Malaria in Bangladesh
•Transferir como PPTX, PDF•
10 gostaram•9,362 visualizações

previous and current situation of malaria in BD, treatment, prevention, national malaria strategic plan 2915 etc.

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Semelhante a Malaria in Bangladesh
Semelhante a Malaria in Bangladesh (20)
Mais de Oyshe Ahmed
Último
Último (20)
Malaria in Bangladesh
- 2. 1. Suraiya Ahmed 2. Atikur Rahman Nyeem 3. Mimma Sultana Chandni 4. Reeti Susan Roy 5. Faria Iqbal 6. Sabrina Arafin Tanni Presented By-
- 3. Malaria is a mosquito-borne infectious disease of humans and other animals caused by parasitic protozoans (a group of single- celled microorganism) belonging to the genus Plasmodium. The female Anopheles mosquito is the only mosquito that transmits malaria. It primarily bites between the hours of 9pm and 5am What is MALARIA?
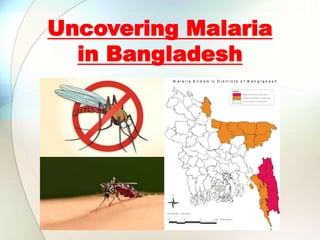
- 4. • Malaria is one of the major public health problems in Bangladesh. • It is endemic in 13 eastern and northern districts of the country. • The three hilly districts (Rangamati, Khagrachari and Banderban) account for 80% of the total burden of malaria. • During the last decade, 82% of the total annual reported cases were due to Plasmodium falciparum. • The remaining cases are due to Plasmodium vivax, and few are due to mixed infection. • Over 13.25 million people of Bangladesh are at high risk of malaria, with the utmost vulnerability of the under-five children and pregnant women. • Malaria claims about 0.10% lives annually. • In 2012, the official number of laboratory confirmed malaria cases in the country was 29,522 with 11 confirmed malaria deaths. INTRODUCTION & BACKGROUND
- 6. • Malaria is caused by the plasmodium parasite. The parasite can be spread to humans through the bites of infected mosquitoes. There are many different types of plasmodium parasite, but only five types cause malaria in humans. They are: 1. Plasmodium falciparum (the most common type of malaria parasite and is responsible for most malaria deaths worldwide) 2. Plasmodium vivax 3. Plasmodium ovale 4. Plasmodium malariae 5. Plasmodium knowlesi CAUSES OF MALARIA
- 7. • Malaria can cause a number of life-threatening complications that can result in death. The following may occur: swelling of the blood vessels of the brain (cerebral malaria) accumulation of fluid in the lungs that causes breathing problems (pulmonary edema) organ failure (kidneys, liver, or spleen) anemia due to destruction of red blood cells low blood sugar Life-Threatening Complications of Malaria
- 8. The plasmodium parasite is spread by female Anopheles mosquitoes, which are known as 'night-biting' mosquitoes because they most commonly bite between dusk and dawn. If a mosquito bites a person already infected with malaria, it can also become infected and spread the parasite on to other people. However, malaria cannot be spread directly from person to person. Once a person is bitten, the parasite enters the bloodstream and travels to the liver. The infection develops in the liver before re- entering the bloodstream and invading the red blood cells. The parasites grow and multiply in the red blood cells. At regular intervals, the infected blood cells burst, releasing more parasites into the blood. Infected blood cells usually burst every 48-72 hours. Each time they burst, patient will have a bout of fever, chills and sweating. Malaria can also be spread through blood transfusion and the sharing of needles, but this is very rare. How Malaria Spreads?
- 10. Shaking chills that are moderate to severe High fever Profuse sweating Headache Nausea Vomiting Diarrhea Anemia Muscle pain Convulsions Coma Bloody stools etc. Symptoms of Malaria
- 11. Four districts (Mymensingh, Netrakona, Sherpur and Kurigram) with eight endemic upazilas have low transmission of malaria and have shown <5% malaria positivity rates (RDT and Microscopy) over last three years. These districts currently may be considered for adopting pre-elimination strategies. There is significant progress in malaria control in Bangladesh during the period from 2008 to 2013 showing a progressive decline in total cases and deaths. Current Malaria Situation in Bangladesh
- 12. The NMCP had the GFATM support since 2007 and there was an increase in number of cases due to scaling up of interventions; introduction of RDR for diagnosis, and ACT for treatment of P. falciparum cases. Thereafter, a steady decline is noted from 84,690 cases in 2008 to 26,891 cases in 2013, having a 68.2% reduction in case incidence. The total deaths came down to 15 in 2013 as against 154 in 2008 showing 90.2 % reduction.
- 13. • The table below shows District-wise epidemiological data of the 13 endemic districts for three consecutive years for a comparison based on total cases, Pf %, and Annual Parasite Incidence (API). The five districts (3 CHT districts and Chittagong and Cox’s Bazar) had reported API 7.36, 4.02 and 3.77 respectively in 2011, 2012 and 2013. Stratification of Malaria Endemic Districts
- 14. • The total population at risk of malaria in the 13 endemic districts is approximately 13.25 million. (Ref: NMCP Routine Surveillance data) and the List is attached as Annex-1. About 80% of the cases of malaria in Bangladesh are reported from the three CHT districts with a total population of about 1.6 million. The indigenous population constitutes about 50% of the total population in CHT districts. • There is a high degree of heterogeneity in malaria cases distribution between the sexes and across age groups in Bangladesh. During the 2008-2013 periods, males consistently show more positive diagnoses than females and with increasing trends over the years(Figure 4).Pregnant women constitute 1% of malaria cases in recent years. Population at Risk Fig: Age Distribution of malaria cases
- 15. • Malaria affects all age groups and both males and females; however, adult males are commonly affected mainly due to occupations and behavior that put them at risk of being bitten by malaria vectors. Pregnant women and children <5yrs are biologically at higher risk and they tend to develop more severe malaria due to low level of immunity. Thus, in high transmission areas, these groups should be given priority for interventions. High risk populations, thus includes: i) Young children, particularly under <5 yr children, ii) Pregnant women, iii) Travelers from non-endemic areas, iv) People from non-endemic areas residing for a long time and returning home, v) ‘Jhum cultivators’ and forest goers, Tea estates; vi) Refugees and mobile population, and vi) People with HIV/AIDS and TB (for co-infections, if any).
- 16. Historically, the malaria control programme in Bangladesh had four phases: 1. Malaria Eradication Programme (in early 1960s; 2. Malaria Control Programme (1977-1994); 3. Revised Malaria Control Strategies (RMCS-1994); and 4. Continuation of RMCS with updated strategies until today. Malaria control program
- 17. Malaria is usually confirmed by- • the microscopic examination of blood films or • by antigen-based rapid diagnostic tests (RDT). • RDT started to use in a mass scale from 2008 under the support of GFATM funding under round 6. At the community level ‘ShayasthoKarmi’ (health worker) and ‘Shayastho Shebika’ (community volunteer) of NGOs are responsible for diagnosis and treatment of uncomplicated malaria. The GoB Health Workers are also responsible for diagnosis and treatment of uncomplicated malaria using Pan RDT. Diagnosis and Management of Malaria The blood film is the gold standard for malaria diagnosis
- 18. Pan RDT
- 19. An insecticide-treated net (ITN) is a net (usually a bed net), designed to block mosquitoes physically, that has been treated with safe, residual insecticide for the purpose of killing and repelling mosquitoes, which carry malaria. A long-lasting insecticide-treated net (LLIN) is an ITN designed to remain effective for multiple years without retreatment. The insecticide is cleverly bound within the fibers that make up the netting and is 'slow released' over a 4-5 year period. LLIN and ITN Coverage for Malaria Prevention
- 20. • HEED Bangladesh signed in agreement with GFATM one of the principle recipients BRAC in May, 2008 to implement Malaria Control Project in Jaintapur Upazila in Sylhet district with a view to contribute in reducing malaria burden nationally by June, 2015. Use of LLIN and ITNs
- 21. • Bioassay test conducted in various sites as a routine entomological surveillance. The results of the bio-assay test on LLINs and ITNs dipped with K-O-Tab1,2,3 mortality rates of mosquito nets at Durgapur, Jheenaigati, Kolmakanda, Lama, Rangamati Sadar and Jointapur upazila. Bio Assay Test
- 22. • Antimalarial medications, also known as antimalarials, are designed to prevent or cure malaria • In the South Asian region, Plasmodium vivax and Plasmodium falciparum are the predominant species causing human malaria. For the last decade, chloroquine-resistant P. falciparum has spread explosively in sub-Saharan Africa, Southeast Asia, and South Asia • Control of falciparum malaria is becoming a challenge especially in Multi-Drug Resistant (MDR) areas. • P. falciparum is also responsible for complications like cerebral malaria etc, prompting more than one million deaths per year. • The other species of mosquito responsible for malaria (P. vivax, P. ovale and P. malariae) also produce high morbidity but are usually susceptible to chloroquine, which is a good blood schizontodicidal drug. Antimalarial medication
- 23. • In Bangladesh, 60% of the malaria cases are P. falciparum. Malaria is also a health problem in the southern belt of 30–50 km and a few valleys in Bhutan, where 50% of the cases are P. falciparum.
- 24. Resistance has been documented in all class of antimalarials, including artemisinin derivatives and it is a major threat to malaria control. Wide spread and indiscriminate use of antimalarials exerts a strong selective pressure on malaria parasites to develop high levels of resistance. Resistance can be prevented by ensuring very high cure rate through full adherence of correct dose regimen. Chloroquine and Salfadoxine/Pyrimethamine both are resistant. So these drugs should not be used in malaria cases. Mefloquine, a highly efficacious drug for P. falciparum but it is not recommended to use as a single drug. Artesunate for uncomplicated malaria is highly effective for P. faciparum but single drug use is not recommended due to chance of development of resistance. Artesunate, Melfoquine combination is highly effective in P. falciparum cases (Alternate regime) Drug resistant malaria
- 25. • Resistant strains are able to efflux the drug by an active pump mechanism. • pfcrt gene encodes a transporter in the membrane of acidic digestive vacuole causing efflux of chloroquine from the food vacuole • :K76T Mutation • There is an increase in the surface area of the resistant parasites, permitting more efficient pinocytosis. Mechanism Of Resistance
- 27. • Pharmacotherapy of uncomplicated P.Falciparum Chloroquine resistant malaria with Artemisinine Combination Therapy. WHY ACT FOR CHLOROQUINE RESISTANT MALARIA? • The Artemisinins produce rapid clearance of parasitaemia and rapid resolution of symptoms • High cure rates (>95%) • Combination therapy prevents resistance. • Shorter T ½ so only problem is Recrudescence. The partner medicine have different mechanisms of action , longer half-lives and must independently be sufficiently efficacious in treating malaria.
- 28. • WHO Recommends following Artemisinin based combination regimes for the management of Chloroquine resistant P.Falciparum malaria. 1. Artesunate-sulfadoxine + Pyrimethamine(AS-S/P) 2.Artemether-Lumefantrine(AS/LF) 3.Artesunate/Mefloquine(AS/MQ) 4. Artesunate-Amodiaquine(AS/AQ) 5. Dihydroartemisinin(DHA)-Piperaquine ARTEMISININ COMBINATION THERAPY (ACT)
- 31. Elimination of mosquito breeding places National improvements on health and hygiene Use of mosquito nets, treated with Pyrithrin Clothing with sleeves and long trousers Use of mosquito repellents Young children and pregnant women should avoid traveling to areas where malaria is common PREVENTION & CONTROL
- 33. The types of drugs and the length of treatment will vary, depending on: Type of malaria parasite Severity of the symptoms Age Pregnancy Medications oThe most common antimalarial drugs include: oChloroquine (Aralen) oQuinine sulfate (Qualaquin) oHydroxychloroquine (Plaquenil) oMefloquine o Doxycycline (available generically) oCombination of atovaquone and proguanil (Malarone) TREATMENT (VACCINE & MEDICATIONS)
- 34. Malaria vaccines are an area of intensive research. Emergence of artemisinin and multi-drug resistant strains of especially P. falciparum are driving research. Current approaches are focusing on recombinant protein and attenuated whole organism vaccines. Various vaccines have reached the state of clinical trials; most demonstrated insufficient immunogenicity. The malaria vaccine candidate RTS,S/AS01. RTS,S/AS01 is the most advanced vaccine candidate against the most deadly form of human malaria, Plasmodium falciparum. VACCINE
- 35. • Tu Youyou (1930) is a Chinese medical scientist and pharmacist. She is best known for discovering artemisinin (also known as qinghaosu) and dihydroartemisinin, used to treat malaria, which saved millions of lives. Tu received the 2015 Nobel Prize in Medicine for discovering this. • She collected 2000 candidate recipes, ancient texts, and folk remedies for possible leads for her research. By 1971, her team had made 380 extracts from 200 herbs, and discovered the extracts from qinghao (Artemisia annua, sweet wormwood) looked particularly promising in dramatically inhibiting Plasmodium growth in animals. Recent Research
- 36. • Existing Strategic Plan (2008-14) The existing National Strategic Plan 2008-2015 envisaged 60% reduction of malaria morbidity and mortality (compared to baseline 2005) by 2015 with the specific objectives of: i) providing early diagnosis and prompt treatment (EDPT) with effective drugs to 90% of malaria patients; ii) ensuring effective malaria prevention to 100% population at risk in five high endemic districts and 80% in the remaining eight districts; iii) providing pre-referral treatment and timely referral of 90% of severe malaria cases; iv) promoting community participation, partnership with NGOs and private sector and v) strengthening management capacity, M&E and Procurement and Supply Management (PSM) systems in the National Malaria Control Programme. National Malaria Strategic Plan 2015-2020
- 37. • The Malaria Strategic Plan (2015- 2020) provides the framework and technical guidance for the National Malaria Control Programme (NMCP) to plan and implement interventions for achieving pre-determined goals, objectives and targets. The goal is ‘To have achieved ‘zero indigenous transmission’ and ‘zero death’ aiming malaria elimination in Bangladesh, by 2020. Malaria Strategic Plan (2015-2020)
- 38. Vision: Malaria-free Bangladesh Mission: The National Malaria Control Programme (NMCP), Bangladesh aims to achieve malaria elimination (‘zero indigenous transmission’ and ‘zero deaths’) by ensuring equitable and universal accesses to effective preventive and curative services to all ‘at risk population’ through concerted efforts of the GoB, NGOs, Private sectors, and the community. Goal: By 2020, to have achieved ‘zero indigenous transmission’ and ‘zero death’ aiming malaria elimination in Bangladesh The goal aims at attaining a status of malaria elimination by 2020, referring to reorientation of the control interventions in phased and stratified manner for: i) addressing four low endemic districts (Kurigram, Sherpur, Mymensingh and Netrakona); ii) expansion to the moderate endemic districts; and iii) intensified efforts in high endemic districts; for achieving eventual malaria elimination status in Bangladesh.
- 39. Conclusion Malaria remains a major public health problem in the tropic. Prompt diagnosis is essential for timely initiation of appropriate therapy. Multi-drug resistant malaria is a public health threat. Chloroquine drug resistant is high so it should not be used in malaria. ACT (Artemisinin combination therapy) should be used. In cerebral malaria i/v Artisunate is preferable than i/v Quinine when available. Preventive measures is one of the major aspects to strengthen malaria control programme.