

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (11)
Semelhante a Granulomatosis de wegener
Semelhante a Granulomatosis de wegener (20)
Mais de MINSA
Último
Último (20)
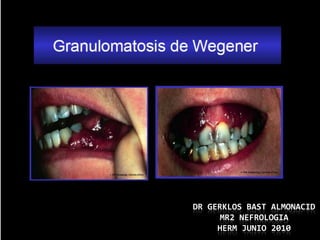
Granulomatosis de wegener
- 1. DR GERKLOS BAST ALMONACID MR2 NEFROLOGIA HERM JUNIO 2010
- 2. 1.- Inflamacion granulomatosa de tracto respiratorio 2.- glomerulonefritis progresiva 3.- vasculitis necrotizante de arterias y venas de mediano y pequeño calibre
- 3. ORGANOS COMPROMETIDOS 95% Pulmón (vasos ) 35% oído medio 90% senos 30% corazón 85% riñón 20% nervios 75% nasofaringe, periféricos bazo 20% SNC 70% articulaciones 50% piel 50% ojos
- 4. INCIDENCIA – PREVALENCIA Bastante rara > Hombres Edad 50-60 años > 95% Caucasicos Arthritis Rheum 2000 Feb;43(2):414 J Watch 2000 Mar 15;20(6):49)
- 5. CAUSAS Desconocida Probablemente inmunologica
- 6. PATOGENESIS Inmunidad tipo III hipersensibilidad mediada por inmunmocomplejos Vasculitis necrotizante de arterias y venas de mediano y pequeño calibre Matriz de metaloproteinasas (MMPs) y sus inhibidores endogenos han sido sugeridos en rol patologico Infeccion con Staphylococcus pueden provocar recaidas
- 7. CUADRO CLINICO Presentaciones comunes Sinusitis , descarga nasal crónica Pérdida de audición Dolor articular hemoptisis Hematuria microscópica Fiebre ( 90 %) Ocasionalmente Glomerulonefritis, tos, rinitis, otitis, disnea , dolor muscular , neuritis, pérdida de peso Tervaert, JW. Anti-neutrophil cytoplasmic antibodies: Current diagnostic and pathophysiological potential. Kidney Int 2004 ; 46:1
- 10. DIAGNOSTICO 1.-Nasal or oral inflammation (painful or painless oral ulcers or purulent or bloody nasal discharge) 2.-Abnormal chest radiograph showing nodules, fixed infiltrates, or cavities 3.-Abnormal urinary sediment (microscopic hematuria with or without red cell casts) 4.- Granulomatous inflammation on biopsy of an artery or perivascular area American College of Rheumatology Arthritis Rheum 2009 Aug;33(8):1101
- 11. PRUEBAS A CONSIDERAR Hematometría ,creatinina sérica Examen completo de orina Factor reumatoideo ANA hepatitis serología (ANCA) anti-neutrophil cytoplasmic antibody biopsia Piel (> rendim), anormalidades en uro análisis Biopsia de nervio sural Biopsia nasal (vasculitis and inflamación granulomatosa) Radiografía de tórax Angiografía Ecocardiografía Mayo Clin Proc 2005 Nov;80(11):1435
- 13. PRUEBAS SEROLOGICAS ANCA – C 90 % G W alta sensibilidad y especificidad (1,3) ANCA – p negativo (1, 5) ANCA –c 81% sensitivity, 98% specificity, 54% VPP and 99% VPN ; (2,3,4) ELISA para ANCA –PR3 (5) Ann Intern Med 1997 Jun 1;126(11):866 Journal Club on the Web 1997 Jun 10) Arthritis Rheum 1998 Sep;41(9):1521 Arch Intern Med 2002 Jul 8;162(13):1509 (Ann Rheum Dis 2009 Feb;68(2):228 (5)
- 15. ANATOMIA PATOLOGICA PULMON : vasculitis granulomatosa , necrotizante (fibrinoide) , granulomas no caseificantes RIÑÓN : GMN focal y segmentaria con progresión a medias lunas GMN necrotizante VASOS : infiltrado inflamatorio y fibrosis ARTERITIS GRANULOMATOSA : predominantemente infiltrado monocítico con cell gigantes y formación de granuloma Koderisch, J, et al. Wegener's granulomatosis with renal involvement: Patient survival and correlations between initial renal function, renal histology, therapy and renal outcome. Clin Nephrol 2007; 35:139.
- 16. EULAR CLASSIFICATION classification of ANCA-associated vasculitis 1.-Localized — Upper and/or lower respiratory tract disease without any other systemic involvement or constitutional symptoms. 2.-Early systemic — Any, without organ-threatening or life-threatening disease. 3.-Generalized — Renal or other organ-threatening disease, serum creatinine ≤ 5.6 mg/dL (500 micromol/L). 4.-Severe — Renal or other vital organ failure, serum creatinine ≥ 5.7 mg/dL (500 micromol/L) 5.-Refractory — Progressive disease unresponsive to glucocorticoids and cyclophosphamide. European League Against Rheumatism (EULAR) 2008 EULAR recommendation for the management of primary small vessel vasculitis. Ann Rheum Dis 2008
- 18. TRATAMIENTO INDUCCION - REMISION Típicamente altas dosis de esteroides y ciclophosphamide ( oral pulsos IV ) methotrexate (o azatioprina si cr > 2 mg/dL ciclofosfamida i IV IG 2 g/kg Mantenimiento de remisión methotrexate 20-25 mg/sem o azathioprine 2 mg/kg/d x 12- 18 m (menos toxica q ciclofl ) trimethoprim-sulfamethoxazole 160/800 mg 2v/d x 24 m reduce el promedio de recaída
- 19. SUMMARY AND RECOMMENDATIONS — The treatment of Wegener's granulomatosis usually begins with cyclophosphamide and glucocorticoid therapy to induce remission. Cyclophosphamide is discontinued one to two months after complete remission is achieved, which usually occurs 3 a 6 m. After cyclophosphamide has been discontinued: Maintenance therapy should not be started until the white BCC is >4000 c and the absolute neutrophil count is >1500 c . Tatsis, E, et al. Therapy for the maintenance of remission in sixty-five patients with generalized Wegener's granulomatosis. Arthritis Rheum 2003 ; 39:2052.
- 20. If these criteria are met, maintenance can be begun within days after cessation of oral cyclophosphamide and within two to four weeks after the last monthly dose of intravenous cyclophosphamide Initiation of maintenance therapy with methotrexate or azathioprine to sustain the remission (Grade 1A) Bacon, P. A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies. N Engl J Med 2003; 349:36.
- 21. azathioprine rather than methotrexate for initial maintenance therapy GFR < 50 mL/´ (Grade 2B). - Azathioprine : initial dose of 2 mg/kg x d The dose can be lowered to 1.5 mg/kg x d at one year from the time of initiation of induction therapy - methotrexate : initial dose 0.3 mg/kg 1 v/sem (max 15 mg) increased by 2.5 mg x sem - max dose of 25 mg 1 v /sem + folic acid (1 to 2 mg/day) or folinic acid (2.5 to 5 mg/week, 24 hours after methotrexate) Maintenance immunosuppressive therapy should be continued for 12 to 18 ms. Longer term or indefinite maintenance therapy may be warranted in patients with multiple relapses. glucocorticoid therapy (prednisone or equivalent), using the lowest dose required for control of extrarenal symptoms (Grade 1C). Bacon, P. A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies. N Engl J Med 2008; 349:36.
- 22. DIAGNOSTICO DIFERENCIAL hypersensitivity vasculitis, septic arthritis (fungal, tuberculosis), lymphomatoid granulomatosis other causes of granulomatous arteritis - Churg-Strauss vasculitis, temporal arteritis, Takayasu's arteritis, seronegative spondylarthropathy (aortitis) other vasculitis of small-to-medium arteries - polyarteritis nodosa, inflammatory rheumatic diseases, HBV, HCV, HIV infection embolic disease - endocarditis (septic, marantic), atrial myxoma, cholesterol embolization vessel stenosis or spasm - atherosclerosis, fibromuscular dysplasia, drug- induced vasospasm (ergotamines, cocaine, phenylpropanolamine), intravascular lymphoma vessel thrombosis - disseminated intravascular coagulation (DIC), thrombotic thrombocytopenic purpura (TTP), coumadin-associated necrosis, antiphospholipid antibody syndrome similar syndrome described in 5 adults with autosomal recessive defective surface expression of HLA class-I molecules. cocaine-induced pseudovasculitis described in case report Mayo Clin Proc 2005 May;80(5):671 Lancet 1999 Nov 6;354(9190):1598
- 24. COMPLICACIONES Glomerulonefritis (3) rápidamente progresiva Hemorragia alveolar (gnrp) pápulas, ulceras y Falla renal lesiones urticariales Sepsis uveítis, neuritis óptica Anemia normocítica (2) normocrómica cardiomiopatía dilatada CID y pericarditis Trombo embolismo enfermedad orbital venoso (1) inflamatoria (4) Compromiso meníngeo Ann Intern Med 2005 Apr 19;142(8):620 Rheumatology (Oxford) 2008 Apr;47(4):530 Mayo Clin Proc 2000 Aug;75(8):856 Eye 2006 Oct;20(10):1196
- 25. RESISTENCIA A LA CICLOFOSFAMIDA the first step is to ensure that the cyclophosphamide regimen has been optimized and, if indicated, plasma exchange has been administered. Mycophenolate mofetil or rituximab (Grade 2C). mycophenolate mofetil 500 mg 2v/d which is increased, if there is no response, by 250 mg 2v/d c/2 sem to a max dose 500 mg 2v/d rituximab : 375 mg/m2 weekly for 4 weeks.