Estrogênio estimula secreção de GH em criança e jovem
•Transferir como DOCX, PDF•
1 gostou•1,134 visualizações

O documento discute o papel do estrógeno na liberação do hormônio do crescimento (GH) em células da pituitária anterior em crianças, adolescentes e jovens. O estrógeno pode potencializar a liberação de GH e modular sua ação de forma independente da secreção. Isso tem implicações para o crescimento e desenvolvimento durante a puberdade.

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Estrogênio estimula secreção de GH em criança e jovem
Semelhante a Estrogênio estimula secreção de GH em criança e jovem (20)
Mais de Van Der Häägen Brazil
Mais de Van Der Häägen Brazil (20)
Estrogênio estimula secreção de GH em criança e jovem
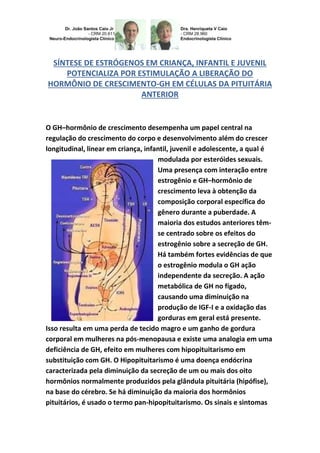
- 1. SÍNTESE DE ESTRÓGENOS EM CRIANÇA, INFANTIL E JUVENIL POTENCIALIZA POR ESTIMULAÇÃO A LIBERAÇÃO DO HORMÔNIO DE CRESCIMENTO-GH EM CÉLULAS DA PITUITÁRIA ANTERIOR O GH–hormônio de crescimento desempenha um papel central na regulação do crescimento do corpo e desenvolvimento além do crescer longitudinal, linear em criança, infantil, juvenil e adolescente, a qual é modulada por esteróides sexuais. Uma presença com interação entre estrogênio e GH–hormônio de crescimento leva à obtenção da composição corporal específica do gênero durante a puberdade. A maioria dos estudos anteriores têm- se centrado sobre os efeitos do estrogênio sobre a secreção de GH. Há também fortes evidências de que o estrogênio modula o GH ação independente da secreção. A ação metabólica de GH no fígado, causando uma diminuição na produção de IGF-I e a oxidação das gorduras em geral está presente. Isso resulta em uma perda de tecido magro e um ganho de gordura corporal em mulheres na pós-menopausa e existe uma analogia em uma deficiência de GH, efeito em mulheres com hipopituitarismo em substituição com GH. O Hipopituitarismo é uma doença endócrina caracterizada pela diminuição da secreção de um ou mais dos oito hormônios normalmente produzidos pela glândula pituitária (hipófise), na base do cérebro. Se há diminuição da maioria dos hormônios pituitários, é usado o termo pan-hipopituitarismo. Os sinais e sintomas
- 2. da doença variam de acordo com os hormônios afetados e a causa primária da anormalidade. O diagnóstico é feito através de exames de sangue, mas geralmente são necessários exames específicos e outras vistorias para que sejam identificadas as causas primárias e o tratamento a ser adotado. As sequelas metabólicas negativas são potencialmente importantes por causa do uso generalizado de estrogênio oral e compostos relacionados com o estrogênio. O estrógeno afeta a ação do GH no nível de expressão do receptor e sinalização. Mais recentemente, o estrogênio tem demonstrado inibir a quinase Janus transdutor/sinal e ativador de transcrição da sinalização por GH através da indução de supressor de sinalização 2-citoquina, um inibidor da proteína de sinalização de citocinas. Isso representa um novo paradigma da regulação esteróide de receptores de citocinas e é provável que tenha significado para uma gama diversificada de função de citocinas. Porque Janus; Janus quinase (JAK) é uma família de não receptores tirosina-quinases intracelular, que traduzem sinais de citocinas mediadas por via da JAK- STAT. Eles foram inicialmente denominados "apenas outra quinase" 1 e 2 (uma vez que eles foram apenas dois de um grande número de descobertas em uma pesquisa baseada em PCR de quinases), mas acabaram por ser publicadas como "Janus quinase". O nome é retirado do deus Romano com duas caras com começos e fins, Janus, porque os JAKs possuem dois domínios de transferência de fosfato quase idênticas. Um domínio exibe a atividade de quinase, enquanto a outra regula negativamente a atividade de quinase do primeiro. Em bioquímica, uma cinase ou quinase, é um tipo de enzima
- 3. que transfere grupos fosfatos de moléculas doadoras de alta energia (como o ATP) para moléculas-alvo específicas (substratos). O processo tem o nome de fosforilação. A molécula-alvo pode ativar-se ou inativar- se mediante a fosforilação. Todas as cinases necessitam de um íon metálico divalente como o Mg2+ ou o Mn2+ para transferir o grupo fosfato. Estas enzimas são ativadas pelo AMP cíclico, que catalisa a fosforilação de determinadas proteínas. Além dessas posições logísticas o que fica marcado entre a secreção do estrógeno e o GH é a rota estrogênica, entretanto, exerce marcada influência sobre o eixo de hormônio de crescimento/fator de crescimento insulina-símile número 1 (GH/IGF-1), no entanto, existe a necessidade de avaliação detalhada para que não comprometa a massa corporal principalmente em criança, infantil e juvenil. Estrógenos e ação do GH: efeitos estrogênicos sobre o eixo GH/IGF-1; O GH regula o crescimento e a composição corporal por meio de um processo complexo que combina ações mitogênicas e metabólicas, que utilizam mecanismos dependentes e independentes de IGF-1. O fígado tem papel importante nesse processo metabólico, pois é um órgão-alvo na ação do GH, responsável pelos níveis séricos de IGF-1 e também órgão-alvo dos hormônios sexuais. Os estrógenos são responsáveis pelo desenvolvimento sexual secundário e têm papel fundamental na função reprodutiva feminina. Existe relação estreita entre os estrógenos e o GH na regulação do crescimento e do desenvolvimento na puberdade, este é um dos motivos que eventualmente sugira ser indicado para fins de crescimento
- 4. longitudinal ou linear em criança, infantil ou juvenil e mesmo adolescente, o auxílio de inibidores da aromatase se tiver indicação precisa. ESTROGEN INCREASES THE SECRETION OF GH IN RESPONSE TO STIMULATION: CHILD AND YOUTH. THE STIMULATION OF GROWTH HORMONE RELEASE-GH AND SUMMARY ESTROGEN IN CHILD, INFANT AND JUVENILE, THE POTENTIAL EFFECT OF ESTROGEN IN CONTROL OF GH SECRETION IN ANTERIOR PITUITARY CELLS: PHYSIOLOGY-ENDOCRINOLOGY-NEUROENDOCRINOLOGY- GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR ET DRA HENRIQUETA VERLANGIERI CAIO. The GH-growth hormone plays a central role in the regulation of body growth and development growth beyond the longitudinal, linear in juvenile, infant, child and adolescent, which is modulated by sex steroids. A presence with interaction between estrogen and GH leads to obtaining gender specific body composition during puberty. Most previous studies have focused on the effects of estrogen on GH secretion. There is also strong evidence that estrogen modulates GH action independent of secretion. The metabolic action of GH in the liver, causing a decrease in the production of IGF-I and fat oxidation in general is present. This results in a loss of lean tissue and a gain of body fat in postmenopausal women and there is an analogy in a GHD effect in
- 5. women with hypopituitarism replacing GH. The hypopituitarism is an endocrine disorder characterized by decreased secretion of one or more of the eight hormone normally produced by the pituitary (hypophyses), in the base of the brain. If there is a reduction of most pituitary hormones, the term is used panhypopituitarism. Signs and symptoms vary according to the affected hormones and the primary cause of the abnormality. The diagnosis is made by blood tests, but specific tests are usually needed and other surveys for which the root causes are identified and the treatment to be adopted. The negative metabolic sequelae are potentially important because of the widespread use of oral estrogen and estrogen-related compounds. The estrogen action affects the level of expression of GH receptor and signaling. More recently, estrogen has been shown to inhibit Janus kinase transducer/signal and activator of transcription by the GH signaling through induction of suppressor of cytokine signaling-2, an inhibitor of cytokine signaling protein. This represents a new paradigm of steroid regulation of cytokine receptors and is likely to have significance for a diverse range of cytokine function. Because Janus; Janus kinase (JAK) is a family of non-receptor intracellular tyrosine kinases, which translate mediated signals pathway the JAK-STAT cytokines. They were originally called "just another kinase" 1 and 2 (since they were only two of a large number of research findings in a PCR-based kinase), but were eventually published as "Janus kinase". The name is taken from the Roman god with two faces with beginnings and endings, Janus, because the JAKs have two domains transfer almost identical phosphate. A domain exhibits kinase activity, while the other negatively regulates the kinase activity of the former. In biochemistry, a kinase is a type of enzyme which transfers phosphate groups from high energy donor molecules (such as ATP) to specific target molecules (substrates). The process is called phosphorylation. The target molecule can activate or inactivate-by phosphorylation. All kinases require a divalent metal ion such as Mg2 + or Mn2 + to transfer the phosphate
- 6. group. These enzymes are activated by cyclic AMP, which catalyzes the phosphorylation of certain proteins. In addition to these logistical positions which is marked between the secretion of estrogen and GH is the estrogen route, however, exerts marked influence on the axis of growth hormone/insulin-like growth factor I (GH/IGF-I), however there is a need for detailed evaluation that does not compromise body mass especially in children, infant and child. Estrogens and action of growth hormone-GH: estrogenic effects on GH/IGF-I axis; GH regulates the growth and body composition by means of a complex process that combines mitogenic and metabolic actions that use mechanisms dependent and independent of IGF-I. The liver plays an important role in this metabolic process; it is a target organ in GH action, responsible for serum IGF-I and target organ of sex hormones as well. Estrogens are responsible for secondary sexual development and play a key role in female reproductive function. There is close relationship between estrogen and GH in the regulation of growth and development at puberty, this is one reason why eventually suggests be given for purposes of longitudinal or linear growth in child, infant and even teenagers or youth, the aid of inhibitors aromatase if you have indicated. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611
- 7. Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna CRM 28930 Como saber mais: 1. Proteínas de ligação de GH (GHBPs) GHBP-Growth Hormone-Binding Protein (Proteína ligadora do hormônio de crescimento) estão presentes no sangue de várias espécies e por complexação com circulação de GH hormônio de crescimento pode alterar a sua recarga e distribuição... http://hormoniocrescimentoadultos.blogspot.com 2. As ações de GHBP-Growth Hormone-Binding Protein humana (hGHBP) até agora têm sido estudados indiretamente, através de seus efeitos sobre a liberação de hGH... http://longevidadefutura.blogspot.com 3. As reações de complexação que são aquelas em que se formam complexos e fazem parte da complexometria... http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Rose SR, Ross JL, Uriarte M, Barnes KV, Cassorla FG, Cuttler Jr GB. The advantage of measuring stimulated as compared with spontaneous growth hormone levels in the diagnosis of growth hormone deficiency. N Engl J Med. 1988; 319:201- 207; Donaldson DL, Pan F, Hollowell JG, Stevenson JL, Gifford AR, Moore WV. Reliability of stimulated and spontaneous growth hormone (GH) levels for identifying the child with low GH secretion. J Clin Endocrinol Metab. 1991; 72:647- 652; Rosenfeld RG, Albertsson-Wikland K, Cassorla F, Fraiser SD, Haseqaua Y, Hintz RL, LaFranchi S, Lippe B, Lauriaux L, Melmed S. Diagnostic controversy: the diagnosis of childhood growth hormone deficiency revisited. J Clin Endocrinol Metab. 1995; 801:1532- 1540; Ghigo E, Bellone J, Aimaretti G, Bellone S, Loche S, Cappa M, Bartolotta E, Dammacco F,Camanni F. Reliability of provocative tests to assess growth hormone secretory status. Study in 472 normally growing children. J Clin Endocrinol Metab. 1996; 81 :3323- 327; Saggese G, Ranke MB, Saenger P, Rosenfeld RG, Tanaka T, Chaussain JL, Savage MO. Diagnosis and treatment of growth hormone deficiency in children and adolescents: towards a consensus. Horm Res. 1998; 50:320-340; Shalet SM, Toogood A, Rahim A, Brennan BMD. The diagnosis of growth hormone deficiency in children and
- 8. adults. Endocr Rev. 1998; 19:203-223; GH Research Society: Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: summary statement of the GH research society. J Clin Endocrinol Metab. 2000; 85:3990-3993. Rosenfeld RG. Editorial: is growth hormone deficiency a viable diagnosis? J Clin Endocrinol Metab. 1997; 82:349 -355; Juul A, Bernasconi S, Clayton PE, Kiess W, DeMuinck-Keizer Schrama S; Drugs and Therapeutics Committee of the European Society for Paediatric Endocrinology (ESPE). European audit of current practice in diagnosis and treatment of childhood growth hormone deficiency. Horm Res. 2002; 58:233-241; Wyatt DT, Mark D, Slyper A. Survey of growth hormone treatment practices by 251 pediatric endocrinologist. J Clin Endocrinol Metab. 1995; 80:3292-3297. Gourmelen M, Pham-Trung M, Girard F. Transient partial hGH deficiency in prepubertal children with delay of growth. Pediatr Res. 1979;13:221-224; Clayton PE, Price DA, Shalet SM. Growth hormone state after completion of treatment with growth hormone. Arch Dis Child. 1987; 62:222- 226. Contato: Fones: 55 11 5087-4404 ou 96197-0305 Nextel: ID:111*101625 Rua Estela, 515 - Bloco D - 12º andar - Conj. 121/122 Paraiso - São Paulo - SP - Cep 04011-002 e-mails: drcaio@vanderhaagenbrasil.com drahenriqueta@vanderhaagenbrasil.com vanderhaagen@vanderhaagenbrasil.com Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr Video http://youtu.be/woonaiFJQwY Google Maps: http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl= pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie =UTF8&ll=-23.575591,- 46.650481&spn=0,0&t = h&z=17