Baixado 23 vezes

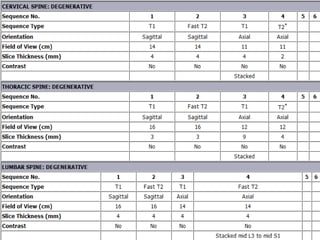
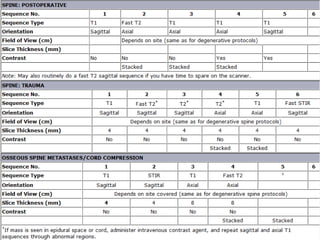
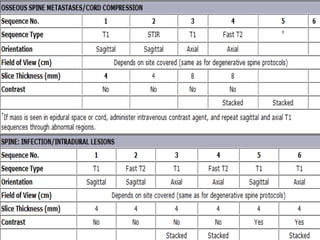
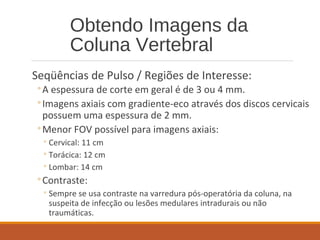
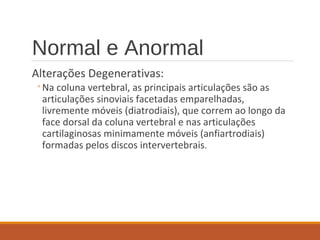
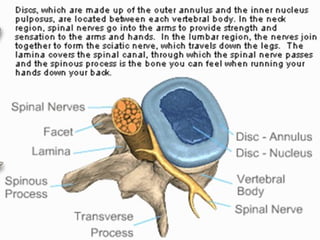
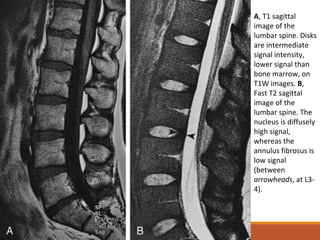
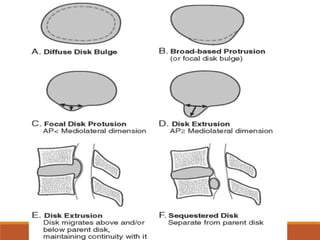
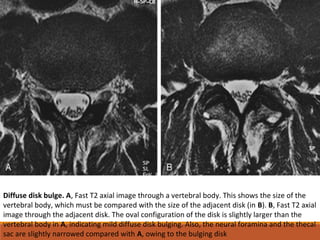
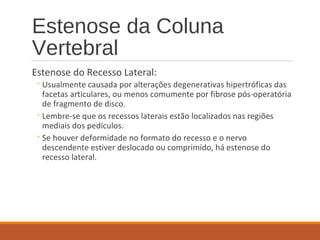


Este documento fornece informações sobre a avaliação por ressonância magnética da coluna vertebral. Ele descreve os protocolos de imagem, alterações degenerativas normais e anormais dos discos intervertebrais e das articulações facetárias, e anormalidades morfológicas dos discos como abaulamentos, protrusões e extrusões. Também discute hematomas epidurais e mielopatia compressiva relacionada aos discos.






















































![metodologias-ativas-de-aprendizagem.pptx_(1)[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/metodologias-ativas-de-aprendizagem-260204140054-ff555186-thumbnail.jpg?width=640&height=640&fit=bounds)




