LVOT OBSTRUCTION IN ICU
•Transferir como PPTX, PDF•
3 gostaram•234 visualizações

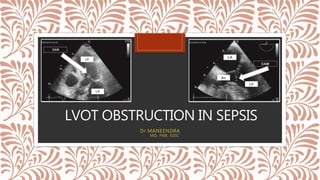
LEFT VENTRICULAR OUTFLOW TRACT OBSTRUCTION IN SEPSIS

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (18)
Semelhante a LVOT OBSTRUCTION IN ICU
Semelhante a LVOT OBSTRUCTION IN ICU (20)
Último
Último (20)
LVOT OBSTRUCTION IN ICU
- 1. LVOT OBSTRUCTION IN SEPSIS Dr MANEENDRA MD, FNB, EDIC
- 2. CASE VIGNETTE • 60 yr/f • DM / HTN / CAD / LVH • Fever 3 days • Burning micturition 2 days, IN ER : • HR : 130 • BP : 80 / 40 • TEMP : 102F • Conscious , oriented • SPO2 : 98% ON RA FLUID RESUSCITATION – 30 ml/kg VASOPRESSORS desaturates and develops crepts WORSENING HYPOTENSION LVOTO
- 3. HCM AND LVOTO Apical hypertrophy Symmetrical hypertrophy Asymmetrical septal hypertrophy without obstruction Asymmetrical septal hypertrophy with obstruction Inc LV wall thickness at least 15 mm in one/ more LV myocardial segments instantaneous peak Doppler LVOT pressure gradient at least 30 mmHg at rest or during physiological provocation
- 4. PATHOPHYSIOLOGY HCM, hypertension aortic stenosis mitral valve replacement or repair steep aortic root angle acute cor pulmonale ballooning syndrome (Takotsubo) sigmoid septum Needs two factors : • Anatomical substrate and • Physiological predisposing conditions
- 5. PATHOPHYSIOLOGY Decrease preload Decrease afterload Increase heart rate Increase contractility Small and hypercontractile LV Needs two factors : • Anatomical substrate • Physiological predisposing conditions
- 6. Stress cardiomyopathy – takatsubocardiomyopathy hypercontractile LV base mid and distal akinesia reduction in LV chamber size bleeding, diuretics, trauma, or inotrope infusion crowding at the LV outflow level results in systolic anterior motion of the mitral apparatus dynamic obstruction Hypotension new prominent systolic ejection murmur in the left third parasternal area
- 7. DIAGNOSIS • new systolic murmur in the left low sternal border that increases with Valsalva maneuver or postextrasystole • Definitive diagnosis requires performing an echocardiogram as soon as possible
- 8. TREATMENT Increase preload Increase afterload Decrease heart rate Decrease contractility Stop Diuretics Vasopressors Ionotropic agents Nitrates Start IV fluids B blockers Ca chnl blockers Disopyramide
- 11. IMPORTANCE IVO occurrence in septic shock patients; correlation between the intraventricular gradient and volume status and fluid responsiveness; mortality rate. prospectively analyzed 218 patients ,septic shock admitted to a general ICU over a 28-month
- 12. CASE VIGNETTE • 60 yr/f • DM / HTN / CAD / LVH • Fever 3 days • Burning micturition 2 days, IN ER : • HR : 130 • BP : 80 / 40 • TEMP : 102F • Conscious , oriented • SPO2 : 98% ON RA FLUID RESUSCITATION – 30 ml/kg VASOPRESSORS desaturates and develops crepts WORSENING HYPOTENSION LVOTO
- 13. Take home message • Identify existence of a phenomena of LVOT obstruction in ICU • Learn to measure LVOT pressure gradient using doppler • Early adequate fluid resuscitation of all sepsis patients • Use of B blockers once hemodynamics are controlled with vasopressors to reduce the heart rate • Plan a observational study of measuring LVOT pressure gradient in all septic shock patients and see how it progresses with treatment and how it influences mortality
- 14. EYES WILL SEE ONLY WHAT THE MIND KNOWS……. THANK YOU……