Recomendados

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Sarathy Danyas PNS FINAL
Semelhante a Sarathy Danyas PNS FINAL (20)
Sarathy Danyas PNS FINAL
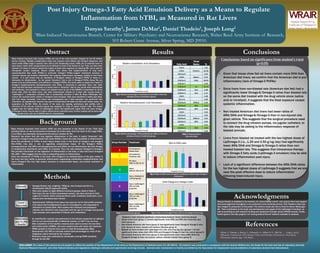
- 1. Post Injury Omega-3 Fatty Acid Emulsion Delivery as a Means to Regulate Inflammation from bTBI, as Measured in Rat Livers Danyas Sarathy1, James DeMar1, Daniel Thadeio1, Joseph Long1 1Blast-Induced Neurotrauma Branch, Center for Military Psychiatry and Neuroscience Research, Walter Reed Army Institute of Research, 503 Robert Grant Avenue, Silver Spring, MD 20910. DISCLAIMER: The views of the authors do not purport or reflect the position of the Department of the Army or the Department of Defense (para 4-3, AR 360-5). All research was conducted in compliance with the Animal Welfare Act, the Guide for the Care and Use of Laboratory Animals (National Research Council), and other federal statutes and regulations relating to animals and experiments involving animals. Animals were maintained in a facility accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International. Abstract Background Methods Results Conclusions Acknowledgments References 0 5 10 15 20 25 1 2 3 4 5 6 7 8 %ARA Treatment Group Relative Arachidonic Acid Abundance 0 0.5 1 1.5 2 2.5 3 3.5 4 1 2 3 4 5 6 7 8 %DHA Treatment Group Relative Docosahexaenoic Acid Abundance 0 2 4 6 8 10 12 1 2 3 4 5 6 7 8 ARA/DHA Treatment Group ARA to DHA ratio 0 2 4 6 8 10 12 14 16 18 20 1 2 3 4 5 6 7 8 Omega-6/Omega-3 Treatment Group Total Omega-6 to Omega-3 ratio Group Number Treatment No treatment, house chow No treatment, American diet No injury, NaCl at 120 uL/hr Injury, NaCl at 120 uL/hr Injury, Intralipid at 1.25 g/kg/day Injury, LipOmega-3 20% at 0.25 g/kg/day Injury, LipOmega-3 20% at 1.25 g/kg/day Injury, LipOmega-3 20% at 2.50 g/kg/day Fig. 1: Relative percentage of Arachidonic Acid (ARA) in Rat liver samples across all treatment groups Fig. 2: Relative percentage of Docosahexaenoic (DHA) in Rat liver samples across all treatment groups Fig. 3: Ratio of ARA (main Omega-6 contributor) to DHA (main Omega-3 contributor) Fig. 4: Ratio of all Omega-6 fatty acids to all Omega-3 fatty acids Student’s t-test indicates significant relationships between these treatment groups: • House chow livers (group 1) contain significantly more DHA and ARA than American diet livers (group 2) • Non-treated American diet livers (group 2) had significantly lower Omega-6/Omega-3 ratio than injured rat livers, treated with Sodium Chloride (group 4) • Blasted rat livers treated with LipOmega-3 at 1.25, and 2.5 g/kg/day (groups 7, 8) had significantly lower ratios (both ARA/DHA and Omega-6/Omega-3) than the control (group 5) • Non-treated American diet livers (group 2) had significantly lower ratios (ARA/DHA and Omega-6/Omega-3) than non-injured, sodium chloride treated livers (group 3) Fatty Acid Trivial Name % C14:0 1.51 C16:0 Palmitic 22.36 C16:1w-9 3.22 C18:0 Stearic 6.13 C18:1w-9 Oleic 28.24 C18:1w-7 4.35 C18:2w-6 LA 23.13 C18:3w-6 GLA 0.48 C18:3w-3 ALA 1.11 C20:0 0.48 20:1n-9 0.69 C20:3w-6 DHGLA 0.43 C20:4w-6 ARA 6.15 C20:5w-3 EPA 0.16 C22:0 0.19 C22:4w-6 0.24 C22:5w-6 DPAn-6 0.01 C22:5w-3 DPA 0.22 C24:0 0.11 C22:6w-3 DHA 0.59 C24:1w-9 0.09 Table 1: Representative fatty acid table Blast induced traumatic brain injuries (bTBIs) are one of the most prevalent dangers for the US military service member. Multiple complications—blast over pressure wave effects and shrapnel dispersion, and more—make bTBIs range in severity from mild to life threatening events. bTBIs are of potential harm to brain tissue, which when compromised can be difficult to treat in the theatre of war. Thus, our lab’s main interest is to study--in animal models--the impact of blast wave exposure on inducing TBI, and to look for therapeutic counter measures. Recent studies have shown that supplementation of long chain polyunsaturated fatty acids (PUFAs)—in particular, Omega-3 PUFAs—support membrane structure in neuronal tissues and produce metabolites that suppress inflammation processes, helping to heal these injuries. It is well known that an imbalance of Omega-6 relative to Omega-3 PUFAs in tissue is a biomarker for inflammation. As the typical “American” diet is rich in Omega-6 PUFAs (these FAs are shown to be pro-inflammatory) and deficient in Omega-3 PUFAs, this study seeks to assess the impact of Omega-3 supplementation—docosahexaenoic acid (DHA), in particular—in post-blast injury rats. Adult male rats that had been maintained on a house chow or “American” diet for one month were anesthetized with isoflurane, and exposed to a linear over pressure wave by use of the WRAIR’s compressed air driven shock tube. After the blast injury, rats were intravenously infused for 5 days with varying levels of “LipOmega-3,” a proprietary emulsion that is synthetically enriched in DHA (B. Braun Melsungen AG); control rats received saline vehicle or Intralipid mock emulsion. Rats were sacrificed 2 weeks post blast, with liver tissue harvested. Liver tissue was homogenized and a lipid extraction was performed with chloroform. An esterification reaction was used to functionalize the lipids into fatty acid methyl esters, for separation by GC/MS. While the results of the study are ongoing, preliminary lipid profiles with a minimum of five rats per treatment group was assessed by virtue of paired student t-test. The results suggest that the highest doses of LipOmega-3, which had significantly higher DHA and lower Omega- 6/Omega-3 ratios, may be able to reduce inflammation post-blast injury. Further analysis will be done with larger sample sizes, and use of ANOVA tests for interpretation Blast induced traumatic brain injuries (bTBI) are ever prevalent in the theatre of war. Their long- standing effects on service personnel encompass the entire body—from the brain to the lungs bTBIs , if not lethal, can potentially compromise the service member for life. Research has shown that diet may regulate inflammation in the body. A typical “American” diet, lacking in omega-3 polyunsaturated fatty acids (PUFAs), leaves the body susceptible to inflammation. Given the prevalence of PUFAs in brain tissue—these come in the forms of omega-3, and omega-6 FAs—PUFAs may play a role in regulating compromised tissue. Of the Omega-3 PUFAs, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are not inflammatory like their Omega- 6 complements—arachidonic acid (ARA), for example. Thus, the ratio between Omega-6 to Omega-3 FAs provides information on the regulation of inflammation in the body; a ratio that favors Omega-6 FAs (ARA > DHA) suggest that the body is responding poorly to inflammation. Given the prevalence of PUFAs in the body—with omega-3’s as building blocks of the gray matter in the brain and their ability to generate inflammation suppressing metabolites—supplementation that favors Omega-3 FAs may help restore structure to compromised tissue, and provide resolution to inflammation. Table 2: Rat treatment groups • Sprague-Dawley rats, weighing ~300g ea. were housed and fed in a standardized (AALAC approved) facility. • Rats were subject to eight different treatment groups, listed in Table 2. • Post injury (by use of blast overpressure waves), rats were returned to their cages for 2 weeks, before being sacrificed under anesthetic (isoflurane). Liver tissues were harvested post mortem. • Approximately 100mg of liver tissue was used per rat for lipid profile analysis. • Liver tissue was homogenized by use of a homogenizer, and suspended in chloroform to isolate lipids. After washes with methanol and potassium chloride, the chloroform was evaporated with the use of a nitrogen drying block • Lipid samples were suspended in Toluene until methylation • An esterification reaction was performed on the toluene suspension by adding a 14% wt/vol concentrated BF3 in Methanol solution, at 100o C for one hour • After completion of the reaction, hexanes were used to extract the now fatty acid methyl esters (FAMEs), and were washed twice with water and methanol. • FAME samples in hexanes were used in a Gas Chromatography/Mass Spectrometry (GC/MS) to calculate relative lipid percentages by virtue of the integration values returned by the machine. • Retention times were calibrated by individually running FAME standards through the GC/MS. Danyas Sarathy is indebted to his mentors, Dr. James DeMar and Dr. Joe Long for their kind support and encouragement throughout a very productive and enriching summer. Dan Thadeio’s data was also integral to production of this poster. The authors would also like to thank B. Braun Melsungen AG. Their contribution to the study was development and supply of the LipOmega-3 emulsion, as well as providing us with research funding and equipment through various CRADA awards. Finally, thanks goes to the CQL program, for making state-of-the-art research available to students. • Given that house chow fed rat livers contain more DHA than American diet livers, we confirm that the American diet is pro- inflammatory (lack of Omega-3 PUFAs) • Since livers from non-blasted rats (American diet fed) had a significantly lower Omega-6/Omega-3 ratios than blasted rats on the same diet treated with the drug vehicle alone (saline and/or intralipid), it suggests that the blast exposure causes systemic inflammation. • Non treated American diet livers had lower ratios of ARA/DHA and Omega-6/Omega-3 than in non-injured rats given vehicle. This suggests that the surgical procedure used to connect the drug infusion pumps, via jugular catheters, to the rats may be adding to the inflammatory response of blasted animals. • Livers from blasted rat treated with the two highest doses of LipOmega-3 (i.e., 1.25 and 2.50 g/kg/day) had significantly lower ARA/DHA and Omega-6/Omega-3 ratios than non- treated blasted rats. This suggests that intravenous therapy with Omega-3 fatty acids (LipOmega-3 emulsion) may be able to reduce inflammation post injury. • Lack of a significant difference between the ARA/DHA ratios for the two highest doses of LipOmega-3 suggests that we are near the peak effective dose to reduce inflammation following blast-induced injury. Conclusions based on significance from student’s t-test (p<0.05) Animals Lipid Extraction Methylation and GC/MS Profile Oliver, T., Demar, J., Riccio, C., Edwards, A., Albert, S. V., Hill, M., . . . Long, J. (n.d.). Efficacious Treatment for TBI: Omega-3 Fatty Acid Emulsion Delivered as a Post-Injury Intravenous Infusion (pp. 1-22, Rep.).