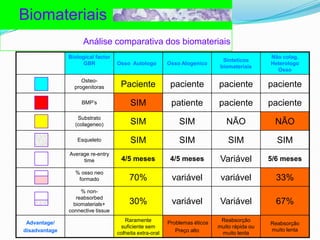
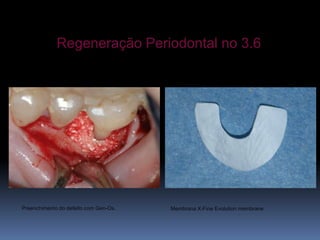
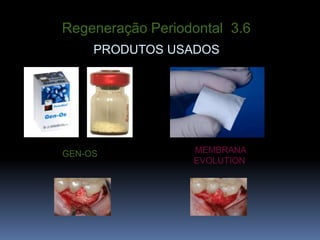
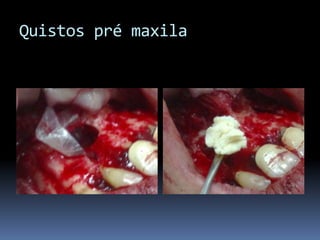
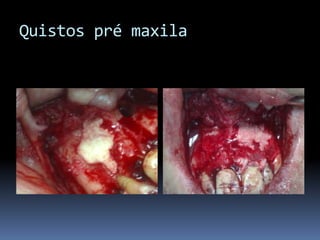
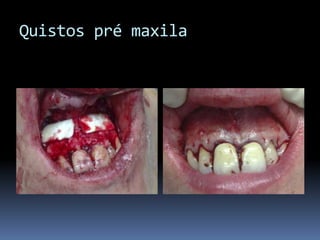
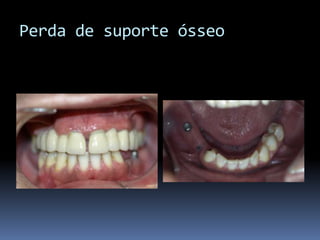
O documento discute a regeneração óssea guiada e seus biomateriais. Colágeno é descrito como o substrato ideal para regeneração óssea, pois promove a afinidade das proteínas morfogenéticas ósseas, protege essas proteínas, previne sua difusão prematura e é completamente reabsorvido, substituído por novo osso formado. Vários casos clínicos ilustram o uso de colágeno e membranas reabsorvíveis para regeneração óssea e periodontal.