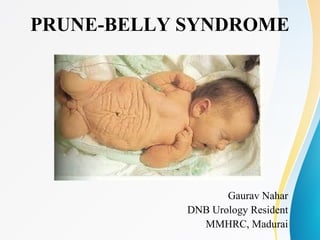
2. INTRODUCTION
• A constellation of anomalies with variable degrees of severity.
• Three characteristic findings:
1. a deficiency of abdominal musculature,
2. bilateral intra-abdominal testes, and
3. an anomalous urinary tract.
• Single most important determinant of long-term survival-
severity of the urinary tract anomaly, in particular, degree of
renal dysplasia.
3. Also known as:
• Triad syndrome,
• Eagle-Barrett syndrome, and
• Abdominal musculation syndrome
5. ...flashback
• Frolich(1839) first described the characteristic
abdominal wall in PBS.
• Parker(1895) described the full triad of
anomalies.
• Osler(1901) coined the term Prune-belly
syndrome d/t characteristic abdominal wall
findings.
6. EPIDEMIOLOGY
• Incidence: 1 in 29,000 to 1 in 40,000 live
births(similar as bladder exstrophy).
• 95% cases in males.
• PBS females exhibit abdominal wall deficiency and
urinary tract dysmorphism without any gonadal
anomaly.
• Higher incidence noted in twins, blacks, and children
born to younger mothers.
• Incidence declining in developed countries because of
prenatal diagnosis and a decision to terminate the
pregnancy.
7. GENETICS
• Most cases sporadic with normal karyotype.
• Reported association with
Turner syndrome
Monosomy 16
Trisomy 13
Trisomy 18
Beckwith Wiedemann syndrome.
Proposed inheritance patterns- X-linked recessive, 2-
step autosomal dominant, sex-influenced autosomal
recessive & polygenic transmission.
8. EMBRYOLOGY
• Exact mechanism unclear.
• Four main theories:
(1) Early in utero posterior urethral obstruction resulting
in severe dilation of urinary tract and possible fetal
ascites and oligohydramnios.
(2) Primary defect in lateral plate mesoderm (precursor
of ureters, bladder, prostate, urethra, and
gubernaculum).
(3) Intrinsic defect of urinary tract leading to ureteral
dilation and fetal ascites
(4) A yolk sac defect.
9. CLINICAL FEATURES
GENITOURINARY ANOMALIES:
Kidneys:
• Spectrum of anomalies range from normal
renal parenchyma to dysplasia.
• Dysplasia in 50%.
• Severe degree of renal collecting system
dilatation- characteristic.
• Calyceal morphology well-preserved.
10. • Severely dysplastic or dilated kidney.
• Non-obstructive hydronephrosis.
• Primary or secondary UPJO.
11. Ureters:
• Dilated, tortuous & redundant.
• Distal ureters more severely affected.
• Vesicoureteral reflux(VUR) in 75% pts.
• Histology- a lack of smooth muscle cells and
an increase in fibrous connective tissue.
• Ratio of collagen to smooth muscle cells in
prune-belly ureters is elevated.
12. • Decreased number of thick and thin myofibrils
(ultrastructural examination) contributes to
poor peristalsis.
• UPJ & UVJ obstruction- uncommon.
• Ineffective ureteral peristalsis because of poor
ureteral wall coaptation.
• Severity of urinary tract abnormalities is not
proportional to flaccidity of abdominal wall.
13.
14. • Excretory urogram (A to
C) demonstrating the
variable degree of HUN in
PBS.
• Note the preservation of
calyceal architecture,
despite severe ureteral
dilation in C.
• D, Dilated tortuous
refluxing ureters as seen on
a voiding
cystourethrogram
15. Bladder:
• Massively enlarged + Urachal
pseudodiverticulum.
• Patent urachus in 25-30%.
• Despite being very thick, bladder wall is
smooth.
• Increased ratio of collagen to muscle fibers in
the absence of obstruction.
• Delayed first sensation to void and a large
capacity.
16. • A significant postvoid residual may result
from a relative outlet obstruction and inability
of bladder to generate sufficient pressure with
a detrusor contraction.
• Despite these limitations, 50% of PBS patients
void spontaneously with normal voiding
pressures, normal flow rates, and low postvoid
residuals.
• Trigone is splayed with ureteric orifices
displaced laterally and superiorly(? cause of
VUR).
17. VCUG of a child with PBS demonstrating urethral
atresia, urachal diverticulum, and VUR
18. Prostate and Accessory Sex Organs:
• Posterior urethral dilatation d/t prostatic hypoplasia,
k/a type 4 valve- angulation of urethra during
voiding.
• Related to abnormal mesenchymal-epithelial
development.
• Reduction of both epithelial and smooth muscle cells
and increase in connective tissue cells.
• Various obstructive lesions of distal posterior
urethra:- urethral atresia, valves, urethral stenosis,
urethral membrane, and urethral diverticulum- occur
in 20% of cases.
19. • Prostatic hypoplasia may cause ejaculatory failure.
• Vas deferens and seminal vesicles are atretic; may be
dilated or thickened.
• Epididymis may be poorly attached to the testis (as is
seen commonly in abdominal undescended testes).
• Lack of continuity between efferent ductules and rete
testis.
• Retrograde ejaculation because of an incompetent
bladder neck.
20. Anterior urethra:
• Usually normal.
• Most common anomalies: urethral atresia or
hypoplasia and megalourethra.
• Unless associated with a patent urachus,
urethral atresia is lethal.
• Spontaneous bladder rupture with fistula
formation also may occur.
21. In PBS, two types of megalourethra seen.
Fusiform type:
• a deficiency of corpus
cavernosum + spongiosum.
• Entire phallus dilates with
voiding.
• results from a mesenchymal
deficiency of urethral folds.
Scaphoid variety:
• a deficiency of spongiosum
only with preservation of
glans and corpora
cavernosa.
• Ventral urethra dilates with
voiding.
• results from a mesenchymal
deficiency of urethral
supportive tissues.
22. • Megalourethra is more commonly seen in PBS
than any other syndrome.
• Transient in utero obstruction of junction
between glanular & penile urethra- proposed
cause of megalourethra.
23. Testes:
• Bilateral intra-abdominal testes lying over iliac
vessels and adjacent to dilated ureters- most
typical findings.
• Some authors found no difference in germ cell
counts, Ad spermatogonia, and Leydig cells
between PBS testes and non-PBS intra-
abdominal testes; others found decreased
numbers.
24.
25. • Infertility caused by a combination of testicular
histologic abnormalities, structural defects of the
ducts, and prostatic abnormalities.
• No PBS pts.have fathered a child. More recently,
paternity achieved by sperm retrieval techniques and
intracytoplasmic sperm injection(ICSI).
• Normal pregnancy with assisted vaginal delivery-
described in a female PBS patient.
27. Abdominal wall defect:
• Most characteristic feature in newborn-
appearance of abdominal wall.
• M.c.- uneven involvement, medial and inferior
musculature most deficient.
• Totally absent abdominal wall musculature, in
some cases.
• Appearance at birth is that of wrinkled,
redundant skin with bulging flanks. Intra-
abdominal organs can be discerned through the
thinned abdominal wall.
28. • The most severely affected areas may have
skin, subcutaneous fat, and a single fibrous
layer on the peritoneum.
• More vulnerable to respiratory illness because
their cough effectiveness is compromised
• Good wound healing.
• "Pot-belly" appearance in adults.
30. Cardiac Anomalies:
• Occur in 10% of children with PBS
• Patent ductus arteriosus,
• Atrial septal defect,
• Ventricular septal defect, and
• Tetralogy of Fallot.
31. Pulmonary:
• Pulmonary hypoplasia (sec. to severe
oligohydramnios related to renal dysplasia or
severe bladder outlet obstruction)
• Pneumothorax and pneumomediastinum can
be seen
• Pneumonia and lobar atelectasis( ineff. cough)
32. Gastrointestinal Abnormalities
• 30% of cases.
• Result from incomplete rotation of midgut
giving way to a wide mesentery
• Int. malrotation, volvulus, atresia, stenosis
• Splenic torsion
• Omphalocele, gastroschisis, and anorectal
abnormalities
• Chr.constipation and acquired megacolon( sec.
to dec. intra abd. pressure)
33. Orthopedic:
• 30% to 45%,
• Result from compressive effects of
oligohydramnios
• Dimpling of lateral aspect of the knees is a
common finding.
• Talipes equinovarus (26%), hip dysplasia
(5%), and congenital scoliosis(4%).
38. • Cardiac or pulmonary often should take precedence
over the urinary tract( in the absence of BOO)
Category 1 Category 2 Category 3
Oligohydramnios Marked
Moderate to
severe
mild/nil
BOO severe( uret. atresia) nil
Pulm Hypoplasia severe mild nil
Prognosis
succumb within few
days / still born
variable good
Urologic
intervention
Not usual- cath. drain Mx controversy
nil or if rec.
UTI/VUR
Early reconstr. - for VUR/ red.
cystoplasty (after 3 mths age)
cons.mx/limited sx
39. Adult Presentation
• Incomplete forms of PBS- present into
adulthood.
• Symptoms of renal failure and hypertension.
Female Syndrome- 5%
• BOO with anorectal anomalies similar to
males
40. EVALUATION & MANAGEMENT
• Requires a team consisting of a neonatologist, a
nephrologist, and a urologist.
• Major initial concern is that of management of
cardiac and respiratory issues- do CXR.
• Pts.with BOO- SPC initially.
• BUN,creat,electrolytes - assess renal insuff, met.
acidosis.
• S.Creat <0.7 % predictive of adeq.renal function.
41. • Circumcision is advisable- reduce risk of
infant urinary tract infections.
• Prophylactic antibiotic therapy is
recommended- before VCUG.
• VCUG- assess Bladder emptying, outlet( esp.
in renal insuff)
• Avoid early VCUG - in normal renal function,
patent urachus.
• DTPA/MAG3 to assess outflow obstruction in
massive HN & stasis(4-6 weeks of age).
42. SURGICAL MANAGEMENT
Three components:
• Urinary tract reconstruction,
• Abdominal wall reconstruction, and
• Orchidopexy
Supravesical Urinary Diversion
• Indications: Repeated upper tract infections or
deterioration of renal function.
• Cut. Pyeloplasty/ureterostomy( UPJO/UVJO)
43. Cutaneous Vesicostomy
• Indications: Acute renal failure, urinary sepsis, or
bladder outlet obstruction from urethral atresia.
• OR Excise large urachal diverticulum
Internal Urethrotomy
• True anatomic obstruction- rare in PBS
• Used in "Unbalanced Urethrovesical function"- with
large PVR.
• Does not result in incontinence.
44. Reduction Cystoplasty:
• Poor bladder contractibility leads to
incomplete and infrequent emptying.
• Remodeling into a more spherical shape to
better direct the contractible forces.
• Simple excision of urachal diverticulum or
excision of redundant mucosa with overlaping
between flaps.
45. Anterior Urethral Reconstruction:
• Urethral atesia/hypoplasia- progresive UD
not successful.
• Urethroplasty with skin flaps / grafts
• Megalourethra- redundant urethra excised,
and reconstructed over catheter.
46.
47. Ureteral Reconstruction:
• Indications: Repeated nonsuppressible UTI or
with progressive upper tract deterioration.
• Ureteral reimplantation may be technically
challenging- abnormal bladder.
48. Orchidopexy:
• Timing of orchidopexy- early: to preserve
normal hormonal function.
• Transabdominal Orchidopexy- at 6 months
current approach of choice.
• If adequate mobilisation not possible -
• Fowler-Stephens orchidopexy(Single or
multi-staged)
• Microvascular autotransplantation.
49. Operative photograph showing increased vacularity along vas
deferens 4 months after first-stage Fowler-Stephens orchidopexy
50. Reconstruction of Abdominal Wall:
• Mild degree- may show improvement with
age.
• Benefits- improved bladder emptying, more
effective cough and improvement in
defecation.
• Timing - can be combined with other urinary
tract reconstructions, even at 6 months.
51. Prune-belly syndrome patient demonstrating preoperative
appearance of abdominal wall (A), estimated extent of abdominal
wall resection (B), and immediate postoperative appearance (C).
52. A and B, Anterior and lateral views of the abdomen of a 14-year-old boy who underwent
major surgical remodeling of the urinary tract during early infancy with good results.
Note typical abdominal configuration. C and D, Anterior and lateral views of the same
boy 1 month after undergoing abdominoplasty with the technique described by Monfort
53. Techniques:
Randolph Technique-
• Transverse incision from 12th rib to pubic
symphysis to opposite 12th rib with full-
thickness removal of skin, lower abdominal
musculature, and peritoneum.
• Healthy fascia is then approximated to anterior
iliac spines, pubic tubercle, and inferior fascia.
• Disadv.- Lateral abdominal bulge persists.
54. Ehrlich Technique-
• Vertical midline incision, preservation of
umbilicus on a vascular pedicle from inferior
epigastric artery.
• Skin and subcutaneous tissues are elevated off
the muscle and fascial layers, and
• an overlapping, vest-over-pants advancement
of each side to contralateral flank is
performed, preserving the less affected lateral
muscles and fascia.
55. Monfort Technique-
• An elliptically oriented incision isolates the redundant skin,
extending from the tip of xiphoid to pubis. A second incision
is made around umbilicus to preserve it in situ.
• Skin and subcutaneous tissue are dissected off the attenuated
fascia and muscle with dissection extending laterally to
anterior axillary line.
• Vertical fascial incisions are made lateral to superior epigastric
arteries, leaving a central fascial bridge.
• If intraabdominal surgery is necessary, excellent exposure to
urinary tract or abdominal testes is afforded through these
lateral fascial incisions.
• The lateral fascia is then advanced over central fascial bridge
from both sides, alleviating redundancy and increasing
thickness of abdominal wall.
60. LONG-TERM OUTLOOK
• If the nadir value is less than 0.7 mg/dL, renal
function tends to be stable
• 30% of patients- with impaired renal function -
develop ESRD at adolscence - need renal
transplant.