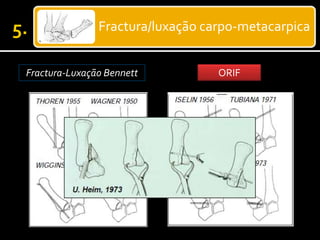
Este documento discute as fraturas dos ossos da mão, incluindo as falanges, metacarpos e ossos do carpo. Ele fornece detalhes sobre os tipos de fraturas, causas, avaliação, tratamento cirúrgico e conservador, e complicações possíveis. O objetivo do tratamento é recuperar a função da mão de forma segura e efetiva.


















![Fraturas dos membros_superiores[1]](https://cdn.slidesharecdn.com/ss_thumbnails/fraturasdosmembrossuperiores1-140305134800-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


























































