Baixado 23 vezes


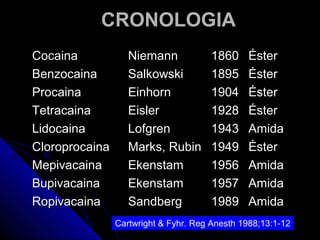
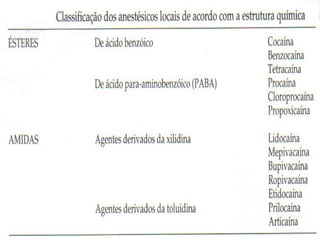



O documento fornece informações sobre a história da anestesia local, incluindo o isolamento da cocaina por Niemann em 1860 e sua investigação por Sigmund Freud e Carl Koller. Também discute o desenvolvimento de vários anestésicos locais ao longo do tempo, como a lidocaina e a bupivacaina.















































