Diphtheria
•
9 gostaram•7,908 visualizações

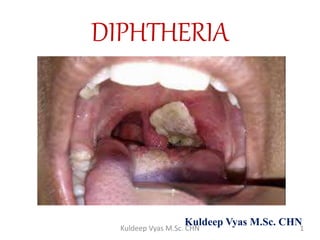
Acute infectious disease caused by toxigenic strains of Coryne bacterium diphtheriae.

Recomendados
Mais conteúdo relacionado
Mais procurados
Semelhante a Diphtheria
Semelhante a Diphtheria (20)
Mais de KULDEEP VYAS
Mais de KULDEEP VYAS (20)
Último
Último (20)
Diphtheria
- 1. KuldeepVyas M.Sc. CHN DIPHTHERIA Kuldeep Vyas M.Sc. CHN 1Kuldeep Vyas M.Sc. CHN
- 2. INTRODUCTION Acute infectious diseasecaused by toxigenic strains of Coryne bacteriumdiphtheriae. 3 major clinicaltypes-anterior nasal, faucial, laryngeal Skin, conjunctiva, vulvaand other parts may beaffected. Bacilli multiply locally inthroat and produce powerfulexotoxin. 2Kuldeep Vyas M.Sc. CHN
- 3. HISTORY Took its name from greek word “diphthera”meaning leather. Named in 1826 by French physician PierreBretonneau. In the past, disease was called as general disease or killerdisease because therewas no treatmentand was the cause of high mortality inchildren. Itwas said that thedisease killed as manyas 80% of the children below 10yrs. 3Kuldeep Vyas M.Sc. CHN
- 5. WORLD Developed countries rare disease dueto routine child vaccination Developing countries endemic due to lackof adequate widespread immunization Reported cases in 2010- 4187 Epidemics are largely due to decreasing immunization coverage among infants and children, waning immunity to diphtheria in adults, movements of large groups of populations in the last few years and irregular supplyof vaccines. 5Kuldeep Vyas M.Sc. CHN
- 6. INDIA Endemic disease Declining trend of diphtheria due toincreasing coverage of child population by immunization. Reported cases 1987- 12952 2011- 4286 112 deathsshowing acase fatality rateof about 2.61 6Kuldeep Vyas M.Sc. CHN
- 7. AGENT Agent Corynebacterium diphtheria Gram positive motileorganism No invasivepower but producepowerful exotoxinafter multiplication locally in the throat responsible for: 1. Formation of false membrane over tonsils, pharynx or larynx, with well defined edgesand membranecannot bewiped away. 2. Marked congestion, edema, local tissuedestruction 3. Enlargement of lymph nodes 4. Toxaemic signs andsymptoms 7Kuldeep Vyas M.Sc. CHN
- 8. 4 types -Gravis Mitis Belfanti Intermedius Sensitive topenicillinand readily killed by heatand chemical agents Affects heart- myocarditis nerves- paralysis Gravis more severe than mitis infection 8Kuldeep Vyas M.Sc. CHN
- 9. SOURCE OF INFECTION Cases- ranges from sub clinical toclinical mild orsilent infections mayexhibit not more than a mere running noseorsore throat Carriers- common source of infection may be temperoryorchronic;nasal or throatcarriers Nasal- dangerous( frequent shedding into environment) Temperory- lasts for 1 month Chronic- last for 1 yearuntil thepatient is treated 9Kuldeep Vyas M.Sc. CHN
- 10. INFECTIVE MATERIAL Naso-pharyngeal secretions Discharge from skinlesions Contaminated fomites Infected dusts 10Kuldeep Vyas M.Sc. CHN
- 11. PERIOD OF INFECTIVITY 14 – 28 days from theonsetof disease butcarriers may remain infective for much longerperiods. A case or carrier may be considered non- communicablewhen atleast 2 culturesobtained from nose or throat, 24 hours apart are negative for diphtheria bacilli. 11Kuldeep Vyas M.Sc. CHN
- 12. AGE Children upto 1-5 yrs HOST FACTORS SEX both IMMUNITY Infants borne of immune mothers are immune for first fewweeks or monthsof life. 12Kuldeep Vyas M.Sc. CHN
- 13. ENVIRONMENTAL FACTORS Cases occur in allseasons. Winter- favourable Kolkata- highest incidence inaugust Mumbai- wintermonths Delhi- august oroctober 13Kuldeep Vyas M.Sc. CHN
- 14. MODE OF TRANSMISSION Droplet infections Can also be transmitted directly tosusceptiblepersons from infected cutaneouslesions. Transmission by objects contaminated by naso- pharyngeal secretionsof patients isalso possible. 14Kuldeep Vyas M.Sc. CHN
- 15. PORTAL OF ENTRY Respiratory route- respiratory tract Non-respiratory route- Portal of entry may be skin wherecuts, ulcersand wounds not properly attended to or through umbilicus of new born. Siteof implantation may be eyes, genitalia or middleear. 15Kuldeep Vyas M.Sc. CHN
- 16. INCUBATION PERIOD 2- 6 days, ocassionallylonger. 16Kuldeep Vyas M.Sc. CHN
- 17. CLINICAL FEATURES Respiratory tract forms ofdiphtheria- pharyngo-tonsillar laryngo tracheal nasal combinations 17Kuldeep Vyas M.Sc. CHN
- 18. Pharyngo-tonsillar diphtheria • Sore throat • Difficulty inswallowing • Low grade fever atpresentation • Presence of pseudomembrane over tonsils • Oedema in submandibular region • Bull necked appearance 18Kuldeep Vyas M.Sc. CHN
- 19. 19Kuldeep Vyas M.Sc. CHN
- 20. Laryngo-tracheal diphtheria • Preceeded by pharyngotonsillar diphtheria • Fever, hoarseness and croupy cough • Dyspnoea • necrosis in heart muscles, liver, kidneys and adrenals • vision difficulties, speech, swallowing or movements of armsor legs • paralysis of softpalate, eye muscle or extremities Toxindamage • parenchymatous degeneration 20Kuldeep Vyas M.Sc. CHN
- 21. Nasal diphtheria • Mildest form • Localized in septum or turbinatesof one side of nose • Conjunctiva and genitals also sources of infection • Membrane extends topharynx. 21Kuldeep Vyas M.Sc. CHN
- 22. Cutaneous diphtheria • Common in tropicalareas • Secondary infection of previous infection orskin abrasion • Presenting lesion-an ulcer surrounded by erythema and covered with membrane. 22Kuldeep Vyas M.Sc. CHN
- 23. 23Kuldeep Vyas M.Sc. CHN
- 24. SCHICK’S TEST Intra dermal test Tests – presence of antitoxin(immunity status)and state of hypersensitivity to diphtheriatoxin. Inject 0.2ml of Schick test toxin intradermallyinto skin of forearm, while into opposite arm- control (Schick toxin inactivated by heat) isinjected. 24Kuldeep Vyas M.Sc. CHN
- 25. Negative reactions if the person is immune, no reaction of any kind. Positive reaction In testarm, acircumscribed red flush of 10-50mm diameter appears within 24-36 hours reaching maximum development by 4th – 7th day. This slowly fades intoa brown patch and skin desquamates. Control arm shows nochange. The person is susceptible todiphtheria. 25Kuldeep Vyas M.Sc. CHN
- 26. Pseudo-positive reactions A red flush develops equally on both arms, much less circumscribed than true +vereactions. Fades by 4th day. allergic reaction found in certain individuals Schick negative Combined reactions Control arm shows pseudo positive reaction and test armshows positive reaction. The person is susceptibleto diphtheria. 26Kuldeep Vyas M.Sc. CHN
- 27. CONTROL OF DIPHTHERIA 27Kuldeep Vyas M.Sc. CHN
- 28. • Start active search immediately fromfamily and school contacts. • Carriers can bedetected by culture methods. (swabs taken from nose and throat) CASES & CARRIERS Early detection Isolation all cases, suspectedcases and carriers should be isolated, preferably in a hospital for atleast 14 days or until proved free of infection. 2 consecutive throat swabs taken 24 hours apart should be negative before terminating isolation. 28Kuldeep Vyas M.Sc. CHN
- 29. Treatment- Cases • Preliminary test dose of 0.2 ml subcutaneouslytodetectsensitization to horseserum. • Followed bydip: antitoxin IM or IV in doses ranging from 20,000-40,000 units or more depending on severity ofcases. • Mild early pharyngeal or laryngeal:20,000- 40,000 units • Moderate naso pharyngeal: 40,000-60,000 units • Severe, extensive or latedisease: 80,000- 100,000 units. • Addition to antitoxin, penicillinor erythromycin for 5-6 days toclearthroat. Carriers • Should betreated in 10 days course of oral erythromycin 29Kuldeep Vyas M.Sc. CHN
- 30. CONTACTS Should be throat swabbed and immunityshould be determined. Where primary immunization was received withinthe previous 2 years- no furtheraction needed. Where primary course or booster dose of diphtheria toxoid was received more than 2 years before, only a booster dose of dip: toxoid need begiven. Non-immunized close contacts shouldreceive prophylatic penicilin orerythromycin. They should be given 1000-2000 unitsof antitoxinand actively immunized againstdiphtheria. 30Kuldeep Vyas M.Sc. CHN
- 31. COMMUNITY Active immunization with diphtheria toxoid of all infants as early in life as possible with subsequent boosterdoseevery 10 years thereafter. Immunization rate must be maintained athigh level. 31Kuldeep Vyas M.Sc. CHN
- 33. Combined vaccines • DPT • DTP(w) • DTP(a) • DT(d-tetanus toxoid) • dT(diphtheria-tetanus, adult type) single vaccines • FT(formal toxoid) • APT(alum-precipitated toxoid) • PTAP(purified toxoid- aluminium precipitate) • PTAH(p:t:a: hydroxide) • TAF(toxoid-anti toxin - flocculus) Antisera Diphtheriaantitoxin 33Kuldeep Vyas M.Sc. CHN
- 34. DPT -VACCINE For immunization of infants. Pertussis component enhances diphtheriatoxoid. Types- plain and adsorbed Adsorption-carried out on a mineral carrier likealuminium phosphate orhydroxide. STORAGE should not be frozen Stored in refrigerator at 2-8 degreecelsius Will loose potency if keptat room temperature fora long time. 34Kuldeep Vyas M.Sc. CHN
- 35. Optimum age- Global Advisory Group of EPI recommended that DPTan be safelyadministered as earlyas 6 weeks after birth. Doses- 3 doses of DPT each is0.5ml. Mode of admn- All vaccines containing mineral carriers should beinjected intramuscular. DPT given in upperand outerquadrantsof gluteal region. 35Kuldeep Vyas M.Sc. CHN
- 36. Immunization schedule- 6 weeks 10weeks 14 weeks 16-18 months (boosterdose) 5 years (DT) 36Kuldeep Vyas M.Sc. CHN
- 37. Reactions- Fever and mild local reactions 2-6% develop feverof 39 degree or higher. 5-10% experience swelling and induration. Neurological- encephalitis, prolonged convulsions, infantile spasms, Reye’ssyndrome. Contra indications- Seriously ill children orwho need hospitalizationare not vaccinated. Should not be repeated if a severe reaction occurred after a previousdose. In case of DPT, subsequent DTimmunization. 37Kuldeep Vyas M.Sc. CHN
- 38. For children over the age of 5 years who have not received DPT- 2 doses of DT vaccine, 4 weeksapart, with a boosterdose 6 months to 1 year later. Thosechildren who received primary courseof DPT earlier, should receive DT as boosterat 5-6 years. For immunizing children over 12 years of age and adults, preparation –dT (adult typediphtheria tetanus vaccine). Contains no more than 2 Lf diphtheria toxoidper dose. Admn:- 2 doses at interval of 4-6 weeks, followedby booster 6-12 months after seconddose. 38Kuldeep Vyas M.Sc. CHN
- 39. SINGLE VACCINES Less frequentlyused. Good immunizing agents. APT- hardly used; prone togive rise tosevere infections. Each doseof theseantigens generallycontain 25 loeffler(lf) units of DT. 39Kuldeep Vyas M.Sc. CHN
- 40. ANTI-SERA main stayof passiveprophylaxis and also for treatment in diphtheria. diphtheria antitoxin prepared in horseserum. 40Kuldeep Vyas M.Sc. CHN
- 41. 41Kuldeep Vyas M.Sc. CHN