Três Fatores Chave para o Sucesso do Tratamento da Baixa Estatura
•
1 gostou•231 visualizações

Nessa época, entretanto, as possibilidades de tratamento ficam muito reduzidas, pois as epífises ósseas já se encontram em processo de fechamento muito adiantado devido à ação dos hormônios da puberdade (exceto aqueles casos em que existe um atraso significativo da idade óssea). Na baixa estatura constitucional, o ideal é que o paciente inicie o tratamento pelo menos dois a três anos antes do estirão puberal. Com tratamento endocrinológico, os filhos poderão chegar à altura que desejamos?

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Três Fatores Chave para o Sucesso do Tratamento da Baixa Estatura
Semelhante a Três Fatores Chave para o Sucesso do Tratamento da Baixa Estatura (20)
Mais de Van Der Häägen Brazil
Mais de Van Der Häägen Brazil (20)
Três Fatores Chave para o Sucesso do Tratamento da Baixa Estatura
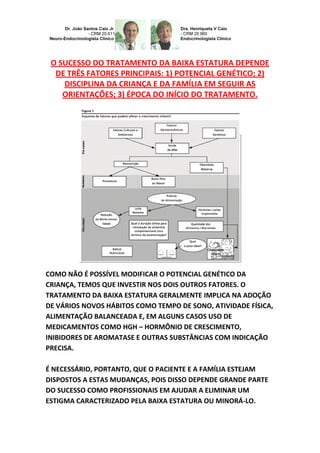
- 1. O SUCESSO DO TRATAMENTO DA BAIXA ESTATURA DEPENDE DE TRÊS FATORES PRINCIPAIS: 1) POTENCIAL GENÉTICO; 2) DISCIPLINA DA CRIANÇA E DA FAMÍLIA EM SEGUIR AS ORIENTAÇÕES; 3) ÉPOCA DO INÍCIO DO TRATAMENTO. COMO NÃO É POSSÍVEL MODIFICAR O POTENCIAL GENÉTICO DA CRIANÇA, TEMOS QUE INVESTIR NOS DOIS OUTROS FATORES. O TRATAMENTO DA BAIXA ESTATURA GERALMENTE IMPLICA NA ADOÇÃO DE VÁRIOS NOVOS HÁBITOS COMO TEMPO DE SONO, ATIVIDADE FÍSICA, ALIMENTAÇÃO BALANCEADA E, EM ALGUNS CASOS USO DE MEDICAMENTOS COMO HGH – HORMÔNIO DE CRESCIMENTO, INIBIDORES DE AROMATASE E OUTRAS SUBSTÂNCIAS COM INDICAÇÃO PRECISA. É NECESSÁRIO, PORTANTO, QUE O PACIENTE E A FAMÍLIA ESTEJAM DISPOSTOS A ESTAS MUDANÇAS, POIS DISSO DEPENDE GRANDE PARTE DO SUCESSO COMO PROFISSIONAIS EM AJUDAR A ELIMINAR UM ESTIGMA CARACTERIZADO PELA BAIXA ESTATURA OU MINORÁ-LO.
- 2. FISIOLOGIA–ENDOCRINOLOGIA–NEUROENDOCRINOLOGIA–GENÉTICA– ENDÓCRINO-PEDIATRIA (SUBDIVISÃO DA ENDOCRINOLOGIA): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO. (ESTE ARTIGO É APRESENTADO EM PORTUGUÊS – INGLÊS – ESPANHOL). Outro aspecto fundamental é a época de iniciar o tratamento. Uma vez identificada a baixa estatura, quanto mais precoce iniciarmos o tratamento maiores serão as possibilidades de alcançarmos os resultados desejados. Embora alguns sinais da baixa estatura sejam percebidos na infância, são comuns os pais e o paciente só procurarem orientação especializada na puberdade, quando o adolescente começa a perder sua autoestima em função da demanda social da estatura. Nessa época, entretanto, as possibilidades de tratamento ficam muito reduzidas, pois as epífises ósseas já se encontram em processo de fechamento muito adiantado devido à ação dos hormônios da puberdade (exceto aqueles casos em que existe um atraso significativo da idade óssea). Na baixa estatura constitucional, o ideal é que o paciente inicie o tratamento pelo menos dois a três anos antes do estirão puberal. Com tratamento endocrinológico, os filhos poderão chegar à altura que desejamos? Embora vários avanços já tenham sido alcançados no tratamento da baixa estatura, infelizmente as pessoas não podem escolher sua altura final que eventualmente desejam, tendo em vista que grande parte dela ainda depende do potencial genético herdado não apenas dos pais, mas também das gerações anteriores.
- 3. Os tratamentos modernos permitem estimular a produção do próprio hormônio de crescimento - GH, melhorar os fatores nutricionais, corrigir eventuais deficiências hormonais, bloquear hormônios que estejam acelerando o fechamento das epífises ósseas e até neutralizar uma parte da expressão genética de algumas síndromes relacionadas à baixa estatura (ex: síndrome de Turner). Se o paciente tiver predisposição para alta estatura, mas não a estiver alcançando por alguma situação clínica ou deficiência hormonal, o tratamento endocrinológico lhe permitirá aproveitar todo o seu potencial. O papel do endocrinologista e neuroendocrinologi sta é criar condições para que o paciente alcance o máximo de desenvolvimento estatural para o qual está programado geneticamente. Um aspecto de extrema importância é a precocidade de atitude preventiva que devemos tomar, pois quanto mais cedo for tomada a atitude corretiva ou estimulativa, melhor será o resultado final com o objetivo de aperfeiçoar a expectativa desejada por pais e filhos em relação à estatura razoável que será alcançada e não esquecendo que quanto tempo mais é postergado a estimulação adequada, menor o resultado alcançado com relação ao crescimento longitudinal. Não é segredo que o tratamento de crescimento estatural é uma situação que requer uma qualificação profissional ímpar de quem se propuser a corrigir ou estimular uma situação estigmatizante, pois a cada dia que passa as pesquisas evoluem, e a bem da verdade, os
- 4. conhecimentos científicos tem evoluído de forma logarítmica. WHEN CHILDREN AND YOUTH MAY HAVE CHILDREN FACTORS THAT INFLUENCE IN THE TREATMENT IN ORDER TO OPTIMIZE THE HEIGHT GROWTH? THE LOW TREATMENT SUCCESS DEPENDS ON HEIGHT THREE KEY FACTORS: 1) GENETIC POTENTIAL; 2) DISCIPLINE OF CHILDREN AND FAMILY TO FOLLOW THE INSTRUCTIONS; 3) TIME OF THE START OF TREATMENT. HOW CAN NOT MODIFY THE POTENTIAL GENETIC CHILD, WE INVEST IN TWO OTHER FACTORS.
- 5. THE LOW TREATMENT HEIGHT SHOULD GENERALLY IN VARIOUS ADOPTION OF NEW HABITS LIKE SLEEPING TIME, PHYSICAL ACTIVITY, BALANCED FEED AND, DRUG USE IN SOME CASES AS HGH - GROWTH HORMONE, AROMATASE INHIBITORS AND OTHER SUBSTANCES WITH ABSOLUTE NEED STATEMENT. YOU MUST THEREFORE THE PATIENT AND FAMILY ARE WILLING TO THESE CHANGES BECAUSE OF THIS GREAT SUCCESS DEPENDS ON THE PART AS IN PROFESSIONAL HELP ELIMINATE A STIGMA FEATURED BY LOW HEIGHT OR ALLEVIATING IT. PHYSIOLOGY-ENDOCRINOLOGY- NEUROENDOCRINOLOGY-GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO. (THIS ARTICLE IS WRITTEN IN PORTUGUESE - ENGLISH -). Another key aspect is the time to start treatment. Once identified short stature, the earlier we start the treatment greater will be the chances of achieving the desired results. Although some of the signs are perceived short stature in children, it is common for parents and the patient only seek expert guidance at puberty when teenagers start to lose your self-esteem due to the social demand of stature. At that time, however, the treatment options are very limited because the bone epiphysis already with closing process very early due to the action of the hormones of puberty (except those cases where there is a significant delay in bone age). At low constitutional stature, the ideal is that the patient begins treatment at
- 6. least two to three years before the growth spurt. With endocrine treatment, the children can reach the height we want? Although many advances have been made in the treatment of short stature, unfortunately people cannot choose their final height that eventually wished, given that much of it still depends on the genetic potential inherited not only the parents but also of previous generations. Modern treatments allow stimulate the production of growth hormone itself - GH, improve nutritional factors, correct any hormonal deficiencies, block hormones that are accelerating the closure of bone epiphysis and to neutralize a part of the gene expression of some syndromes related to short stature (e.g., Turner syndrome). If the patient has a predisposition to high stature, but not is reaching for some medical condition or hormonal deficiency, endocrine treatment will allow you to take advantage of its full potential. The role of the endocrinologist and neuroendocrinologist is to create conditions for the patient to reach the maximum height development for which is genetically programmed. A very important aspect is the early preventive attitude we should take, because the sooner it is taken corrective or estimulativa attitude, the better the end result in order to improve the desired expectation for parents and children in relation to the reasonable height to be achieved and not forgetting that much longer is postponed proper stimulation, less result will be achieved with respect to the longitudinal growth. It is no secret that the treatment of height growth is a situation that requires an odd professional qualification who proposes to correct or encourage a stigmatizing situation, because every day the research evolves and in actual fact the scientific knowledge has evolved so logarithmic. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna
- 7. CRM 28930 Como saber mais: 1. A constatação de baixa estatura por DGH – deficiência de hormônio de crescimento, durante a avaliação diagnóstica de crianças de baixa estatura, pode-se, através destes exames, diferenciar casos de crianças com DGH, das crianças de baixa estatura idiopática ISS... http://hormoniocrescimentoadultos.blogspot.com. 2. Seguindo o diagnóstico dos primeiros, devemos regular o monitoramento dos níveis séricos de IGF-1 (insulin-like growth factor–1), e IGFBP-3 (insulin-like growth factor binding protein–3), nas crianças que estão recebendo reposição hormonal do GH rDNA é importante pelas seguintes razões: em 1º porque esses parâmetros são estáveis em relação aos níveis de GH, e são extremamente sensíveis às suas variações, e os níveis destes parâmetros se manterão “normais” quando a reposição do GH rDNA bioidêntico for fisiologicamente efetivo... http://longevidadefutura.blogspot.com 3. Em 2º para razões teóricas de segurança, a manutenção dos níveis de IGF-1 (insulin-like growth factor–1), e IGFBP-3 (insulin-like growth factor binding protein-3) dentro de pelo menos 2 DS (desvios padrões) em relação aos valores relativos à idade e sexo do paciente, são essencialmente dados quando altos níveis de IGF-1 (insulin-like growth factor–1), e baixos níveis de IGFBP-3 (insulin-like growth factor binding protein-3) tem sido associados ao aumento de casos de neoplasia... http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Tzeel A, Fine MJ. Plan and pharmacy perspectives: growth hormone therapy, formulary, and benefit authorization. Manag Care. 2009;18(8)(suppl 6):17-19. ; Reiser PA. Pediatric growth hormone deficiency. Human Growth
- 8. Foundation; Dunn JD, Nickman NA. Indications for recombinant human growth hormone and evaluation of available recombinant human growth hormone devices: implications for managed care organizations. Am J Manag Care. 2011;17(suppl 18):eS16-eS22. ; Wilson TA, Rose SR, Cohen P, et al; Lawson Wilkins Pediatric Endocrinology Society Drug and Therapeutics Committee. Update of guidelines for the use of growth hormone in children: the Lawson Wilkins Pediatric Endocrinology Society Drug and Therapeutics Committee. J Pediatr. 2003;143(4):415-421. ; Guidelines for the use of growth hormone in children with short stature. A report by the Drug and Therapeutics Committee of the Lawson Wilkins Pediatric Endocrine Society. J Pediatr. 1995;127(6):857-867. ; Richmond E, Rogol AD. Current indications for growth hormone therapy for children and adolescents. In: Hindmarsh PC, ed. Current Indications for Growth Hormone Therapy. Vol 18. 2nd rev ed. Basel, Switzerland: S. Karger AG; 2010:92-108. ; Cook DM, Yuen KC, Biller BM, Kemp SF, Vance ML; American Association of Clinical Endocrinologists. American Association of Clinical Endocrinologists medical guidelines for clinical practice for growth hormone use in growth hormonedeficient adults and transition patients—2009 update. Endocr Pract. 2009;15(suppl 2):1-29. ; Romano AA, Allanson JE, Dahlgren J, et al. Noonan syndrome: clinical features, diagnosis, and management guidelines. Pediatrics. 2010;126(4):746-759. ; Bondy CA. Care of girls and women with Turner syndrome: a guideline of the Turner Syndrome Study Group. J Clin Endocrinol Metab. 2007;92(1):10-25. ; Saenger P, Wikland KA, Conway GS, et al; Fifth International Symposium on Turner Syndrome. Recommendations for the diagnosis and management of Turner syndrome. J Clin Endocrinol Metab. 2001;86(7):3061-3069. ; Clayton PE, Cianfarani S, Czernichow P, Johannsson G, Rapaport R, Rogol A. Management of the child born small for gestational age through to adulthood: a consensus statement of the International Societies of Pediatric Endocrinology and the Growth Hormone Research Society. J Clin Endocrinol Metab. 2007;92(3):804-810. ; Cohen P, Rogol AD, Deal CL, et al; 2007 ISS Consensus Workshop participants. Consensus statement on the diagnosis and treatment of children with idiopathic short stature: a summary of the Growth Hormone Research Society, the Lawson Wilkins Pediatric Endocrine Society, and the European Society for Paediatric Endocrinology Workshop. J Clin Endocrinol Metab. 2008;93(11):4210-4217. ; Goldstone AP, Holland AJ, Hauffa BP, Hokken-Koelega AC, Tauber M; speakers contributors at the Second Expert Meeting of the Comprehensive Care of Patients with PWS. Recommendations for the diagnosis and management of Prader-Willi syndrome [published correction appears in J Clin Endocrinol Metab. 2010;95(12):5465]. J Clin Endocrinol Metab. 2008;93(11):4183-4197. Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr google.com/+JoãoSantosCaioJrvdh google.com/+VANDERHAAGENBRAZILvdh Video http://youtu.be/woonaiFJQwY VAN DER HAAGEN BRAZI