
Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Bladder and injuries
Semelhante a Bladder and injuries (20)
Último
Último (20)
Bladder and injuries
- 2. Location & relations • Located in the ant pelvis • Rests on anterior part of pelvic floor, behind the symphysis pubis and below the peritoneum
- 3. Bladder anatomy Size & shape varies with amount of urine Hollow muscular organ, urine reservoir
- 4. PARTS OF BLADDER Body with a fundus or base Bladder neck Apex A superior surface Two inferolateral sufaces
- 5. Superior surface Related to Peritoneum of utero-vesical pouch, uterus and bowel
- 6. Base of the bladder Related with the supravaginal cervix & the anterior fornix.
- 7. Inferolateral surface Related with the space of Retzius.
- 8. Bladder neck Rests on superior layer of the urogenital diaphragm
- 9. Bladder bed
- 10. Angles of the Bladder • Apex - continuous with • 2 Lateral angles where the obliterated urachus the ureters enter the bladder • Neck - most inferior part, related to the superior pelvic fascia
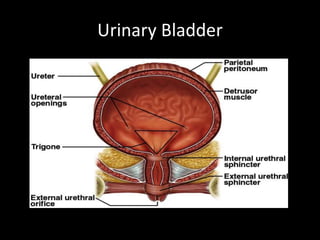
- 11. Trigone of the Bladder Triangular area marked by three openings Two ureteral orifices Urethral opening
- 12. Bladder trigone cervix uterus
- 13. Female Urethra • 3 to 4 cm long • External urethral orifice – between vaginal orifice and clitoris • Internal urethral sphincter – detrussor muscle, thickened smooth muscle, involuntary control • External urethral sphincter – skeletal muscle, voluntary control
- 15. Blood Supply Vesical arteries Superior VA Arises from the proximal part of ant div of Int I A Divides into numerous br & supply dome of bladder Middle VA Br of SVA Supplies the base of bladder Inferior VA Arises from middle rectal or vaginal artery Base & the Trigone
- 16. Venous drainage of bladder Vesical venous plexus Internal Iliac veins Internal vertebral venous plexus
- 17. Lymphatic supply • Superior part - external iliac lymph nodes • Inferior part - internal iliac lymph nodes • Bladder neck - sacral or common iliac lymph nodes
- 18. Micturition Results from a complex interplay of sympathetic , parasympathetis & higher centre
- 19. Micturition reflex Filling of urinary bladder → stretch receptors → sensory impulse via pelvic nerve to S2 – S4 → Parasympathetic impulse via pelvic nerve → Contraction of detrusor muscle & relaxation of internal sphincter → urine in urethra stimulates stretch receptors → sensory impulse via pelvic nerve to S2 – S4 → inhibition of somatic fibers in pudendal nerve → relaxation of external sphincter → results in urination
- 20. Micturition reflex Sympathetic (through hypogastric nerve) stimulation of beta receptors on detrusor muscle causes relaxation & of alpha receptors on internal sphincter causes constriction of sphincter, hence sympathetic stimulation causes filling & referred to as nerve of filling.
- 21. Higher brain centers of Micturition • Facilitatory & inhibitory centers in brain stem especially pons • Centers located in cerebral cortex is normally inhibitory but can become excitatory • For voluntary urination, cortical centers can facilitate the sacral micturition centers to help initiate a micturition reflex & at the same time inhibit the external urinary sphincter.
- 22. Voluntary Control of Micturition • Micturition center in pons receives stretch signals and integrates cortical input (voluntary control) • Sends signal for stimulation of detrussor and relaxes internal urethral sphincter • To delay urination impulses sent through pudendal nerve to external urethral sphincter keep it contracted until you wish to urinate • Valsalva maneuver – aids in expulsion of urine by pressure on bladder – can also activate micturition reflex voluntarily
- 23. BLADDER INJURIES Risk factors Distorted pelvic anatomy Previous Cesarean sections Previous gynecologic surgeries Extensive pelvic adhesion ( Severe endometriosis, PID etc) Large myomas Pelvic malignancies Extensive surgical dissection (e.g, RH, Retropubic procedure)
- 24. BLADDER INJURIESINJURY BLADDER More frequent than Ureteral Injuries Rate - 1-1.8%
- 25. Mechanism of Bladder injury Perforation of bladder dome during Veress needle/trocar insertion Incidental cystotomy during development of bladder flap & VVS in routine/radical Hysterectomy Adhesiolysis or dissection with endoscopic scissors with or without electrosurgery
- 26. Bladder injury in a case with previous C-section
- 27. Bladder injury during TLH for Big fibroid (20 weeks)
- 28. Diagnosis of bladder injuries Unlike ureteral injuries, almost all the bladder injuries are diagnosed intra-operatively
- 29. Signs of intra-operative bladder injuries • Visualization of the Foley catheter bulb • Distention of urine collection bag with CO2 (Pneumaturia) • Urine drainage from accessory trocar site • Intraperitoneal leakage of Methylene Blue • Haematuria • Suprapubic bruising • Abdominal wall or pelvic mass • Cystoscopy – size & location
- 30. Intraoperative bladder injury identification by Methylene blue test
- 31. Post-operative identification of Bladder injury Bladder injury is suspected in the presence of: • Haematuria • Leakage of urine per vagina ( fistula) • Fever, flank pain, ileus, abdominal distension • Sepsis
- 32. Post-operative Diagnosis Cystoscopy POST-OPERATIVE VVF Cystogram Pad test IVP Diagnostic laparoscopy Cystogram showing VVF
- 33. Sequelae of Undiagnosed Injuries • Voiding dysfunction • Detrusor instability • Bladder stone formation with recurrent UTI • Uro-genital fistula formation • Renal damage
- 34. Management Intra-operative bladder injury Depends on : Size & location • Small cystotomy (<10 mm) - Closure followed by drainage for 5-7 days • Larger injuries - Laparoscopic or open repair
- 35. Laparoscopic Bladder injury repair Cystoscopy - Exclude injury to trigone - Check proximity of the defect to the ureter Remove necrotic tissue, adhesions or areas of endometriosis before actual repair
- 36. Laparoscopic repair of small intraoperative bladder injury
- 37. Laparoscopic Bladder suturing • Interrupted or continuous absorbable sutures through full thickness of bladder wall • Polyglactin or Polydioxanone , no 3-0 • Single layer closure is sufficient • Repair should include mucosa, muscularis & serosa • Peritoneal imbrication or omental graft placement between suture lines may decrease risk of fistula formation
- 38. Post-operative Period Bladder drainage with large caliber urethral or suprapubic catheter 5-7 days - simple fundal laceration 14 days - closer to trigone or vaginal vault - significant thermal damage Retrograde cystogram to confirm healing
- 39. Vesico-vaginal fistula • Delayed bladder injury presents as a VVF • Abnormal connection b/w bladder and vagina • Seen in first 7-10 days post operatively
- 40. Incidence 0.3-2% Abdominal hysterectomy- 83% Vaginal-8% Urological surgeries- 6.9% Radiation-4% Obstetric- 6.5%
- 41. Demographic variation Obstetric injuries are most common cause of VVF in developing countries whereas in developed countries, gynecological surgical injuries are the commonest cause of VVF.
- 42. What causes fistula ? • Direct trauma • Tissue devacularisation during dissection • Inadvertent suture placement • Infection- > tissue necrosis • Overdistention of bladder post operatively
- 43. Risk factors • Previous surgery • h/o sepsis • Endometriosis • Malignancy • Adhesions with bladder and uterus or cervix • Anatomical distortion within pelvis • Radiation
- 44. Clinical features Depend on site and size of fistula • Vaginal leakage • Recurrent cystitis • Pyelonephritis • Unexplained pyrexia • Hematuria • Pain: flank, vaginal or supra pubic • Abnormal urinary stream • Irritation of vagina and perineum • Foul odour
- 45. Type of fistula Simple - Tissue healthy, good vaginal access Complicated – large (> 5cms) scarring Impaired access Involvement of ureteric orifices
- 46. classification of urogenital fistulas • Urethral • Bladder neck • Sub symphysial • Midvaginal • Juxtacervical/vault • Vesicouterine • Vesicocervical
- 47. Presentation • Continuous urinary incontinence • Limited sensation of bladder fullness • Infrequent voiding
- 48. Timings of presentation 5-14 days post-operatively
- 49. Investigations • Dye test • Cysto urethroscopy • IVP • Retrograde pyelogram • Vaginal fluid collection to see conc. of urea • Urine analysis and culture
- 50. Basic principles for fistulae repair • Ensure that there is no cellulitis, edema, or infection at the fistula site prior to closing the fistula • Excision of avascular scar tissue • Wide mobilisation of bladder • Tension free layer closure of bladder and vagina • Good hemostasis with bladder drainage • Using transplanted blood supply
- 51. Techniques of repair • Conservative • Abdominal approach • Vaginal approach • Laparoscopic • Combined • Electrocautery • Fibrin glue • Using interposition flaps or grafts
- 52. Various approaches Vaginal Flap splitting Latzko’s procedure Abdominal O’conor technique Modified O’Conor Laparoscopic transperitoneal repair
- 53. Vaginal vs abdominal approach Vaginal Abdominal • In simple fistula • Inadequate vaginal exposure • When easy access to • For complicated fistula anterior vaginal wall • Recurrent fistula e.g, trigonal fistula • Failure of vaginal repair • Less morbiditiy • Multiple fistula • Shorter operative time • Larger fistula • Minimal blood loss • Associated pelvic pathology • Quicker recovery • In close proximity to ureter
- 54. Timings of repair • If diagnosed within 48 hrs post operatively – immediate repair Early repair 1-3 months Late repair 2-4 months
- 55. Pre operative care • Urinary or vaginal infection- treated • Early attempts to divert urinary stream • Catheter drainage( spontaneous healing in 7 %) • Care for perineal skin
- 56. Flap splitting technique • Adequate exposure made. • Fistula tract excised with a scalpel • The entire tract is dissected • The layers of the bladder wall and vagina adequately delineated and mobilized • The bladder mucosa closed with interrupted 4-0 synthetic absorbable suture • A second layer, the bladder muscle, is closed with 2-0 synthetic absorbable suture.
- 59. Flap splitting technique • Vaginal incision closed separately • The bulbocavernosus muscle transplant ± • The bladder filled with 200 mL of methylene blue to ascertain fistula closure. • Catheter for 3 wks
- 60. Latzko’s repair Prerequisites - Adequate preoperative vaginal vault length - Fistula located at vaginal apex Success rate - 89% at first attempt
- 61. Latzko’s repair • Obliterates upper vagina for 2-3 cm around the fistula ( partial colpocleisis) • An elliptical portion of vaginal epithelium is stripped in all directions around fistula tract • Pubovesical fascia closed in two layers • Vaginal epithelium closed in interrupted sutures • Posterior vaginal wall becomes the posterior bladder wall
- 62. Latzko’s repair
- 63. Abdominal repair Operative technique • Cystoscopy • Ureteral stenting • Vesicovaginal fistula catheterisation • Transperitoneal laparoscopic approach
- 66. Post operative care • Supra pubic drain for distal fistula • Urethral catheterization • Adequate hydration
- 67. Interposition grafting • Brings in new blood supply to the area • Supports fistula repair site • Creates additional layer • Fill the dead space
- 68. Tissues used.. • Martius graft- ( bulbocavernous muscle used) • Gracilis muscle • Omental pedicle graft • Peritoneal flap graft (paravesical area)
- 69. Complications of Fistula Repair • Post Operative Failure • Recurrent Fistula Formation • Injury to Ureter, Bowel, or Intestines • Vaginal Shortening
- 70. Prevention of bladder injuries • Routine drainage of bladder prior to trocar insertion • Identify the boundaries of the bladder (fill with 200-300 ml NS) • Meticulous & careful sharp dissection in the presence of • adhesion, endometriosis or previous LSCS • Be careful with the use of cautery & while suturing the vault • Be intrafascial in approach CYSTOSCOPY at the end
- 71. Thank You
Notas do Editor
- In O’Connors technique, bladder is bi-valved but in modified approach, bi-valving is avoided and and repair is done by making a small incision on the posterior aspect to reachupto the fistula.