Biochemistry
•Transferir como DOCX, PDF•
2 gostaram•1,858 visualizações

Bachelor of Science in Nursing

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Biochemistry
Semelhante a Biochemistry (20)
Mais de RoxanneMae Birador
Mais de RoxanneMae Birador (20)
Último
Último (20)
Biochemistry
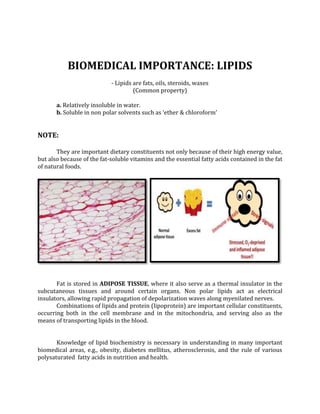
- 1. BIOMEDICAL IMPORTANCE: LIPIDS - Lipids are fats, oils, steroids, waxes (Common property) a. Relatively insoluble in water. b. Soluble in non polar solvents such as ‘ether & chloroform’ NOTE: They are important dietary constituents not only because of their high energy value, but also because of the fat-soluble vitamins and the essential fatty acids contained in the fat of natural foods. Fat is stored in ADIPOSE TISSUE, where it also serve as a thermal insulator in the subcutaneous tissues and around certain organs. Non polar lipids act as electrical insulators, allowing rapid propagation of depolarization waves along myenilated nerves. Combinations of lipids and protein (lipoprotein) are important cellular constituents, occurring both in the cell membrane and in the mitochondria, and serving also as the means of transporting lipids in the blood. Knowledge of lipid biochemistry is necessary in understanding in many important biomedical areas, e.g., obesity, diabetes mellitus, atherosclerosis, and the rule of various polysaturated fatty acids in nutrition and health.
- 2. LIPIDS ARE CLASSIFIED AS SIMPLE OR COMPLEX 1. SIMPLE LIPIDS: ester of fatty acids with various alcohols. a. Fats- ester of fatty acids with glycerol, oils are fats in the liquid state. b. Waxes- ester of fatty acids with higher molecular weight monohydric alcohols. 2. COMPLEX LIPIDS: ester of fatty acids containing groups in addition to an alcohol and a fatty acid. a. PHOSPHOLIPIDS- lipids containing, in addition to fatty acids and an alcohol, phosphoric acid residue. They frequently nitrogen-containing bases and other substituents, e.g., in ‘glycerophospholipids’ the alcohol is glycerol and in sphingophospholipids the alcohol is sphingosine. b. GLYCOLIPIDS (glycosphingolipids) – lipids containing a fatty acid, sphingosine and carbohydrate. c. Other complex lipids- lipids such as sulfolipids and amino lipids. Lipoproteins may also be placed in this category. 3. PRECURSOR AND DERIVED LIPIDS: These include fatty acids, glycerol, steroids, other alcohols, fatty aldehydes and ketone bodies, hydrocarbons, lipid-soluble vitamins and hormones. Vitamin A, D, E, K Neutral Fats: Are unchanged, acglycerols (glycerides), cholesterol, and cholesterly esters.
- 3. SATURATED FATTY ACIDS COMMON NAME NUMBER OF C ATOMS ACITIC 2 Major end product of CHO fermentation by rumen organisms BUTYRIC 4 In certain fats in small amount VALERIC 5 (especially butter) CAPROIC 6 An end product of CHO fermentation by rumen organisms. LAURIC 12 Spermaceti, cinnamon, palm kernel, coconut oils , laurels, butter MYRSITIC 14 Nutmeg, palm kernel, coconut oils, myrtles, butter PALMITIC 16 Common in all animals and plant fats STEARIC 18 Common in all animals and plant fats LIPIDS (CHO) Carbon and Hydrogen out # oxygen insoluble in water EXAMPLE: A. neutral fats (triglycerides) -found in fat deposits -made of fatty acids and glycerol - source of stored energy B. phospholipids - steroids EXAMPLE: Cholesterol bile salts vitamin D some hormones
- 5. LIPIDS Classification of Lipids 1. neutral fat 2. phospholipids 3. cholesterol 4. fatty acids NEUTRAL FAT (triglycerides)- are used in the body mainly to provide energy for the different metabolic process. It functions almost equally with CHO. PHOSPHOLIPIDS CHOLESTEROL- does not contain fatty acids. Its sterol nucleus is synthesized from degradation products of fatty acid molecules. FATTY ACID- example: Palmitic Acid CH3 (CH2)14 COOH BASIC CHEMICAL STRUCTURE OF TRIGLYCERIDES (Neutral Fat) CH3—(CH2)—COO—CH3 I CH3—(CH2)—COO—CH Tristearin I CH3—(CH2)—COO— CH3 Are used throughout the body to form the membranes of all cells of the body and to perform other cellular functions.
- 6. THREE FATTY ACIDS MOST COMMONLY PRESENT IN THE TRIGLYCERIDES 1. Streamic acid (as shown above), has 18 carbon chain and is fully saturated with hydrogen atoms. 2. Oleic acid- has 18 carbon chain but has one double bond in the middle of the chain. 3. Palmitic acid- has 16 carbon atoms and is fully saturated. Transfer of triglycerides and other lipids and by the lymph from Gastrointestinal Tract- the chylomicrons. FAT in the DIET absorb from intestine into the lymph digest in the intestine triglycerides monoglycerides fatty acids pass thru the intestinal epithelial cells they are resynthesized into new molecules (chylomicrons) enter the lymph chylomicrons absorbs protein B this increases their suspension stability in the fluid of lymph and prevents their adherence to the lymphatic vessel
- 7. PHOSPHOLIPIDS: Typical Phospholipids A Lecithin O II H 2C—O—C—(CH2)7—CH=CH—(CH2)7—CH3 I O I II HC—O—O—(CH2)16—CH3 CH3 I II I H2C—O—P—O—CH2—CH3— N – CH3 I I OH CH3 A Cephalin O II H 2C—O—C—(CH2)7—CH=CH—(CH2)7—CH3 I O I II HC—O—C—(CH2)16—CH3 I II H2C—O—P—O—CH2—CH2— N+H3 I OH Sphingomyelin CH3 I (CH2)12 I CH II CH I HO —C—H O I II HC—NH—C—(CH2)16—CH3 I O CH3 I II I H—CH—O—P—B—CH2—CH2—N—CH I I I H OH CH3
- 8. PROSTAGLADINS PGs— are synthesized aerobically from polyunsaturated fatty acids arachidonic acid with the help of multi enzyme complex called Prostaglandin H Synthase. FUNCTIONS OF PROSTAGLANDINS 1. CARDIO VASCULAR SYSTEM: PG-Es and PG-As are potent (active) vasodilators, they can prevent hypertension (decrease BP). 2. HAEMATOLOGICAL RESPONSE: - Capillary permeability is increased by: PGs-E1, E2, E 1∝, E 2 ∝, - Intradermal infection of PGs in man causes wheal and flare similar to histamine. - Platelets; PGE, is a potent inhibator of human platelet aggregation. Thus, PGE has proved useful for harvesting and storage of blood platelets for therapeutic transfusion. 3. ACTION ON GASTRO INTESTINAL SECRETIONS: a. GASTRIC SECRETION: PGsE1, E2, and A1-inhibit gastric secretion, whether basal or stimulated by feeding, histamine or pentagastrin.
- 9. b. Pancreatic Secretion: Its action is opposite. There is increase un volume, bicarbonate and enzyme content of pancreatic juice. c. Intestinal Secretion: Mucus secretion is increased. There is substantial movement of water and electrolytes into intestinal lumen. ⇨ PG-E, given orally in human volunteers produces watery diarrhea. 4. EFFECTS ON SMOOTH MUSCLES: a. Gastro Intestinal Musculature: - In human beings PG-E and F produce contraction of longitudinal muscle from stomach to colon. b. Bronchial Muscle: - PG-Fs contract and PG-Es relax bronchial and brachial Musculature. - PGE1 and PGE2, has been used for treatment of status asthmaticus. c. Uterine Muscle: - PGE1, E2, and PG-F2∝, when administered I.V. The response is prompt and close- dependent and takes the form of a sharp rise in tonus with super imposed rhythmic contractions. ⇨ PGE2 at 0.5 mg/ml has been used for induction of labor at or near term. If high doses 5mg/ml has been reported to be effective in therapeutic termination of pregnancy in 1st and 2nd trimesters (abortifacient). 5. METABOLIC EFFECTS AND ACTION OF ENDOCRINE ORGANS: - Lypolysis: PG-Es inhibit adenyl cyclase and lowers cyclic AMP level, thus decreasing lipolysis. - PGEs have also some insulin life effects on carbohydrates metabolism. -Excess PTH-like (Parathormone) effects on bone, resulting to mobilization of calcium from bone producing “hypercalcemia” - Exert thyrotropin like effect on thyroid gland. - Stimulation of steroid production by adrenal cortex (“Steroidogenesis”) - Luteolysis: Prompt subsidence of progesterone secretion and regression of corpus luteum follows parenteral injection of PGF2∝ in a wide variety of mammals. Mechanism of leutoclysis it involve block of the normal ovarian response to circulating Gonadotrophins.
- 10. MUSCLE AND THE CYTOSKELETON Biomedical Importance * CHON play an important role in movement at both organ (eg., skeletal muscle, heart and gut) and cellular levels. *Ca –calcium molecules used in muscular contraction. Molecular bases that affect muscle: *Duchenne-type muscular dystrophy due to mutations in the acne encoding dystrophin. *Malignant Hyperthermia a serious complication for some patients undergoing certain types of anesthesia. *Heart Failure a very common medical condition, with a variety of causes; its rational therapy requires understanding of the biochemistry of heart muscle.
- 11. CARDIOMYOPATHIES⇨ one group of conditions that cause heart failure. NITRIC OXIDE (N.O.)⇨major regulator of smooth muscle tone. NITROGLYCERIN⇨vasodilators, used in the treatment of angina pectoris. Act by increasing the formation of N.O. MYOFIBRILS of the SKELETAL MUSCLE contain thick and thin filament: -Thick filaments contain myosin -Thin filaments contain –actin –tropomyosin –troponin complex ⇨ tropenin T, tropenin I, tropenin C →Sliding filament cross-bridge model Is the foundation of current thinking about muscle contraction. BASIS: This model is the interdigitating filaments slide past one another during contraction and cross-bridges between myosin and actin generate and sustain the tension.
- 12. →The hydrolysis of ATP is used to drive movement of the filament. ATP binds to myosin heads and is hydrolyzed to ADP and Pi by theATP are activity of the acto myosin complex. →Ca plays a key role in the initiation of muscle contraction by binding to troponic C. In skeletal muscle, the sarcoplasmic reticulum regulates distribution of Ca to the sacromeres, where as inflow of Ca via Ca channels in the sarcolemma is of major importance in cardiac and smooth muscle. →Many care of malignant hyperthermia in humans are due to mutations in the gene encoding of the Ca release channel. →A number of differences exist between skeletal and cardiac muscle. Cardiac muscle contains a variety of receptors on its surface. →Some cause of familiar hypertrophic cardiomyopathy are due to messene mutation in the gene coding for 𝛽-myosin heavy chain. →Mutation in genes encoding a number of other proteins have also been detected. →Smooth muscle, unlike skeletal and cardiac muscle does not contain the troponic system, instead, phosphorylation of myosin light chains initiates contraction. →Nitric Oxide is a regulator of vascular smooth muscle and blockage of its formation from arginine causes an acute elevation of blood pressure, indicating that regulation of blood pressure is one of its many functions. →Duchenne-type muscle dystrophy, is due to mutations in the gene, located on the x chromosomes, encoding the protein dystrophin.
- 13. TWO MAJOR TYPES OF MUSCLE FIBERS ARE FOUND IN HUMAN: White : (anaerobic)- white are particularly used in sprints. Red : (aerobic)- the red in prolonged aerobic exercise. ⇨During the sprints, muscle uses creatine phosphate and glycolysis as energy sources. ⇨In the marathon, oxidation of fatty acids is of major importance during lutter phase. Non muscle cells perform various types of mechanical work carried out by the structures constituting the cytoskeleton. STRUCTURES INCLUDE — actin filament (microfilaments) —microtubules composed primarily of ∝ - tubulin and 𝛽 – tubulin —intermediate filament; include keratins, Vit. Like CHON, neurofilaments, lamins ⇨ 𝑺𝒆𝒒𝒖𝒆𝒏𝒄𝒆 𝒐𝒇 𝒆𝒗𝒆𝒏𝒕𝒔 𝒊𝒏 𝒄𝒐𝒏𝒕𝒓𝒂𝒄𝒕𝒊𝒐𝒏 𝒂𝒏𝒅 𝒓𝒆𝒍𝒂𝒙𝒂𝒕𝒊𝒐𝒏 𝒐𝒇 𝑺𝒌𝒆𝒍𝒆𝒕𝒂𝒍 𝑴𝒖𝒔𝒄𝒍𝒆 STEPS IN CONTRACTION: DR BIGGIR BF 1.Discharge of motor neuron. 2. Release of transmitter (acetylcholine) at motor end place. 3. Binding of acetylcholine to nicotinic acetylcholine receptors. 4. Increased Na and K conductance in end plate membrane. 5. Generation of action potential in muscle fibers. 6. Inward spread of depolarization along T tubules. 7. Release of Ca from terminal listerns of sarcoplasmic reticulum and diffusion to thick and thin filaments. 8. Binding of Ca to troponic C, uncovering myosin binding sites of actin. 9. Formation of cross-linkages between actin and myosin and sliding of thin on thick filaments, producing shortening. STEPS IN RELAXATION: CR C 1. Ca pumped back into sarcoplasmic reticulum. 2. Release of Ca from troponin. 3. Cessation of interaction between actin and myosin.
- 14. CAUSATION OF MALIGNANT HYPERTHERMIA Mutation in the RYR1 gene Altered Ca release channel protein (RYR1) (eg. Substitution of cys for Arg) Mutated channel opens more easily and stays open longer, thus flooding the cystosol with Ca. High intracellular level of Ca stimulates sustained muscle contraction (rigidity) and high Ca also stimulates breakdown of glycogen, glycolysis, and aerobic metabolism. (resulting in excessive production of heat) BIOCHEMICAL CAUSES OF INHERITED CARDIOMYOPATHIES CAUSE PROTEINS OR PROCESS AFFECTED Inborn errors of fatty acid oxidation Carnitine entry into cells and mitochondria. Certain enzymes of fatty acid oxidation. Disorder of Mitochondrial CHONS encoded by mitochondrial genes. Oxidative phosphorylation CHONS encoded by nuclear genes. Abnormalities of myocardial contractive 𝛽-myosin heavy chains , troponin and structural CHONS tropomyosin, dystropin
- 15. CAUSATION OF DUCHENNE MUSCULAR DYSTROPHY Deletion of part of the structural gene for dystrophin, located on the X chromosome. Diminished synthesis of the mRNA for dystrophin. Low levels or absence of dystrophin. Muscle contraction or relaxation affected; mechanism not elucidated. Progressive, usually fatal muscular weakness. CAUSATION OF FAMILIAR HYPERTROPHIC CARDIOMYOPATHY Preclaminantly messence mutation in the 𝛽-myosin heary chain gene on chromosome 14. Mutant polypeptide chain (poison polypeptides)that lead to formation of defective myofibrils. Compensatory hypertrophy of one or both cardiac ventricles. Cardiomegally and various cardiac S/Sx including sudden death.
- 16. PLASMA CHON (Protein) MAJOR TYPE: ⇨ albumin ∝ 𝜷𝟏 ⇨globulin 𝜷— ⇨fibrinogen 𝜷𝟐 ALBUMIN → for colloid osmotic pressure in plasma. It prevent plasma loss in the capillary. GLOBULIN→perform enzymatic function in the plasma, responsible for natural immunity. FRIBRINOGEN→forming blood clots to help to repair circulatory system. FUNCTION OF PLASMA CHON Transport: Transferin Ceruplasmin Lipoproteins Albumin Transcertin Retinol Haptoglobin Thyroxin
- 17. SPECIFIC FUNCTION OF SOME CHON: CHON PLASMA CONC. (g/L) FUNCTION Pre albumin 0.3 Binds T3 and T4 albumin 40.0 Transport colloid osmotic pressure ∝ 1- globulin 3.0 Anti proteinase ∝ 1- antitrypsin 3.0 Anti proteinase ∝ 2- globulin 3.0 Anti proteinase ceruplasmin 0.4 Copper transport heptoglobin 1.2 Binds hemoglobin ∝ 2- macroglobulin 3.0 Transport anti proteinase CHON PLASMA CONC. FUNCTION 𝛽-globulins transferin 2.5 Iron transport hemopexin 1.0 Binds haem plasminogen 0.7 Fibrinolysis fibrinogen 4.0 haemostasis globulin 0.9-4.5
- 18. MAJOR FUNCTION OF IMMUNOGLOBULIN (Ig) IMMUNOGLOBULIN 1. Ig G⇨ main antibody in the secondary response. Opsonizes bacteria, making than easier to phagocytes. Fixes complement, which enhances bacterial killing. Neutralizes bacterial toxins and viruses. Cross the placenta. 2. Ig A⇨ secretory Ig A prevents attachment of bacteria and viruses to mucous membrane. Does not fix complement. 3. Ig M⇨produced in the primary response to an antigen. Fixer complement. Does not cross the placenta . Antigen receptors on the surface of B cells. 4. Ig D⇨uncertain. Found on the surface of many B cells as well as in serum. 5. Ig E⇨mediates immediately hypersensitivity by causing release of mediators from most cella and basophile upon exposure to antigen (allergen). Defends against worm infection by causing release of enzymes from eosinophils. Does not fix complement. Main host defense against helmithic infection. PLASMA PROTEINS AND IMMUNOGLOBULINS Major functions in Blood: 1. RESPIRATION—transport of oxygen from the lungs to the tissue and of CO2 from the tissue to the lungs. 2. NUTRITION—transport of absorbed food materials. 3. EXCRETION— transport of metabolic waste to the kidneys,lungs, skin and intestines for removal. 4. Maintenance of the normal Acid-Base balance in the body. 5. Regulation of water balance through the effect of blood on the exchange of water between the circulating fluid and the tissue fluid. 6. Regulation of Body Temperature by the distribution of body heat.
- 19. 7. Defense against infection by the white blood cells and circulating antibodies. 8. Transport of hormones and regulation of metabolism. 9. Transport of Metabolites. 10. Coagulation → PLASMA: consists of water, electrolytes, metabolites, nutrients, protein and hormone. The water and electrolyte composition of plasma is practically the same as that of all extracellular fluids (Na,K, Ca, Cl, HCO3, PaCO2, and the blood pH: are important in the management of many patients. →ELECTROPHORESIS: the most common method of analyzing plasma proteins. →HYDROSTATIC PRESSURE: in anterioles is about 37mmHg with an interstitial (tissue) pressure of 1mmHg opposing it. →OSMOTIC PRESSURE (ONCOTIC PRESSURE): exerted by the plasma proteins in approximately 25mmHg. →STARLING FORCE: are the pressure of hydrostatic pressure and osmotic pressure. →EDEMA: If the concentration of plasma proteins is markedly diminished due to severe protein malnutrition, fluid is not attracted back into the intravascular compartment and accumulates in the extra vascular tissue space.
- 20. SOME FUNCTION OF PLASMA PROTEINS Function: Plasma Proteins Antiproteases antichymotrypsin,∝ 1 antitrypsin (∝ 1 antiproteinase) ∝ 2 macroglobin, antithrombin Blood Clotting various coagulation factors, fibrinogen Enzymes function in blood, eg, coagulation factors, cholinesterase Leakage from cells or tissue, eg. Amino transferase Hormones Erythropebetin Immune defense Immunoglobulins, complement proteins, 𝛽2 microglobulin Involvement in inflammatory response Acute phase response proteins, (eg. Creatine protein) ∝ 1 acid glycoprotein [orosomucoid] Oncofetal ∝ 1 fetoprotein (AFP) Transport of binding proteins - Albumin (various ligands, including bilinubin, fue fatty acids, ions (Cc), metals (Ca, Zn) methane, steroids other hormone and variety of drugs). -Ceruplasmin (contains Ca; albumin probably more important in pghniologis transport of Ca. -Corticosteriod-bing globulin (transcertin,binds cortesol) -Sex hormone-binding globulin (binds testosterone) -Thyroid-binding globulin (binds T3, T4) -Transthyretin -Retinol-binding protein
- 21. PROTEINS -are vital components of all living system. -they are present in the different parts of the body, like the muscle, skin, nails. -they catalyze reactions, transport oxygen, serve as hormones in the regulation of specific body processes and act as antibodies and blood clotting agent. -among the most important proteins in the body are: enzymes, hormones, and other component chromosomes and cell membranes. ⇨ Catalytic triad structure of many enzymes are: 1.base 2.nucleophile 3.oxyanion PROTEIN DIVERSITY IN HUMAN BODY Protein Function 1. actin, myosin, dystrophin muscle contraction 2. antibodies, antigens, cytokines immunity 3.carbohydrates,lipases, proteases digestive enzymes 4. casein milk protein 5.collagen, elastin connective tissue 6.colony stimulating factors blood cell formation 7.DNA polymerase DNA replication 8.Ferritin Iron transport 9.Fibrin, Thrombin blood clotting 10.Growth Factors cell division 11.Hemoglobin, myoglobin oxygen transport 12.Insulin, glucagon control of blood glucose level 13.Integrins, laminins cell adhesion 14.Keratin hair structure 15.Tubulin cell movements 16.Tumor Suppressors prevent cancer NOTE: short polymers of amino acids called PEPTIDES. This perform prominent roles in the neuro endocrine system as hormones, hormone releasing factor, neuro modulators, or neurotransmitters.
- 22. THYROID HORMONE -major metabolic hormone -has 2 active iodine—containing hormone such as Thyroxine (T4) and Triiodothyronine (T3) T4 : major hormone that will be converted to T3. T3 and T4 each is constructed from 2 Tyrosine. * T4 4 bonds of iodine * T3 3 bonds of iodine → In addition to amino acids found in the protein, some amino acids are known not to occur in proteins. Examples of non protein also known as are: 1. 𝜷- alanine— building block of the Vitamin A, pantothenic acid. 2. Ornithine— an intermediate of the urea cycle. 3. Gamma Aminobutyric Acid (GABA)— a chemical agent for the transmission of nerve impulses.
- 23. GROUPS OF FUNCTION PROTEINS Functional Group Roles in the Body 1. ANTIBODIES It recognize, bind with and inactive bacteria, toxins and some viruses, function in the immune response, with help protect the body from “invading” foreign substance. 2. HORMONES help to regulate growth and development. Example: Growth Hormone—an anabolic necessary for optimal growth. Insulin— helps to regulate blood sugar levels. Nerve Growth Factor—guides the growth of neurons in the development of nervous system. 3. TRANSPORT PROTEIN Hgb transport oxygen in the blood other transport proteins in the blood carry iron, cholesterol etc. 4. CATALYSTS Essential to every biochemical reactions in the body.Increase the rate of chemical reactions by at least a million fold. In their absence (or destruction) biochemical reactions cease. Substance form by a living cells that acts as a catalyst in bodily chemical reaction.
- 24. FUNCTIONAL ENZYME The substrates or molecule the enzymes acts on, has a corresponding binding site and 2 sites fit together very precisely. Substrate molecules fit the active site of enzyme in a lock—and—key analogy. If it is bind together there will be a reaction to form a new product. The substrate molecule must have a susceptible chemical bond that can be attacked. DENATURE ENZYME Enzyme—substrate binding can no longer occur. It involves the breaking of many weak linkages or bonds within a protein molecule that are responsible for the highly ordered structure of the protein in its natural state. It can be brought about in various ways by treatment with alkali, acid or urea.
- 25. PRINCIPAL SERUM ENZYMES USED IN CLINICAL Dx’c Serum Enzyme Major Dx’c Use Aminotransferases →Aspartate Aminotransferase Myocardial Infarction (AST or SGOT) →Alanine Aminotransferase Viral Hepatitis (ALT or SGPT) → Amylase Acute Pancreatitis →Ceruloplasmin Hepatolenticular degeneration (Willson’s Disease) →Creatine kinase Muscle disorders and Myocardial Infarction → Glutanyl transpeptidase various liver disease →Lactate dehydrogenase (Isozymes) Myocardial Infarction →Lipase Acute Pancreatitis →Phosphatase Alkaline (Isozymes) various bone disorders Obstructive liver disease →Morphine SO4 decrease pain and anxiety →Phosphatase Acid metastatic carcinoma of the prostate
- 26. THROMBIN—is the specific for catalyzing hydrolysis of a peptide bond adjacent to argine. Does so primarily in a protein essential to blood clothing with bond broken, the product. (Fibrin) proceeds to polymerize into blood clot. ENZYME PAPAIN— from papaya fruit. Catalyzes the hydrolysis of peptide bonds in many locations. Has ability to break down proteins accounts for the use in: a. meat tenderizers b. contact-lens cleaners c. cleansing dead or infected tissue from wounds (debridement) ENZYMES REACTION CATALYZED PAPAIN Hydrolysis of peptide bonds. RIBONULEASE Hydrolysis of phosphate ester link in RNA RINASES Transfer of phosphoryl group between substrates. CARBONIC ANHYDRASE converts CO2 to HCO3 MANAGEMENT FOR MYOCARDIAL INFARCTION M—morphine sulfate O—oxygen N—nitroglycerin A—aspirin to prevent aggregation of platelets HYDROGEN ION- determines the acid and basis of the blood. pH power of Hydrogen
- 27. CHO: SEQUENCE AND SITE OF CHEMICAL DIGESTION FOOD SOURCES OF ENZYME Lactose Starch Sucrose salivary amylase Oligosaccharide pancreatic amylase microvilli; brush border Lactose maltose Sucrose ENZYMES: (Dextrinase & Glucomylase) INTESTINALBRUSHBORDER: Lactase, Maltase and Sucrase Galactose Glucose Fructose NOTE: Absorption Monosaccharides (glucose, galactose and fructose) enter the capillaries of the villi and are transported to the liver via Hepatic Portal Vein.
- 28. CHON: SEQUENCE AND SITE OF CHEMICAL DIGESTION FOOD SOURCE OF ENZYMES SITE OF ACTION Proteins Pepsin (gastric glands) stomach Increase the presence of HCL Largest polypeptide Large polypeptide small intestine Pancreatic enzymes: (trypsin, chymotrypsin, carboxypeptidase) Small peptidase Amino Acids Intestinal (brush border) small intestine Enzymes: (aminopeptidase, carboxypeptidase, Dipeptidase) NOTE: Absorption Amino acids enter the capillaries of the villi and are transported to the liver via the Hepatic Portal Vein.
- 29. LIPIDS: SEQUENCE AND SITE OF CHEMICAL DIGESTION FOOD STUFF SOURCE ENZYMES SITE OF ACTION Unemulsified Emulsified by detergent action small of bile salts from the liver intestine pancreatic lipase monoglycerides glycerol & fatty acids & fatty acids NOTE: Absorption Absorbed primarily into the lacteal of the villi and transported in the lymph to the systemic circulation via the thoracic duet and then to the liver via hepatic artery. Glycerol and short-chain fatty acids are absorbed into the capillary blood in the villi and are transported to the liver via the Hepatic Portal Vein.
- 30. CHARACTERISTICS OF CEREBROSPINAL FLUID PARAMETER Normal value Abnormal Findings Volume 135-150 ml Volume increase with hydrocephalus, decrease in space occupying lesions. Specific gravity 1.007 Increase with blood cells and infection Color Crystal clear Discoloration (xanthochromia) looks red in intracranial and traumatic hemorrhage. Turbidity indicates an increase number of WBC Protein 15-45 mg/100ml Increase with tumors,injections and hemorrhage WBC 0-5cells/mm3 10-200 cells mostly lymphocytes occurs in viral meningitis , multiple sclerosis, tumor and neurosyphilis. Glucose 40-80 mg/ 100 ml Decrease in glucose indicates presence of glycolytic substances such as bacteria in CSF. Pressure 76-200mm H2 O Increase in Intracranial pressures
- 31. FLUIDS AND ELECTROLYTES SERUM VALUE: Na= 135-145mEq/L Cl= 95-105 mEq/L K= 3.5-5.0 mEq/L Mg= 1.5-2.5mEq/L PO4= 2.8-4.4 mEq/L Ca=9-11 mg/dL or 4.5-5.5 mEq/L HOMEOSTATIC MECHANISM →ANTIDIURETIC HORMONE (ADH) results in water retention. →ADRENOCORTICOTROPIC HORMONE (ACTH) stimulates the adrenal cortex to release cortisol and aldosterone causing Na retention. →Parathormone elevates the serum calcium level and promotes phosphorus excretion. →Kidney regulates acid-base balance by excreting either hydrogen or bicarbonate.
- 32. IMBALANCE IN FLUIDS AND ELECTROLYTES A. FLUID VOLUME DEFICIT Causes: -vomiting -diarrhea -GI suction -decreased fluid intyake -hemorrhage -3rd-space fluid shifts (fluids moves from vasculature into interstitial spaces and is unavailable for use. S/Sx: -acute weight loss -decresed skin turgor -oliguria -concentrated wine -weak, rapid pulse -decreased BP -increased Blood Urea Nitrogen (BUN) Treatment and Nursing Implications: -ISOTONIC IV FLUIDS (eg. Normal Saline, Ringers Lactate) -Tx of shock -monitor urinary output, BP -daily weights
- 33. B. FLUID VOLUME EXCESS Causes: -renal failure -Congestive Heart Failure (CHF) -cirrhosis or Liver failure -rapid excessive infusion of IV fluids S/Sx: -acute weight gain -edema -distended neck veins -rakes (moist crackles) -decreased BUN due to dilution Treatment and Nursing Implications: -Administers diuretics as ordered: Monitor for electrolyte imbalance -Low-sodium diet (avoid processed meats, canned soups and vegetables, table salt) -Restrict fluid intake; strict I and O - Maintain in Semi-Fowlers position -Assess breath sounds frequently -Check the pitting edema -Daily weights
- 34. HYPONATREMIA ( Serum Na < 135mEq/L) ETIOLOGY: 1. H2O intake 2. Na loss 3. Na intake CLINICAL EYE: Central Nervous System Activity— increase reflexes (hyper reflexia), apathy depression, head ache, disorientation, confusion (especially in adults), convulsion, decrease LOC (Lethary-Stupor-Coma) signs of increase ICP (if cerebral edema is present), decrease level of alertness Neuromuscular Activity—muscle weakness (earliest symptoms), muscle twitching, abdominal cramps SIGNS OF DECREASING BLOOD VOLUME: BP , CR , RR , PR , temperature, cold clammy diaphoresis skin. No thirst, CVP (Central Venous Pressure), UO (Urinary Output) Dx’c EXAMS: -Hct (hematocrit) -Hb (hemoglobin) -RBC (red blood cells) -Na < 135 mEq/L Na= 135 mEq/L Serum Osmolarity < 265 mEq Osmotic pressure in blood Attraction of H2O in blood Filtration Pressure Blood Volume S/S: edema formation, Hypovolemia potential, ICP projectile vomiting, head ache Hct,Hb,RBC– cold, clammy skin diaphoresis
- 35. HYPOKALEMIA ( K< 3.5 mEq/L) Causes:-diarrhea -vomiting -GI suction -Diuretics S/Sx: -fatigue -muscle weakness -nausea and vomiting -dysrhytmias -flat T wave accompanied by ST segment depression on ECG -Predisposed to digitalis toxicity Treatment and Nursing Implication: -Administer potassium supplements P.O. (oral) or IV (maximum 20mEq/hr in diluted IV solution, never give IV push (bolus) -Encourage potassium rich foods (bananas, apricots, cantaloupes, oranges, nuts, dark leafy greens, dried fruits) -Monitor ECG -If patient receiving digoxin, assess for digitalis toxicity (bradycardia, confusion, dysrhytmias, blurred or “white, green, yellow vision) -Provide for safety when ambulating, due to weakness HYPERKALEMIA ( > 5mEq/L ) Causes: -renal failure -acidosis -burn -salt substitute S/Sx: -muscle weakness to flaccid -paralysis -Intestinal colic -Elevated T wave on ECG Treatment and Nursing Implications: -Administer Na polystyrene sulfonate (kayexalate) by mouth or enema -Administer calcium gluconate IV -Aminister D10 W (10% dextrose in water) and regular insulin IV -Dialysis -Monitor ECG pattern for dysrhythmias -Restrict potassium in diet -Monitor for adequate urinary output
- 36. HYPOCALCEMIA ( < 9 mg/dL or 4.5 mEq/L) Causes: -hypoparathyroidism - mal absorption - Vit. D deficiency -Incedental removal of a trauma to parathyroid glands during thyroidectomy or radical reck surgery S/Sx: -circumoval tingling -Chvostek’s sign -numbrens in finger and toes -seizures -Trousseau’s sign Treatment and Nursing Implication: -Administer calcium gluconate P.O. (oral) or slow IV (intravenously); give oral form before meals with milk. -Administer alendronate (Fosamax), which slows abnormal and normal bone reabsorption in inhibiting bone formation and mineralization. It is used for treatment and prevention of ‘osteoporosis’ in postmenopausal women and osteoporosis in men. -Observe seizure -Assess the positive Trousseu’s and Chvostek’s signs. HYPERCALCEMIA ( > 11mg/dL or 5.5 mEq/L) Causes: -hyperparathyroidism -prolonged immobilization -malignant neoplastic disease -excess calcium supplements in the body S/Sx: -muscle weakness -constipation -nausea and vomiting -cardiac dysrhythmias -renal calculi Treatment and Nursing Implications: -encourage fluids -Administer phosphorus P.O. or IV -Administer calcitonin subscutaneously or IV -Monitor ECG -Encourage high-fiber diet to prevent constipation -Assess the renal colic
- 37. NORMAL ARTERIAL BLOOD GASES pH= 7.35-7.45 HC O3= 22-26 mEq/L P O2= 80-100 mmHg P CO2= 35-45 mmHg O2 Sat.= 95%-100% or 98%-100% METABOLIC ACIDOSIS Causes: →Diabetes Mellitus (fat used for energy, ketones produced) →Starvation (fat used for energy, ketones produced) →Shock, Myocardial Infarction (lock of oxygen results in anaerobic metabolism producing lactic acid and hypotension) →Renal failure (potassium and hydrogen ions retained) →Acetylsalicylic acid overdose (acid producing) →Diarrhea (bicarbonate base lost) →Intestinal fistula (bicarbonate base lost) S/Sx: -confusion -headache -drowsiness -kussmaul’s respiration -decreased cardiac output -bicarbonate level < 22 mEq/L - PCO2 normal or 35mmHg, if compensating -pH < 7.35 METABOLIC ALKALOSIS Causes: →vomiting (loss of HCl) →GI suction (loss of HCl) →Hyperaldosteronism (aldosterone retains Na; K is secreted in the urine and hydrogen ions always follow potassium, thus possibly causing metabolic acidocis) →Cushing’s syndrome (too much steroids) S/Sx: - increased muscle irritability -tetany -slow,shallow respirations -disorientation -seizure -pH >7.45 -PCO2 normal, or >45 mmHg, if compensating -Bicarbonate level > 26 mEq/L
- 38. RESPIRATORY ACIDOSIS Causes: →Chronic Obstructive Pulmonary Disease (COPD) →Any condition that interferes with O2/CO2 exchange in the lungs →Drug overdose (respiratory depression) S/Sx: -dizziness -confussion -palpitation -headache -ventricular fibrillation -decreased cardiac output -pH < 7.35 -drowsiness -PCO2 > 45 mmHg -HCO3 normal or > 26 mEq/L, if compensating Treatment and Nursing Implications: -Administer O2 -Administer Na HCO3 (IV) RESPIRATORY ALKALOSIS Causes: → high fever with rapid respiratory rate →hyperventilate S/Sx: -lightheadedness -palpitation -increased muscle irritability -pH > 7.45 -HCO3 normal or < 22mEq/L, if compensating Treatment and Nursing Implication: -re-breathing bag -control elevated temperature with antipyretics
- 39. THE DIVERSITY OF THE ENDOCRINE SYSTEM ACTH- Adrenocorticotropic hormone ANF - Atrial natriuretic factor cAMP- Cyclic adrenaline monophospate CBG - Corticosteroid-binding globulin CG - Chorionic gonadotropin cGMP- Cyclic guanosine monophosphate CLIP - Corticotropin -like intermediate lobe peptide DBH - Dopamine β- hydroxylose DHEA- Dehydroepiandrosterone DHT - Dihydrotosterone DIT - Diiodotyrosine DOC - Deoxycorticosterone EGF - Epidermal Growth factor FSH - Follicle-stimulating hormone GH - Growth hormone IGF-I - Insulin –like growth hormone factor-I LH - Luteotropic hormone MSH - Melanocyte –stimulating hormone TBG - Thyroxine-binding Globulin TSH - Thyrotropin-stimulating hormone
- 40. Several of multicellular organisms depends on their ability to adapt to a constantly changing environment. - Intracellular communication mechanism are necessary requirements for this adaptation - It is govern by nervous system and the endocrine system NERVOUS SYSTEM Provide on fixed communication system ENDOCRINE SYSTEM Supplied hormones, which are mobile messages. “Hormone” G.W means to arouse to activity. - Is a substance that is synthesizes in one organ and transported by the circulatory system to act on another tissue. - Can act on adjacent cells (PARACRINE action) - Can act on the cell which they mere synthesized (AUTOCRINE action) without entering the systemic circulation. - It is a blood burn substance and transported through circulation and has a specific target organ or tissue. TARGET CELL CONCEPT 1. Determinants of the concentration at a hormone at the target cell. a. The rate of synthesis and secretion of the hormones. b. The proximity of the target cell to the hormone source (dilution effect). c. The dissociation constants of the hormone with specific plasma transport protein (if any). d. The conversion of inactive or sub optimally active forms of the hormone in the fully active form. e. The rate of clearance from plasma by other tissue or by digestion, metabolism, or excretion.
- 41. 2. Determination of the target all response. a. The number, relative activity, and state of occupancy of the specific receptors on the plasma membrane or in the cytoplasm or nucleus. b. The metabolism (activation or inactivation) of the hormone in the target cell. c. The presence of other factors within the cell that are necessary for the hormone response. d. Lep – or – down – regulation of the receptors consequent to the interaction with the lizard. e. Postreceptor desensitation of the cell, including down – regulation of the receptor. RECEPTORS Cell-associated recognition molecules HORMONES - Initiate their biologic effects by binding to specific receptors. NOTE: hormone induced action generally terminate when the effector dissociates from the receptor. TARGET CELL - Has its ability to selectively bind a given hormone to its congnate receptor. - Several biochemical features of interaction are important in order for hormone – receptor interactions to be physiologically relevant. 1. Binding should be specific. Ex. Displaceable by against or antagonist. 2. Binding should be saturated. 3. Binding should occur within the concentration range of the expected biologic response. Polypeptide and protein hormone and the catecholamines bind to receptors in the plasma membrance and thereby generate a signal that regulates various intracellular functions by changing the activity of an enzyme. Steroid, retinoid and thyroid hormones interact with intracellular receptors and it is this lizard – receptor complex that directly provides the signal.
- 42. Receptor – effector corepling - Provides the first step in amplification of the hormonal response. Hormones are synthesized in discrete organs designed safety for this specific purpose: - Thyroid – triiodothyronine - Adrenal o Glucocorticoids o mineralocorticoids Pituitary - TSH Growth hormone - FSH Prolactin - LH ACTH Some organ are designed to perform two distinct but closely related functions - Organics produces o mature oocytes o Reproductive hormones Estradiol Progesterone - Testes produces o Mature spermatozoa o Testosterone Hormones are also produced in specialized cells within other organs such as: - Small intestine o Glucagon Like peptide - Thyroid o Calcitonin - Kidney o Angiotensin II Some hormone requires the parenchymal cells of more than one organ such as: - Skin, - Liver, - Kidney, are required for the production of 1,25 (OH)2 – D3 (calcitriol)
- 43. SUMMARY The presence of a specific receptor defines the target cells for a given hormone. Receptors are proteins that bird specific hormones and generate an intracellular signal (receptor – effector - coupling). Some hormones have intracellular receptors; others bird to receptors on the plasma membrane. Hormones are synthesized from a number of precursor molecules, including cholesterol, tyrosine perse, and all the constituent amino acids of peptides and proteins. A number of modification processes alter the activity of hormones. For example, many hormone are synthesized from larger precursor molecules. The compliment of enzymes in a particular cell type allows for the production of a specific class of steroid hormone. Most of the lipid – soluble hormones are found to rather specific plasma transport proteins.
- 44. GLAND HORMONE CHEMICAL CLASS ACTION REGULATED BY Pineal Gland Metanonin Amine Involved in rhythmic activities Light/dark cycles Hypothalamus Pituitary Gland - Posterior lobe (releases hormones made by the hypothalamus) Oxytocin Antidimetric hormone (ADH) Peptide Peptide Stimulates contraction of uterus.The milk “let down” reflex Promotes retention of water by kidney Hypothalamus (Nervous System) In response to Uterine stretching And/or suckling of baby Hypothalamus in response to water/salt imbalance Anterior lobe Growth hormone (GH) Prolactin (PRL) Protein Protein Stimulates growth (specially of bones and muscles and metabolism) Stimulates milk production Hypothalamic releasing and inhibiting hormones Hypothalamic hormones
- 45. Follicle Stimulating Hormone (FSH) Luteinizing hormone (LH) Thyroid stimulating hormone (TSH) Adrenocorticotrop ic hormone (ACTH) Protein Protein Protein Protein Stimulates production of ova and sperm Stimulates ovaries and testes Stimulates thyroid gland Stimulates adrenal cortex to secrets glucocorticoids Hypothalamic hormones Hypothalamic hormones Thyroxine in blood. Hypothalamic hormones Glucocorticoids Hypothalamic hormones Thyroid gland Thyroxine (T4) Triiodothyroxine (T3) calcitonin Amine Amine Peptide -Stimulates metabolism -reduce blood calcium level TSH Calcium level in blood Parathyroid glands Parathyroid hormone Peptide Raise blood calcium level Calcium level in blood Thymus Thymosin Peptide “programs” T cells Not known Adrenal glands Epinephrine Steroids -Increase Nervous system
- 46. -adrenal medulla Norepinephrine blood glucose -Increase rate of metabolism -Constrict certain blood vessels (sympathetic division) Adrenal cortex Glucocorticoids Mineralocorticoids Steroids -increase blood glucose -promotes reabsorption of Na+and secretion of K+ in kidney - ACTH -Changes on blood volume or blood pressure , K+ and Na+ level in blood Pancreas Insulin Glucagon Protein Protein -reduces blood glucose - increases blood glucose Glucose level in blood Gonads -testes Androgens Steroids Support sperm formation dev. & maintenance of male 2 degree sex characteristis FSH LH Ovaries Estrogen Steroids -Stimulates uterine lining growth- development and maintenance of female 2 FSH LH
- 47. Progesterone Steroids degree sex characteristics -promotes growth of uterine lining FSH LH Estrogen- stimulates development of ductile structure of the breast. Progesterone- stimulates the development of the acinal structure of the breast. Human Placental Lactogen- promotes breast development during pregnancy. Oxytocin- Let-down reflex. This is inhibited by progesterone. Prolactin- stimulates milk production. This is inhibited by estrogen. Testosterone- hormone which stimulates spermatogenesis and is responsible fpr the development. Leydig cells- release testosterone and other interstitial androgens.
- 48. Functions of Dietary Proteins 1. Synthesize tissue proteins of the body - Maybe utilized for the production of energy and maybe converted to CHO and fats. 2. For growth and tissue repair - Quality of proteins taken in diet is more important than the quantity concerned. - Good quality CHON has many or complete essential amino acids Classification of Quality of Proteins 1. Complete proteins - ( ex. Animal proteins such as meat ) 2. Incomplete protein – (ex. Vegetable protein ) Protein factors in Nutrition can be studied by: 1. Quality of CHON 2. Quantitative of CHON or Quantitative Aspect Quality of Proteins can be discussed by the ff. 1. Biological value of CHON 2. Amino acid composition of the dietary CHON 3. Balance of dietary amino acid 4. Availability of amino acid from food 5. Supplementary relationship of amino acids Biological value of CHON - % of absorbed nitrogen which is retained in the body Amino acid composition of CHON - The concept is : CHON should have complete essential amino acids and have a good biological value of CHON so that they can be utilized for protein synthesis.
- 49. Effect if the protein intake does not meet the immediate requirements, Protein Anabolism cannot be maintained at the required rate in our body 1. Growth is retarded ( in children ) 2. Weight is lost ( in children ) 3. Wound healing is delayed 4. If the deficiency is worked, excessive amount of fats may accumulate in the liver Causes ‘fatty liver. Fatty liver is d/t choline deficiency, a consequence of methionine deficiency Impaired ‘apoprotein synthesis’ Lipoprotein formation Fatty liver Fibrosis of the liver Liver cirrhosis CANCER OF A LIVER Cause of Bleeding Disorders Prolong Deficiency of CHON Inadequate synthesis of plasma CHON Fibrinogen deficiency BLEEDING DISORDER
- 50. 5. Causes edema and increase susceptibility to shock Decrease in plasma albumin Edema Decrease fibrinogen Bleeding Shock 6. Endocrine abnormalities may appear Ex. Gonadotropin deficiency – amenorrhea 7. Resistance to infection may be diminished 8. Ex. Impaired capacity for forming gamma-globulins antibodies ( IgG’s) Role of Carbohydrates in Diet 1. Energy producer / Source of energy - Glucose, fructose, galactose and mannose ( minor dyres ) Ribose, deoxyribose-required for nucleic acid synthesis
- 51. Basic Functions of Food ( Nutrients ) Nutrients Function Carbohydrates - Energy production Fats - Energy production Proteins - Energy production - Protection against infections -Body building (growth ) repair and maintenance Vitamins - Protection against infections -Regulation of tissue functions Minerals - Body building (growth ) repair and Maintenance - Regulation of tissue functions Water - Body building (growth ) repair and Maintenance - Regulation of tissue functions
- 52. MARASMUS - Results of starvation in small children - Calories became the most limiting factor ( nature of diet ) - Infant survives on utilizing its own tissues Causes: - Excessive Bf infant of a malnourished mother - Milk is grossly reduced - Prolong BF with inadequate supplementation of food Pre-disposing - Premature babies-Malformations of mouth and nose -Local disease Age: - < 1 y.o S/Sx: - Retarded growth, emaciated, under weight -No edema - Depleted of subcutaneous fats and muscle -Hair thin - Hungry and cries continuously -‘little monkey’ face - LBM and vomiting -Dehydration and electrolyte imbalance - Hungry diarrhea- small dark green mucous stools - Skin is thin, flaccid and wrinkled, bony prominence are marked - Reddish mucous membrane in the mouth
- 53. KWASHIORKOR - d/t very low in CHON,very low in protein but provides enough calories to satisfy the need of a child - CHON became the most limiting factors and not calories - CHON lack is quantitative and also qualitatively of low biological value Causes: - Artificially fed and weaned children -Low quality of cottons are fed - Occurs weeks or months after weaning - No milk, egg, etc. Pre-disposing factors: - Cases of all most infections -Measles - Acute diarrhea -Respiratory infection Age: -Older children: in 2nd/3rd year of life S/Sx: - Growth retarded, not emaciated but looks blown up d/t edema - Early sign: Apathy and Anorexia - Lens lively and refuse to eat - Lesion in skin, patches of hypigmentation - Pitting edema -Dry and thin hair - Flag sign ~> de pigmented alternate with more pigmented hair
- 54. ROLE OF LIPIDS IN THE DIET Lipids - Provide energy - ‘carriers of certain fat soluble vitamins ( A,D,E and K ) provitamins - ‘minor’ proteinsposing effect Linoleic Acid - Fats or oil form seeds and coconut oil. Arachidonic Acid - Fats of animal origin Maintenance Requirement of Fluid on Caloric Expenditure Body Weight 3-10 10-20 More than 20 Caloric Expenditure 100 cal/kg/d 1,000 cal +50 cal/kg for each kg of body wt. more than 10kg 1,500 cal+20 cal/kg for each kg of body wt> 20kg Daily Fluid Requirement 100ml/kg 1,000 ml +50 ml/kg for each kg of body wt> 10kg 1,500ml +20 ml/kg for each kg of body wt> 20kg
- 55. HYPOMAGNESEMIA (Mg < than 1.5 mEq/L) Causes: -Diabetes ketoacidosis -Alcoholism -Abnormal digestion S/Sx: -Neuromuscular irritability -Weakness -CNS affection -Disorientation -Hallucination -Seizure Treatment and Nursing Diagnosis: -Administer of magnesium sulfate HYPERMAGNESEMIA (Mg > 2.5 mEqL) Causes: -Renal failure -Medication of magnesium hydroxide S/Sx: -Flushing -Hypotension -Hypo active reflex -Depress respiration -Cardiac arrest Treatment and Nursing Diagnosis: -Administer calcium gluconate
- 56. Republic of the Philippines LagunaStatePolytechnicUniversity MAIN CAMPUS Brgy.Bubukal, Santa Cruz, Laguna A.Y. 2013-2014 Submitted by: Birador, Roxanne Mae E. Abayari, Maureen Linatoc, Thelma Jean Submitted to: Sir Elmo Maagad