
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Etiopathogenesis Urinary bladder malignancy
Semelhante a Etiopathogenesis Urinary bladder malignancy (20)
Mais de GovtRoyapettahHospit
Mais de GovtRoyapettahHospit (20)
Último
Último (20)
Etiopathogenesis Urinary bladder malignancy
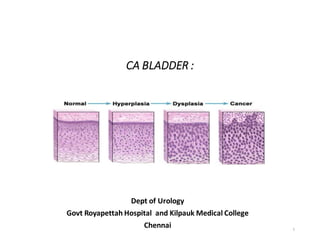
- 1. CA BLADDER : Dept of Urology Govt Royapettah Hospital and Kilpauk Medical College Chennai 1
- 2. Moderators: Professors: • Prof. Dr. G. Sivasankar, M.S., M.Ch., • Prof. Dr. A. Senthilvel, M.S., M.Ch., Asst Professors: • Dr. J. Sivabalan, M.S., M.Ch., • Dr. R. Bhargavi, M.S., M.Ch., • Dr. S. Raju, M.S., M.Ch., • Dr. K. Muthurathinam, M.S., M.Ch., • Dr. D. Tamilselvan, M.S., M.Ch., • Dr. K. Senthilkumar, M.S., M.Ch. Dept of Urology, GRH and KMC, Chennai. 2
- 3. • EPIDEMIOLOGY • ETIOPATHOGENESIS • CLASSIFICATION, • CLINICAL FEATURES, • HISTOPATHOLOGY OF BENIGN & MALIGNANT TUMOR 3 Dept of Urology, GRH and KMC, Chennai.
- 4. EPIDEMIOLOGY 4 Dept of Urology, GRH and KMC, Chennai.
- 5. 5 Dept of Urology, GRH and KMC, Chennai.
- 6. M>F - More prevalence of smoking and exposure to environmental toxins • Adolescents and young adults - develop well-differentiated non invasive, rather than invasive bladder cancer 6 Dept of Urology, GRH and KMC, Chennai.
- 7. ETIOLOGY • Genetic abnormalities • External risk factors • Smoking • Nutritional factors • Fluid intake • Inflammation •Chemotherapy, Radiation. 7 Dept of Urology, GRH and KMC, Chennai.
- 8. Genetic • Several polymorphisms - related & susceptibility to environmental carcinogen • N-acetyl transferase (NAT) & slow NAT-2 polymorphism is related to bladder cancer • Glutathione-S transferase (GSTM1) conjugates arylamines and nitrosamines. • The null GSTM1 and slow NAT-2 lead to high levels of 3- aminobiphenyl - higher risk of bladder cancer. 8 Dept of Urology, GRH and KMC, Chennai.
- 9. N-acetyl transferase (NAT) detoxifies nitrosamines, a known bladder carcinogen. NAT-2 regulates the rate of acetylation of compounds such as caffeine, which are related to bladder cancer formation. Glutathione-S transferase (GSTM1) conjugates several reactive chemicals, including arylamines and nitrosamines. 9 Dept of Urology, GRH and KMC, Chennai.
- 10. Genetic Abnormalities Protooncogenes expression - Ras, p21 Tumour suppressor gene mutation - p53, p21, p27 LOH of chromosome 9 Abnormalities of specific cell cycle regulatory proteins CABLES, k167,cyclinD 10 Dept of Urology, GRH and KMC, Chennai.
- 11. External Risk Factors • Exposure of chemical Dye and Rubber industries • Primary culprits -- Aromatic amines that bind to DNA . Benzidine and β-naphthylamine , • Polycyclic aromatic hydrocarbons (PAH), diesel exhaust, and paint substances • Environmental carcinogens –by inhalation or through skin absorption 11 Dept of Urology, GRH and KMC, Chennai.
- 12. 12 Dept of Urology, GRH and KMC, Chennai.
- 13. 13 Dept of Urology, GRH and KMC, Chennai.
- 14. Smoking •The intensity and duration of smoking is linearly related to the increased risk, with no clear plateau level •Black tobacco appears to be worse than blonde tobacco because of a greater amount of aromatic amines in the former •30 % Bladder Cancer associated with smoking •Risk correlates with number, duration, degree of inhalation 14 Dept of Urology, GRH and KMC, Chennai.
- 15. Nutritional Factors • Moderately higher in coffee and tea drinkers • Mediterranean diet -- Lowest urothelial cancer risk • Fruits and vegetables— Polyphenols,& antioxidants, are important in detoxification. Can prevent DNA adduct formation and oxidative damage • Micronutrients & antioxidants Vitamins A, C and E; selenium and zinc 15 Dept of Urology, GRH and KMC, Chennai.
- 16. Inflammation • Chronic infection with Schistosoma hematobium leads to formation of Squamous cell carcinoma • Chronic indwelling catheter , stones, and infections • Chronic urinary tract infections Escherichia coli and Pseudomonas 16 Dept of Urology, GRH and KMC, Chennai.
- 17. Chemotherapy • Related to the duration and intensity of cyclophosphamide Mutagenic metabolic – Phosphoramide mustard . • Up to ninefold increased risk • High grade, muscle infiltrating, younger, equal in both sexes • Latency period = 6 to 13 years • Uro protectant - MESNA (2-Mercaptoethanesulfonic acid) 17 Dept of Urology, GRH and KMC, Chennai.
- 18. 18 Dept of Urology, GRH and KMC, Chennai.
- 19. 19 Dept of Urology, GRH and KMC, Chennai.
- 20. • Radiation Increased risk in patients with prostate or cervical cancer treated with RT • Heredity First-degree relatives -- twofold increased risk 20 Dept of Urology, GRH and KMC, Chennai.
- 21. • Fluid Intake Increased fluid intake Decrease the concentration of potential carcinogens Decrease the risk of bladder cancer Consumers of artificial sweeteners, alcohol intake, phenacetin - No evidence of Risk • BMI-Causes hyperinsulimia –increases-growth factors • Pioglitazone –increses cancer risk 21 Dept of Urology, GRH and KMC, Chennai.
- 22. 22 Dept of Urology, GRH and KMC, Chennai.
- 23. PATHOPHYSIOLOGY Urothelium 3-7 layers thick BM Lamina propria - muscularis mucosa, blood vessels, lymphatic, nerves Muscularis propria- inner longitudinal, middle circular, and outer longitudinal Serosa 23 Dept of Urology, GRH and KMC, Chennai.
- 24. 24 Dept of Urology, GRH and KMC, Chennai.
- 25. Term usingfor.... Hyperplasia :-increase in no of cell layers without nuclear or cellular abnormalities. Atypical hyperplasia: -Increase in no of cells with nuclear or cellular changes Metaplasia: - change in epithelium with squamous or adenomatous development. Mild to moderate nuclear & cellular atypia Dysplasia: abnormal histology or anatomical structure -Epithelial changes that are intermediate between normal urothelium and CIS (severe dysplasia) - Isolated dysplasia – 19% CIS & 15% TCC - Dysplasia with previoush/o UC – 60% CIS 25 Dept of Urology, GRH and KMC, Chennai.
- 26. Pathogenesis of urothelial cancer formation 26 Dept of Urology, GRH and KMC, Chennai.
- 27. 27 Dept of Urology, GRH and KMC, Chennai.
- 28. Pathogenesis of urothelial cancer formation • Somatic mutations - more common than germline mutations • Accumulation of the genetic event - phenotypic changes results unregulated cell growth and invasion 28 Dept of Urology, GRH and KMC, Chennai.
- 29. • Lowgrade papillary tumors - genomic stability allows tumor recurrence • Genetic alterations - fibroblast growth factor receptor–3 , deletions of 9p and 9q. • High-grade papillary cancer and CIS - unstable genomes Genetic alteration - HRAS, FGFR, 5q-, 6q-, 7q+ 29 Dept of Urology, GRH and KMC, Chennai.
- 30. CLASSIFICATION • WHO 1973 – G1/G2/G3, based on degree of cellular & architectural atypia • WHO/ISUP 1998 – introduction of term PUNLMP define Papilloma, PUNLMP, CaLG, CaHG 30 Dept of Urology, GRH and KMC, Chennai.
- 31. • WHO 2004 – introduction of low grade & high grade PUC PUNLMP term adopted by WHO clear Histological features of UC & dec. the diagnostic subjectivity of the WHO 1973 scheme • WHO 2004/2016 – Division of pT1 tumors into LG & HG - further differentiate Non-invasive LG & HG papillary car. from Invasive urothelial carcinoma 31 Dept of Urology, GRH and KMC, Chennai.
- 32. 32 Dept of Urology, GRH and KMC, Chennai.
- 33. 33 Dept of Urology, GRH and KMC, Chennai.
- 34. classifications & percentage 34 Dept of Urology, GRH and KMC, Chennai.
- 35. 35 Dept of Urology, GRH and KMC, Chennai.
- 36. 36 Dept of Urology, GRH and KMC, Chennai.
- 37. 37 Dept of Urology, GRH and KMC, Chennai.
- 38. 38 Dept of Urology, GRH and KMC, Chennai.
- 39. Histology Non–muscle-invasive bladder cancer (NMIBC) includes – Papillary urothelial neoplasia of low malignant potential (PUNLMP), Low- and high-grade urothelial cancer CIS ( carcinoma in situ) previously been called “superficial bladder cancer 39 Dept of Urology, GRH and KMC, Chennai.
- 40. 40 Dept of Urology, GRH and KMC, Chennai.
- 41. EPIDEMIOLOGY • 9th most common cancer world wide • Cancer of environment and advancing age • Peak Incidence - 8th decade of life • Strong association with environmental toxins 41 Dept of Urology, GRH and KMC, Chennai.
- 42. Papillary urothelial neoplasia of low- malignant potential (PUNLMP) • Papillary growth with minimal cytological atypia more than seven cells thick • Solitary and located on the trigone 42 Dept of Urology, GRH and KMC, Chennai.
- 43. PUNLMP • Composed of thin papillary stalks • Polarity of the cells is maintained • Nuclei are minimally enlarged. • Low proliferation, non invasive, non metastatic 43 Dept of Urology, GRH and KMC, Chennai.
- 44. PUNLMP 44 Dept of Urology, GRH and KMC, Chennai.
- 45. HGPUC • Fused papillary stalks with high-grade cancer in the urothelial layer. • Disordered growth pattern, numerous mitotic figures pleomorphic cells with exaggerated nuclei. • Over 80% of high-grade cancers will invade the underlying stroma 45 Dept of Urology, GRH and KMC, Chennai.
- 46. HGPUC 46 Dept of Urology, GRH and KMC, Chennai.
- 47. 47 Dept of Urology, GRH and KMC, Chennai.
- 48. Tumor suppressor genes Low grade papillry CIS and muscle invasive High grade papillary and Muscle invasive TP53 mutations (17p13) Uncommon Hallmark- 60% Hallmark- >50% PTEN (10q23) Rare Hallmark Hallmark- 30-35% RB gene (13q14) Rare Hallmark Hallmark-37% Deletions of Ch regions 9P16, 9p21 Hallmark Absent in pure CIS 70-80% Loss of heterozygosity (LOH) of Ch 9 >50% Rare Rare 48 Dept of Urology, GRH and KMC, Chennai.
- 49. proto oncogenes Low grade papillry CIS and muscle invasive High grade papillary and Muscle invasive Alterations in the fibroblast growth factor receptor–3 (FGFR-3) - 4p16 Hallmark-75% Infrequent-20% Common Deletions -9p14, 9q11-13, 9q33-34 Hallmark Absent in pure CIS 70-80% H RAS mutations- (11p15) 15% 10-15% 10-15% Point mutations in PIK3CA (3q26) 16% Rare Rare Over expression of C-Erb B2 (7q) Uncommon 10-14% 10-14% 49 Dept of Urology, GRH and KMC, Chennai.
- 50. BENIGN LESIONS/ TUMORS OF THE BLADDER • EPITHELIAL METAPLASIA • LEUKOPLAKIA • INVERTED PAPILLOMA • PAPILLOMA • NEPHROGENIC ADENOMA • CYSTITIS CYSTICA AND GLANDULARIS • LEIOMYOMA 50 Dept of Urology, GRH and KMC, Chennai.
- 51. EpithelialMetaplasia • Focal area of transformed urothelium surrounded by normal urothelium • Normal cellular & nuclear architecture • Location- trigone Composed of squamous (Squ.metaplasia) or glandular (glan Metap. ) 51 Dept of Urology, GRH and KMC, Chennai.
- 52. ON CYSTOSCOPY- knobby app.covered by white flaky, easily disrupted & lying on the trigone Glandular Metaplasia appears as clumpy, raised, reddish area that look like inflammatory, often confused for cancer Approx 40% female 5% male have Squ. Metaplasia of the bladder Biopsy & t/t not required. 52 Dept of Urology, GRH and KMC, Chennai.
- 53. Leukoplakia • Similar to Squ. Metaplasia with the addition of • Keratin deposition that appears as a white flaky substance floating in the bladder • Benign lesion, 53 Dept of Urology, GRH and KMC, Chennai.
- 54. 54 Dept of Urology, GRH and KMC, Chennai.
- 55. • Symptoms- vesical irritation & passage of flakes • Premalignant • Careful cystoscopic assessment & biopsy • May require resection. 55 Dept of Urology, GRH and KMC, Chennai.
- 56. A. Epithelial metaplasia B. Leukoplakia 56 Dept of Urology, GRH and KMC, Chennai.
- 57. Benign proliferative lesions Inverted Papilloma • Associated with -Chronic inflammation -Bladder outlet obstruction. • Located throughout the bladder -Most common – Trigone -Less than 1% of all bladder tumors 57 Dept of Urology, GRH and KMC, Chennai.
- 58. • Present with non-specific hematuria or irritative voiding symptoms • May be asso. with urothelial cancer or malignant changes • Recurrence – 1% 58 Dept of Urology, GRH and KMC, Chennai.
- 59. InvertedPapilloma...... • Gross: - usually smooth, solitary, polypoid, sessile or pedunculated - Usually < 3 cm - multiple lesions – 1.5 to 4.5% • Microscopic ( Histologic ) - smooth surface & base with minimal to absent exophytic components - no/minimal cytologic atypia 59 Dept of Urology, GRH and KMC, Chennai.
- 60. • DDx: - Urothelial cancer with inverted growth pattern - Papillary urothelial neoplasm of LMP • FISH – differentiate b/w benign & malignant • Treatment - Transurethral resection 60 Dept of Urology, GRH and KMC, Chennai.
- 61. Inverted Papilloma..... • Two main subtypes: 1. Trabecular subtype ( classic type) - irregular, downward growth - consisting of cords & trabeculae as a sheets arising from the urothelial layer growing into the lamina propria 2. Glandular subtype - morphologically overlap with Cystitis cystica 61 Dept of Urology, GRH and KMC, Chennai.
- 62. 62 Dept of Urology, GRH and KMC, Chennai.
- 63. 1. Inverted growth pattern of papillary 2. Inverted growth pattern of lining cells fronds of typical inverted Papilloma with central streaming & peripheral composedof intact surface of bladder palisading without any atypia and urothelium. ( H&E ; X10 ) mitosis. ( H&E ; x40 ) 63 Dept of Urology, GRH and KMC, Chennai.
- 64. Papilloma • Discrete Papillary growth with a central fibrovascular core lined by normal urothelium • Small, single, exophytic lesion • Younger pts ( mean age- 46yrs) 64 Dept of Urology, GRH and KMC, Chennai.
- 65. Posterior or lateral wall (close to UO) R/F similar to urothelial cancer C/F- asymptomatic, Hematuria Benign behaviour, may recur but not progress or invade the bladder T/t – TUR of lesions 65 Dept of Urology, GRH and KMC, Chennai.
- 66. Papilloma..... • Gross: - Soft, pink, small isolated growth with discrete papillary structure - Usually pedunculated, mean 3 mm • Microscopic(Histologic): - Discrete Papillary fronds, minimal branching & fusion, benign cells - Papillae appear to float above urothelial surface - Papillae usually small with scant stroma & slender fibrovascular cores - Lined by normal urothelium with prominent umbrella cells 66 Dept of Urology, GRH and KMC, Chennai.
- 67. • Molecular/cytogenetic discription: - Negative stain – p53 & RB . Positive stain – CK-20 - Diploid , 75% cases are FGFR3 mutations 67 Dept of Urology, GRH and KMC, Chennai.
- 68. DDX:PUNLMP: it has a thicker cell layer, large nuclei with occasional mitotic figures, recurrence- 20-30% 68 Dept of Urology, GRH and KMC, Chennai.
- 69. Nephrogenic Adenoma • Chronic irrigation of the urothelium - Trauma - Previous surgery - Renal transplantation - Intravesical chemotherapy - Stones, catheters & infection - Immunosuppression • Associated with inflammation 69 Dept of Urology, GRH and KMC, Chennai.
- 70. Nephrogenic Adenoma...... • Usually adults, • more common at bladder neck, 15% prostatic urethra • In renal transplant recipients, derived from exfoliated & implanted renal tubular cells in the bladder • In other pts, appear to be metaplastic and not a neoplasm • Involve mucosa & submucosa 70 Dept of Urology, GRH and KMC, Chennai.
- 71. Clinical features: • Gross hematuria, irritative voiding symptoms • Valvety app on cystoscopy, often mistaken for papillary urothelial car. • Benign, no malignant transformation 71 Dept of Urology, GRH and KMC, Chennai.
- 72. Neohrogenic adenoma..... • Gross: - Polypoid, sessile or Papillary, 20% multiple • Microscopic (Histologic): - small hollow tubules, on EM – similar to PCT - usually lined by single layer of Cuboidal or Hobnail cells - clear or eosinophilic cytoplasm, small nuclei, no prominent nucleoli 72 Dept of Urology, GRH and KMC, Chennai.
- 73. 73 Dept of Urology, GRH and KMC, Chennai.
- 74. IHC: Positive stains – PAX-2, PAX-8 Negativestains – p16 CK-7 & CK-20 S100 PAS+, A1+ CD10 74 Dept of Urology, GRH and KMC, Chennai.
- 75. • DDx 1. Papillary urothelial car. multilayered, atypia, p16+ 2. Prostatic carcinoma : prostatic urethra may resemble & similar express AMACR+, but NA is PSA & PSAP –ve more atypia in PC 3. Urothelial car. Nested variant - cystic degeneration of nests, - multilayered, marked atypia - 75 Dept of Urology, GRH and KMC, Chennai.
- 76. Cystitis Cystica & Glandularis UreteritisCystica • Common incidental finding in bladder specimens • Reactive urothelial changes 76 Dept of Urology, GRH and KMC, Chennai.
- 77. • chronic Cystitis, • Bladder extrophy, • ureteral implantation, • neurogenic bladder or • any cause of mucosal irritation 77 Dept of Urology, GRH and KMC, Chennai.
- 78. Term using.... 1. Brunn nests : invagination from the overlying urothelium into lamina propria. 2. Cystitis Cystica: when Brunn nests become cystically dilated ( with or without eosinophilic secretions in the lumen) . 3. Cystitis Glandularis: when the urothelial cell nests show central cyst or lumen lined by columnar/ Cuboidal epithelium. 78 Dept of Urology, GRH and KMC, Chennai.
- 79. Cystitis Cystica& Glandularis HP image:all threepattern 79 Dept of Urology, GRH and KMC, Chennai.
- 80. HPspecimen: (a)CystitisCystica. (b)cystitis Glandularis 80 Dept of Urology, GRH and KMC, Chennai.
- 81. Cystitis Cystica& Glandularis.... • C/F – incidental finding in biopsies , - on cystoscopy – may present as papillary or polypoid mass - usually asymptomatic, recurrent UTI 81 Dept of Urology, GRH and KMC, Chennai.
- 82. Histological two types ; 1. Usual type – more common, express membranous beta-catenin 2. intestinal type – also called intestinal metaplasia - presence of goblet & mucin cells - express nuclear beta-catenin - risk of adenocarcinoma more Both type involved only lamina propria 82 Dept of Urology, GRH and KMC, Chennai.
- 83. • usual type – CK7+ , CDX2 & CK-20 –ve Intestinal type – CDX2 & CK-20 + ve • D/D-ADENOCARCINOMA • ENDOCERVICOSIS 83 Dept of Urology, GRH and KMC, Chennai.
- 84. • Treatment: removal of source of infection/injury long term antibiotics therapy Surgical options reserved when conservative Mx not respond. 84 Dept of Urology, GRH and KMC, Chennai.
- 85. HP specimens: CystitisGlandularis( usualtype) 85 Dept of Urology, GRH and KMC, Chennai.
- 86. 86 Dept of Urology, GRH and KMC, Chennai.
- 87. LEIOMYOMA • Rare benign Mesenchymal tumor • Till now, only 250 cases are reported • Similar incidence in male and female 87 Dept of Urology, GRH and KMC, Chennai.
- 88. Leiomyoma • Etiology is still unknown, but may be related to - chromosomal alteration - hormonal disturbance - Repeated bladder wall & detrusor infection - perivascular inflammation 88 Dept of Urology, GRH and KMC, Chennai.
- 89. • Based on location – 3 type 1. Endovesical - (65-85% ) 2. Intramural - ( 3-7% ) 3. Extravesical - ( 10-30% ) 89 Dept of Urology, GRH and KMC, Chennai.
- 90. Histopathologicalspecimens: (A) Proliferation of spindle shaped cells, Eosinophilic cytoplasm on H & E stain, No evidence of mitotic changes or atypia (B) Stain negatively for Ki-67 (C) Positive SMs staining for Actin 90 Dept of Urology, GRH and KMC, Chennai.
- 91. Clinical presentation (30%) • Obst. voiding symptoms (49%)- • Irrit. Voiding symptoms (38%) • Flank pain (13%) • Hematuria (11% ) 91 Dept of Urology, GRH and KMC, Chennai.
- 92. • Best imaging for diagnosis – MRI & cystoscopic biopsy • Treatment : Endovesical – TURBT Intramural & Extravesical – wide excision/partial cystectomy open/laparoscopic 92 Dept of Urology, GRH and KMC, Chennai.
- 93. On USG: Smoothwall, Homogeneous, hypoechoic, solid mass with echogenic surface On CT(P):Hypodense mass, CT(c): Moderately enhancingmass 93 Dept of Urology, GRH and KMC, Chennai.
- 94. Carcinomain situ(CIS) Flat, high grade , non- invasive urothelial cancer surface epithelium contains cancer cells • Spread – Distal ureters and prostatic urethra on the surface or in a pagetoid manner 94 Dept of Urology, GRH and KMC, Chennai.
- 95. • Urine cytology - 80- 90 % positive • 40 - 83% progress to muscle-invasive cancer • Endoscopically, - reddish with heaped-up mucosa can be mistaken for inflammatory changes or radiation cystitis. 95 Dept of Urology, GRH and KMC, Chennai.
- 96. 96 Dept of Urology, GRH and KMC, Chennai.
- 97. Classificationof CIS intoclinicaltypes: • Primary : isolated CIS with no previous or concurrent Papillary tumors or previous CIS • Secondary : CIS detected during follow-up of pts with a previous tumor that was not a CIS • Concurrent : CIS in the presence of any other urothelial tumors in the bladder 97 Dept of Urology, GRH and KMC, Chennai.
- 98. • Muscle invasive • Histology: • Invading urothelium shows irregular nests, single cell infiltration or tentacular finger-like projections • Stromal response -desmoplasia, -retraction or -inflammation. 98 Dept of Urology, GRH and KMC, Chennai.
- 99. 99 Dept of Urology, GRH and KMC, Chennai.
- 100. • Assess level of invasion for staging . • Presence and status of involvement of muscularis propria should be reported in TURBT specimen for adequate staging. 100 Dept of Urology, GRH and KMC, Chennai.
- 101. HISTOLOGICVARIANTS OF UROTHELIAL CARCINOMA • Nested pattern • Small tubular pattern • Microcytic pattern • Inverted pattern • With squamous differentiation • With glandular differentiation • Micro papillary • Sarcomatoid • Clear cell • With syncitiotrophoblasts • With unusual stromal reaction 101 Dept of Urology, GRH and KMC, Chennai.
- 102. NESTEDVARIANTOFUROTHELIALCARCINOMA • Rarebut aggressive cancer • male-to-female ratio of 6 : 1 • confused with benign lesions - von Brunn nests that are in the lamina propria, - cystitis cystica, -inverted papillomas. littlenuclear atypia in the nested variant of urothelial carcinoma 102 Dept of Urology, GRH and KMC, Chennai.
- 103. Nested variant • Tumor cells will often contain areas with large nuclei and mitotic figures 103 Dept of Urology, GRH and KMC, Chennai.
- 104. CLEAR CELLVARIANTOFUROTHELIAL CARCINOMA • 70% -will have foci of clear cells within the tumor. • glycogen-rich vacuoles and may be confused with metastatic clear cell carcinoma of the kidney. Clear cell variant does not a significantly worse prognosis for urothelial cancers 104 Dept of Urology, GRH and KMC, Chennai.
- 105. 105 Dept of Urology, GRH and KMC, Chennai.
- 106. GLANDULAROR ADENOCARCINOMA DIFFERENTIATION • Mixed tumor differentiation is m/c with squamous cell cancer, • only 6% of urothelial cancer cases. Diffi- two glandular spaces within the tumor • Mucin production can occur, and tumor cells seem to be floating in the mucin. 106 Dept of Urology, GRH and KMC, Chennai.
- 107. PLASMACYTOIDTUMOR Recognized by the WHO classification system since 2004 • Urothelial tumor cells look like plasma cells due to abundant eosinophilic cytoplasmhe ecentric nuclei & indistinct nucleoli. • Invade the bladder wall and perivesical adipose tissue & abdominal cavity at the time of diagnosis. 107 Dept of Urology, GRH and KMC, Chennai.
- 108. • diagnosed at an advanced stage, 64% T3 & 23% T4, 60% metastasis. • Positive stains: CK, CD138 • Negative stains: plasma cells & lymphocytes marker • Delation of 9p21, p53 mutation in 30% • Onset of hematuria is delayed – • sessile and non-papillary tumor growth pattern. 108 Dept of Urology, GRH and KMC, Chennai.
- 109. 109 Dept of Urology, GRH and KMC, Chennai.
- 110. MICROPAPILLARY • Incidence- 0.7-2.2% • M:F - 10:1 • occurs at older age – 65 yrs • Present at advanced stage, • Edematous stroma with chronic inflammatory infiltrate • Associated with conventional urothelial ca in 80% 110 Dept of Urology, GRH and KMC, Chennai.
- 111. • Histology- Small nests & papillae with surrounding retraction spaces, similar to papillary serous ca of ovary ( no psammoma bodies) • Angiolymphatic invasion is common • High progression from Non-muscle invasive -Muscle invasive - Metastatic 111 Dept of Urology, GRH and KMC, Chennai.
- 112. HP image:Micropapillary(U)& UsualUC(L) • Positive stains: CK7, CK20, variable HER2 & CA-125 DDx: papillary car. Of ovary papillary nephrogenic adenoma invasive UC with stromal retraction 112 Dept of Urology, GRH and KMC, Chennai.
- 113. NONUROTHELIAL MALIGNANCY •Sarcoma •Signet ring cell ca •Small cell ca •Sq cell ca •Prostatic urethral ca •adenocarcinoma 113 Dept of Urology, GRH and KMC, Chennai.
- 114. Squamouscell carcinoma • Risk factor for bladder SCC - Smoking - Stones/FBs - Schistosomiasis haematobium - Chronic UTIs - Chronic indwelling catheter 114 Dept of Urology, GRH and KMC, Chennai.
- 115. - BCG - Diverticula (bladder) - Trauma - prolonged cyclophosphamide- 115 Dept of Urology, GRH and KMC, Chennai.
- 116. 116 Dept of Urology, GRH and KMC, Chennai.
- 117. SquamousCell Carcinoma • Histological types: Usual type, • Verrucous, • Variant, • Basaloid with sarcomatoid features 117 Dept of Urology, GRH and KMC, Chennai.
- 118. Mechanism may be due to 1.Increased proliferation rate 2.Chronic inflammation and exposure to environmental agent – Generate: N-butyle N-Nitrosomaine Chronic infection converts nitrates – nitrites - nitrosamines 118 Dept of Urology, GRH and KMC, Chennai.
- 119. 119 Dept of Urology, GRH and KMC, Chennai.
- 120. • Large ulcerated, necrotic • 80% involved muscular wall at diagnosis • Squ. Metaplasia up to 60% 120 Dept of Urology, GRH and KMC, Chennai.
- 121. • LN metastasis- 10-27% • Metastasis to bone & lung • Positive stains: CK5/6( 77%) CK5/14 (96%) • Negative stains: CK-20 & Uroplakin III • Grading is not reproducible 121 Dept of Urology, GRH and KMC, Chennai.
- 122. Adenocarcinoma • Risk factors for adenocarcinoma of the bladder - Urachal cyst/remnant, - Cystitis glandularis, - CIS, - Chronic inflammation, - Ureterosigmoidostomy, - Bladder augmentation - Exstrophy of bladder. 122 Dept of Urology, GRH and KMC, Chennai.
- 123. ADENOCARCINOMA • <2% of primary bladder cancers • Majority represent Mets from GI tract, breast, lung , colon primary • Usually arise in trigoneor in dome (urachal) 123 Dept of Urology, GRH and KMC, Chennai.
- 124. • M/C – Exstrophy & associated with pelvic lipomatosis Develop in response - • chronic inflammation • irritation 124 Dept of Urology, GRH and KMC, Chennai.
- 125. 125 Dept of Urology, GRH and KMC, Chennai.
- 126. • Classifications of adenocarcinomas of the GU tract • 1) primary vesical • 2) urachal • 3) metastatic 126 Dept of Urology, GRH and KMC, Chennai.
- 127. • Most are poorly differentiated and invasive • More often associated with cystitis glandularis than CIS • Glandular components predominant, resemble colonic CA • Poor prognosis due to advanced stage at presentation. • Positive stains: CK7, CK20, CEA, EMA, Villin, membranous beta-catenin • Negative stains: vimetin, Uroplakin III, nuclear beta-catenin 127 Dept of Urology, GRH and KMC, Chennai.
- 128. URACHAL ADENOCARCINOMA • Located at the dome of the bladder • 90% of masses occur close to the bladder 128 Dept of Urology, GRH and KMC, Chennai.
- 129. • Midline, • infraumbilical, • soft-tissuemass with calcification ( Stippled ) consideredto be urachal adenocarcinoma until proved otherwise. 129 Dept of Urology, GRH and KMC, Chennai.
- 130. • Usually adenocarcinomas but can also be TCC, SCC, or even sarcomas • C/F- bloody or mucoid discharge from umbilicus • palpable mass after forming mucocele. 130 Dept of Urology, GRH and KMC, Chennai.
- 131. Urachaladenocarcinoma... • Staging is different than other UC • Sheldon staging system • Positive stains: CK7, CK20, CDX2 beta-catenin –ve • Mets to LN, lungs, Peritoneal cavity, liver & bone 131 Dept of Urology, GRH and KMC, Chennai.
- 132. • DDx: 1. local extension of colonic or other adenocarcinoma 2. Metastatic AC 3. Villous adenoma 4. Non urachal AC of bladder with mucinous or colloidal histology 132 Dept of Urology, GRH and KMC, Chennai.
- 133. 133 Dept of Urology, GRH and KMC, Chennai.
- 134. 134 Dept of Urology, GRH and KMC, Chennai.
- 135. Urachal adenocarcinoma.... 135 Dept of Urology, GRH and KMC, Chennai.
- 136. • Cystoscopy: Exophytic, • sessile mass • Grape like, • Papillary lesions • fulgrated area 136 Dept of Urology, GRH and KMC, Chennai.
- 137. T/t: clinically localised/feasibl case: • Partial cystectomy with en block resection of MUL & Umbilicus • RT, CT( 5-FU, Cisplatin) • Targeted therapies: sunitinib, Gafitinib Bevacizumab & cetuximab Advance cases: radical cystectomy • Poor prognosis, 5 yrs SR – 25-50% 137 Dept of Urology, GRH and KMC, Chennai.
- 138. 138 Dept of Urology, GRH and KMC, Chennai.
- 139. SIGNET CELL CARCINOMA: • 1/3 urachal origin and 2/3 directly extend into the bladder • Rare variant of adenocarcinoma • High-grade, high-stage tumors at presentation • Poor prognosis 139 Dept of Urology, GRH and KMC, Chennai.
- 140. • Carcinoembryonic antigen (CEA)- Elevated • The prognostic significance – unclear • Treatment is radical cystectomy • Survival < 20 months 140 Dept of Urology, GRH and KMC, Chennai.
- 141. 141 Dept of Urology, GRH and KMC, Chennai.
- 142. SMALLCELLCARCINOMA • < 1% all primary bladder tumors • Derived from neuroendocrinestem cells or dendritic cells • Stain +ve for Enolase • May be mixed with elements of TCC • Very aggressive with earlyvascular and muscle invasion 142 Dept of Urology, GRH and KMC, Chennai.
- 143. • Small cell carcinoma of lung or prostate- Metastasized to the bladder Small cell carcinoma of the bladder should be considered and treated as metastatic disease, even if there is no radiologic evidence of disease outside the bladder. Chemo-radiation 143 Dept of Urology, GRH and KMC, Chennai.
- 144. 144 Dept of Urology, GRH and KMC, Chennai.
- 145. SARCOMA • Leiomyosarcoma > rhabdomyosarcoma • M:F = 2:1, 6th decades of life , non- smoker • Rhabdomyosarcoma- MC in young children. • Produce polyploidy lesions at the base of the bladder, described as botryoides tumors 145 Dept of Urology, GRH and KMC, Chennai.
- 146. • Pelvic RT & CT (Cyclophosphamide) • Most of sarcomas are high grade • > 75% are confined to bladder muscle • Gross painless hematuria • local irritative symptoms 146 Dept of Urology, GRH and KMC, Chennai.
- 147. 147 Dept of Urology, GRH and KMC, Chennai.
- 148. CECT abdo:(a) heterogeneousenhancingtumorin thebladder (b) Delayed imaging showing siteof attachmentof tumorto the domeof bladder 148 Dept of Urology, GRH and KMC, Chennai.
- 149. Cystoscopicimages:(a) Tumor(T) seeninside the bladder (UB) (b) Narrowareaof attachmentof tumor to bladder 149 Dept of Urology, GRH and KMC, Chennai.
- 150. • Mean size- 7cm, • Invasive with ulcerative surface • necrosis in high grade • Myxoid subtype: like inflammatory myofibroblastic tumor 150 Dept of Urology, GRH and KMC, Chennai.
- 151. • IHC: positive stains- • Actin, • h-caldesmin, • desmin, • vemetin Negative stains – EMA, S100, CK5/6 151 Dept of Urology, GRH and KMC, Chennai.
- 152. • DDx: • 1. Sarcomatoid car. 2. Inflammatory myofibroblastic tumor • T/t: Radical cystectomy with wide margin • CT for Mets or CT+RT before SX • Poor prognosis 152 Dept of Urology, GRH and KMC, Chennai.
- 153. 153 Dept of Urology, GRH and KMC, Chennai.
- 154. Prostatic Urethral Carcinoma • Associatedwith urothelial Ca in 90% of cases • Isolatedcases only 3% • Risk factors : CIS of the bladder neck, h/o intravesicalCT • Pts undergoing radical cystectomy for UC – 40% • 154 Dept of Urology, GRH and KMC, Chennai.
- 155. • Route of spread- Direct or pagetoid • Diagnosis : Transurethral resection of prostatic urethra is primary method • Treatment : Non invasive- • Transurethral resection of prostatic urethra + BCG • Prostatic ductal ca- complete transurethral prostatectomy + BCG 155 Dept of Urology, GRH and KMC, Chennai.
- 156. 156 Dept of Urology, GRH and KMC, Chennai.
- 157. Pagetoid spread • Cancer cells grow undermining the normal surface urothelium • Primary seen in urothelial CIS • Can occur into the prostatic urethra & distal ureters 157 Dept of Urology, GRH and KMC, Chennai.
- 158. • M/C after repeated doses of intravesical therapies • Detection is very difficult, only 15% CIS & 11% NMIBC shows this type of growth • Biopsy should be considered 158 Dept of Urology, GRH and KMC, Chennai.
- 159. DIRECT EXTENSION • Direct extension of tumors into deeper structure & angiolymphatic system • caused by genetic & epigenetic changes • produce substance in ECM that invade these tissue -collagenases, motility & growth factors, cell adhesion molecules • Proepithelin – critical role as autocrine growth factor 159 Dept of Urology, GRH and KMC, Chennai.
- 160. Directextension • Others growth factors associated with UC invasion • EGFs , TGFa , HBGF, ILGF, • Cell adhesion molecules: maintain cell-cell junction & inhibition of cell growth - E-cadherin integrins , CD-44, NCD-44 160 Dept of Urology, GRH and KMC, Chennai.
- 161. 161 Dept of Urology, GRH and KMC, Chennai.
- 162. Prognosticfactors • Tumor size • Multiplicity • Papillary vs Sessile configuration • Absence/presence of Lymphovascular invasion 162 Dept of Urology, GRH and KMC, Chennai.
- 163. • Status of remaining urothelium • Cytogenetic profile • Stage & grade of tumor Tumor Grade: growth potential of primary tumor/progression Tumor stage: extent of the cancer & ability to invade/survival 163 Dept of Urology, GRH and KMC, Chennai.
- 164. • THANK YOU 164 Dept of Urology, GRH and KMC, Chennai.