
Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Carotid artery stenosis
Semelhante a Carotid artery stenosis (20)
Carotid artery stenosis
- 1. View Carotid Artery, Stenosis Page 1 of 54 View Topic Carotid Artery, Stenosis Author: Lennard A Nadalo, MD, Clinical Professor, Department of Radiology, University of Texas Southwestern Medical School; Consulting Staff, Envision Imaging of Allen and Radiological Consultants Association. Lennard A Nadalo is a member of the following medical societies: American College of Radiology, American Society of Neuroradiology, American Society of Pediatric Neuroradiology, Radiological Society of North America, and Texas Radiological Society. Coauthor(s): Michelle C Walters, DO, Consulting Staff, Radiological Consultants Association Editors: Robert A Koenigsberg, DO, MSc, FAOCR, Professor, Director of Neuroradiology, Program Director, Diagnostic Radiology and Neuroradiology Training Programs, Department of Radiology, Hahnemann University Hospital, Drexel University College of Medicine; Bernard D Coombs, MB, ChB, PhD, Consulting Staff, Department of Specialist Rehabilitation Services, Hutt Valley District Health Board, New Zealand; Douglas M Coldwell, MD, PhD, Professor of Radiology, Director, Division of Vascular and Interventional Radiology, University of Louisville School of Medicine; Robert M Krasny, MD, Resolution Imaging Medical Corporation; Kyung J Cho, MD, FACR, William Martel Professor of Radiology, Interventional Radiology Fellowship Director, University of Michigan Health System. Synonyms, Key Words, and Related Terms carotid artery stenosis, carotid plaque, ulcerated carotid plaque, carotid artery stenosis, carotid arterial stenosis, stroke, brain attack, CVA, cerebrovascular accident, carotid stenosis, carotid bruit, extra cranial carotid occlusive disease Introduction Background Stroke (brain attack) represents one of the most serious causes of mortality and morbidity in the United States and throughout the world. Each year, 150,000 patients die as a direct result of a cerebrovascular accident (CVA), while 600,000 patients experience the morbidity of aphasia, blindness, or paralysis. Among patients with stroke, extracranial carotid disease represents the cause of approximately one half of cases. The goals of carotid imaging can be described as early detection, clinical staging, surgical road mapping, and postoperative therapeutic surveillance (see Image 1). http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
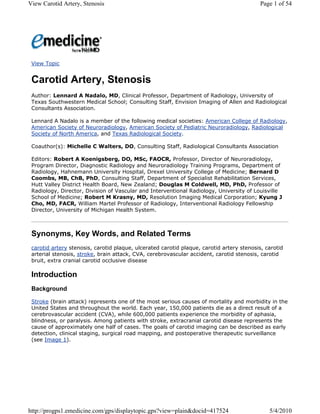
- 2. View Carotid Artery, Stenosis Page 2 of 54 Four of the most common methods of imaging the carotid artery are compared. Angio = angiography, CTA = CT angiography, Duplex = duplex ultrasonography, Gd = gadolinium enhancement, ICA = internal carotid artery, MRA = magnetic resonance angiography, TOF = time of flight. Surface-rendered 3-dimensional volume CT angiogram demonstrates a complete occlusion of the right common carotid artery (CCA). Imaging helps in detecting associated conditions early. Coronary artery disease, peripheral arterial stenosis, and hypertension are associated with an increased incidence of carotid arterial stenosis. Carotid arterial screening remains controversial. Good evidence supports evaluation for carotid stenosis prior to coronary arterial bypass surgery.1, 2, 3 Detection of a carotid bruit is a common physical examination finding that may lead to a referral for carotid duplex sonography. The correlation between a carotid bruit and a hemodynamically important carotid stenosis is reported to be between 10-20%. A cardiac murmur may be transmitted to the neck. Stiff, calcified, or torturous vessels may generate a bruit in the absence of stenosis. Recent study The use of intravenous tissue plasminogen activator (t-PA) for stroke 3-4.5 hours after symptom onset has been endorsed by the American Heart Association, although time to treatment remains of extreme importance and should not be delayed. The European Cooperative Acute Stroke Study 3 (ECASS 3) showed benefit from t-PA in patients treated 3-4.5 hours after onset of 4, 5, 6, 7 symptoms of stroke. For excellent patient education resources, visit eMedicine's Stroke Center and Dementia Center. Also, see eMedicine's patient education articles Stroke, Transient Ischemic Attack (Mini-stroke), and Stroke-Related Dementia. Pathophysiology Transient ischemic attack (TIA) is the result of a brief interruption of blood flow to the brain. In 80% of cases, the interruption occurs as a result of blockage in the arterial circulation to the http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 3. View Carotid Artery, Stenosis Page 3 of 54 brain due to an embolus, an obstructing arterial thrombus, or the stenotic effects of atherosclerosis. In the other 20%, the interruption is caused by minor hemorrhage in the brain. In both types of TIA, the lack of oxygen to the brain produces symptoms similar to those produced during a full stroke. Symptoms can affect vision, behavior, movement, speech, and thought processes. However, the symptoms of a TIA are temporary, generally lasting only 8-14 minutes with most clearing within an hour, although they can continue for as long as 24 hours. Permanent damage is unlikely because the oxygen supply to the brain is restored fairly quickly. Thrombus causes 25-50% of all TIAs, and embolism causes 11-30%. A lacunar infarction occurs in 11-14% of patients with TIA. Less common causes of a TIA involve minor bleeding or sentinel leaks from a cerebral blood vessel (approximately 10% of cases). Mini strokes caused by bleeding are usually due to high blood pressure (hypertension). Since the underlying cause of this type of TIA is bleeding rather than blockage, the patient must receive an immediate and accurate medical evaluation. Treatment should not include thrombolytic drugs or aspirin because these agents increase bleeding. Once blockage or bleeding occurs, whether the person is about to have a TIA or a full stroke depends greatly on host factors, eg, the person's age and general health status and the location and size of the blockage or bleed. Other blood vessels in the area may enlarge to improve blood flow to the affected area, thus ending the TIA. Although a TIA is characterized by a brief interruption of blood flow, symptoms of a TIA (eg, weakness on 1 side of the body) may last much longer than the time needed to dissolve the blockage completely or to absorb the bleed. For most people, symptoms last approximately 8-14 minutes and usually clear within an hour, but they can last as long as 24 hours. Patients with symptoms of a TIA that persist for more than 24 hours usually are treated as though they have had a full stroke. More than 50,000 Americans have TIAs every year. In persons older than 65 years, 8.5% have been diagnosed with at least 1 mini stroke. The risk of stroke is highest soon after a TIA, and the risk continues to be approximately 5% during the first month following the TIA. Of patients with TIAs, 20-25% are estimated to develop a stroke within 2 years. If the degree of carotid stenosis is severe, in the absence of adequate collateral circulation the ipsilateral cerebral hemisphere may become underperfused. When the arterial circulation falls, there is an increased risk of thrombosis within the middle cerebral artery (MCA), the anterior cerebral artery, and the more peripheral branches of the intracranial arterial circulation. Focal thrombosis may occur in areas of pre-existing atherosclerotic disease. Other general medical issues which may exacerbate symptoms related to carotid stenosis include chronic lung disease, cardiac disease with restricted cardiac function, and attempts to low systemic hypertension. Any adverse physiological change which further limits oxygenation to the brain may result in cerebral ischemia in patients who otherwise tolerated even high-grade carotid stenosis. The presence of 2 or more tandem arterial stenoses may result in symptomatic cerebral ischemia, even if any one of the narrowed arterial inflow circulation pathways was not critically narrowed. Frequency United States The prevalence of hemodynamically significant carotid stenosis varies with age and other risk factors. Estimates indicate that 5 per 1000 persons aged 50-60 years and approximately 10% of persons older than 80 years have carotid stenosis greater than 50%. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 4. View Carotid Artery, Stenosis Page 4 of 54 Strokes were responsible for more than 150,000 deaths in 1998. Stroke is the third leading cause of death in the United States after heart disease and cancer. Each year, approximately 600,000 people have a stroke, and in 100,000 people, strokes recur annually. Approximately one half of all strokes result from significant extracranial arterial disease. International Carotid stenosis and CVA follow a similar pattern of occurrence within the developed world. A direct relationship exists between cigarette smoking and a diet rich in fat. The occurrence of carotid vascular disease probably is lower in underdeveloped countries; however, absolute incidence is difficult to measure. Mortality/Morbidity Patients with carotid artery stenosis are at increased risk for subsequent stroke, myocardial infarction (MI), and death. The risk of stroke is greatest for persons with neurologic symptoms such as TIAs, but it also is increased in patients with asymptomatic lesions. The proportion of all strokes attributable to previously asymptomatic carotid stenosis is small; however in patients older than 60 years who have cerebral infarction, approximately 15% have ipsilateral carotid stenosis of 70% or greater. The frequency of hemodynamically significant carotid artery stenosis is higher in symptomatic patients than in asymptomatic patients. In 40-50% of those with a complete stroke, the primary etiology of the stroke is related to extracranial carotid disease (stenosis). Morbidity of a true transient CVA is nil. Without a completed infarction, the ischemic brain should return to a normal functional state. However, if the period of cerebral ischemia persists beyond 12-24 hours, even a seemingly full neurologic recovery is commonly associated with imaging findings of focal cerebral infarction. Beyond 24 hours and up to 48 hours following the initial CVA, neurologic recovery may be nearly complete, with small areas of infarction best demonstrated on T1-weighted diffusion cerebral MRIs. The completed infarct syndromes involve neurologic defects that persist beyond the period of active medical treatment in patients with acute stroke. The specific morbidity related to a stroke is a reflection of the portions of the brain that have become ischemic and is related closely to the cerebral vessels that are stenotic or thrombosed. Common stroke syndromes that may result from carotid stenosis, ulceration, or occlusion include the following: • Regarding common and internal carotid artery (ICA) occlusion syndromes, young people with occlusion of the main trunk may be asymptomatic. Other manifestations of ICA occlusion include transient hemiplegia, persistent hemiparesis, unilateral loss of vision if the ophthalmic artery is involved, and aphasia when the dominant side is thrombosed. • Embolization to the anterior cerebral artery or critical stenosis of carotid artery may affect the major branches of the anterior cerebral artery (medial striate artery, recurrent artery of Heubner, orbitofrontal artery, frontopolar artery, anterior internal frontal artery, middle internal frontal artery, posterior internal frontal artery, callosomarginal artery, pericallosal artery, and parieto-occipital artery). • Anterior cerebral occlusion syndrome involving the main trunk results in contralateral hemiplegia (lower extremity), mild sensory deficits of the contralateral lower limb, and mental confusion or clouding of consciousness. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 5. View Carotid Artery, Stenosis Page 5 of 54 • The middle cerebral artery, including the major branches (striate arteries, anterior cerebral head of caudate septum pellucidum, middle cerebral globus pallidus, anterior temporal branch, and orbitofrontal, operculofrontal, central sulcus, posterior parietal, angular, and posterior temporal branches) may be directly affected by embolization, or a thrombosis may result due to proximal stenosis of the ipsilateral ICA. • Middle cerebral occlusion syndrome of the main trunk results in coma, contralateral flaccid hemiplegia, hemianesthesia hemianopia, and motor and sensory aphasia (dominant hemisphere). • Middle cerebral occlusion syndromes of the posterior parietal, angular, or posterior temporal branches result in contralateral hemiparesis, contralateral astereognosis, contralateral homonymous hemianopia, sensory aphasia, agnosia, apraxia, and alexia if on dominant side. • Embolization to perforation branches results in contralateral hemiplegia, contralateral rigidity, and tremor. • Posterior cerebral branches, including major branches (anterior temporal artery, posterior temporal artery, posterior occipital artery, calcarine artery, and collateral arteries), may be involved. The primary blood flow pattern to the posterior cerebral artery may arise from the ICA. The stroke pattern resulting from embolization or stenosis affects the related cerebral structures, ie, the anterior temporal artery (inferior temporal lobe), posterior temporal artery (inferior temporal lobe), posterior occipital artery (inferior and medial occipital lobe, posterior corpus callosum), calcarine artery (calcarine cortex occipital lobe), and collateral arteries (thalamogeniculate thalamoperforating branches). • Posterior cerebral occlusion syndrome of the main trunk includes contralateral hemianesthesia, contralateral homonymous hemianopia, sensory aphasia if on the dominant side, ipsilateral cerebellar signs, contralateral rigidity, tremors, and choreiform movements. • Retrolenticular capsule includes hemiplegia hemihypalgesia, hemianesthesia, and contralateral homonymous hemianopia. • Involvement of the calcarine artery includes contralateral homonymous hemianopia, loss of half of the person's macular vision, visual agnosia if on the dominant side, thalamic syndrome, contralateral hemianalgesia, contralateral dysesthesia, and pain. Race Strokes are more common among blacks and Hispanics than others. The incidence of CVA tends mirror the incidence of hypertension and diabetes. The rate of diabetes among Hispanics is greater than in the population as a whole. Hypertension is both more severe and more common among blacks than among others. The factors of diet, obesity and family history interact to result in a greater risk of carotid stenosis in both blacks and Hispanics. Treatment of patients who are asymptomatic for carotid stenosis and the overall management of hypertension tend to be less successful among patients of lower socioeconomic status, resulting in more frequent and more severe strokes. To the extent that blacks and Hispanics represent a greater percentage of the population in poverty, the medical treatment of strokes in minority patients has a worse outcome. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 6. View Carotid Artery, Stenosis Page 6 of 54 The complex interassociation of genetics, diet, and lifestyle is reflected by the relatively low rates of vascular disease reported among elderly persons living in remote areas of Italy and China. Sex Carotid stenosis requiring surgical treatment tends to occur in almost equal frequency in men and women. In general, women are more likely to seek and receive treatment for both benign and symptomatic carotid stenosis. Age Extracranial carotid disease tends to occur more frequently in elderly persons. In patients with increased risk factors, the age at first presentation tends to be younger. Anatomy Anatomy and variants The aortic arch presents many anatomic variations that may affect the treatment of patients with carotid stenosis. The most common aortic arch variant has 3 primary branches, ie, the innominate artery, the left common carotid artery (CCA), and the left subclavian artery. The right CCA arises from the innominate artery. The most common variant has a single (bovine) origin of the innominate artery and the left CCA (see Image 2). Thoracic arch angiography demonstrates one of the common variants of normal aortic arch (AA) development in which both the innominate artery (IA) and the left carotid artery share a common origin. The right common carotid artery (RCA) and the right internal carotid artery are irregular and narrowed. The long, multisegment areas of stenosis are believed to result from the effects of radiation therapy to the right side of the neck in this patient. Effects of radiation therapy are related to adverse effects on the vascular supply to the carotid or vertebral artery in the radiation field. The right subclavian artery may take its origin from the aortic arch distal to the left subclavian artery, in which case, the first aortic arch branch usually is the right CCA. Stenosis of the proximal origin of the CCA or the innominate artery may result in clinical cerebral ischemia and must be differentiated from carotid stenosis because the surgical approach is entirely different. The CCA bifurcates in the cervical region to form the external carotid artery (ECA) and the ICA. The level in the cervical region at which the bifurcation occurs is highly variable. Occasionally, the origin of the ICA occurs at or above the angle of the mandible. Four primitive connections that normally regress occur between the anterior and the posterior circulations. The persistent trigeminal artery is the most common anomaly. The persistent hypoglossal artery occurs at a rate of approximately 0.2%. Clinically, significant stenosis may occur at the origins of http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 7. View Carotid Artery, Stenosis Page 7 of 54 both normal and anomalous vessels. The normal internal diameter of the ICA is highly variable. Within the same normal vessel, the diameter of the ICA varies and is larger in the proximal carotid bulb. As a result of normal variations, the absolute internal diameter is less significant than the ratio of the diameter of a stenotic vessel to the normal diameter of the distal ICA. Vascular causes of stroke The cervical portion of the CCAs and ICAs form the primary basis for diagnosis and treatment of carotid stenosis (see Image 5). Surgical treatment and prevention of stroke is directed toward the detection of extracranial carotid vascular disease because effective surgical treatment is limited to the cervical carotid artery and the brachiocephalic branches of the aorta. Extracranial carotid occlusive disease accounts for more than one half of strokes. While stenosis, thrombosis, and anomalies of the aortic arch may contribute to unusual collateral blood flow, stenosis and plaque ulceration within the common carotid bulb and proximal ICA indicate the primary anatomic structures found in the surgical treatment of stroke. Common carotid angiogram shows normal findings. Note the slightly dilated shape of the distal common carotid artery and the proximal internal carotid artery (carotid bulb). ec = external carotid artery; f = facial artery; l = lingual artery; ic = internal carotid artery; im = internal maxillary artery; o = occipital artery; p cer = posterior cerebral artery; p com = posterior communicating artery The ECA and its branches provide important collateral pathways, which may reduce the ischemic effects of an ICA stenosis (see Image 19). The primary external carotid arterial pathways involve branches of the ophthalmic artery, the internal maxillary artery, and the occipital artery. Plaque in the proximal ECA may result in a bruit, which can result in diagnostic confusion. Rarely, the ECA may become the source of distal embolization through enlarged collateral pathways. The ICA can be divided into a cervical portion, an intrapetrosal portion to the cavernous sinus, an intracavernous segment, and a supraclinoid segment with major distal branches including the anterior cerebral and MCAs. Major branches of the ICA include the ophthalmic, meningohypophyseal, posterior communicating, anterior choroidal, anterior cerebral, and MCAs. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 8. View Carotid Artery, Stenosis Page 8 of 54 Carotid Artery, Stenosis. Sagittal MPR image from a carotid CTA in a patient with sudden onset of aphasia. The proximal left ICA demonstrates a short segment of complete occlusion with flow preserved in the more distal left ICA. The common carotid artery (CCA) has a normal diameter. Decreased cerebral arterial perfusion can result in symptomatic cerebral ischemia if a significant degree of stenosis occurs at most points along the blood pathway from the aortic arch to the end intracranial vessels. Atherosclerotic stenosis tends to occur near the origins of major branch arteries and within the area of vascular turbulence. This is most likely related to intimal trauma, which tends to occur near the origins of arterial branches. Assessment of a patient who presents with cerebral vascular disease should include a search for an inflow stenosis near the origin of the right innominate artery or the proximal left CCA. In the most common anatomic presentation, the right CCA and the right subclavian artery arise from the innominate artery. Stenosis of the innominate artery may result in right-sided vertebral arterial steal as well as symptomatic reduction of right carotid arterial blood flow. Because of the larger diameter of the innominate artery, symptomatically significant stenosis of the innominate artery is less common than stenosis of the proximal left common artery. Clinical Details Risk factors for carotid artery disease are similar to those for coronary artery disease, ie, atherosclerosis of the main arteries that carry the oxygen-rich blood to the heart (coronary arteries). Therefore, people with one condition often also have the other. Risk factors for both (as shown by a coronary risk profile) that can be modified include smoking, lack of regular exercise, eating a high-fat high-cholesterol diet, obesity (>20% over an individual's ideal weight), uncontrolled diabetes, uncontrolled hypertension, uncontrolled stress and anger, high low-density lipoprotein (bad cholesterol) levels, and low high-density lipoprotein (good cholesterol) levels. Risk factors that cannot be modified include (1) sex, ie, men are more likely to have a stroke and survive, women are more likely to die as a result of stroke; (2) advanced age, ie, cardiovascular diseases tend to affect older people more than younger people; and (3) ethnicity, ie, African Americans have a higher risk of high blood pressure than others. TIA is a warning sign of a future stroke. An estimated 25% of patients with TIA develop a stroke within the next 2 years. Symptoms of a TIA include weakness, numbness or tingling on one side of the body, confusion, trouble with speaking, difficulty understanding speech, vertigo, and severe headache. TIAs also may cause a variety of visual symptoms that include partial loss of vision or complete blindness, double vision, abnormal eye movements, blurred vision, and a gray shading or fogging within the field of vision. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 9. View Carotid Artery, Stenosis Page 9 of 54 Medical treatment for mild to moderate carotid stenosis is most appropriate. Treatment is directed toward reducing the progression of the atherosclerotic disease process by lowering serum cholesterol levels, controlling hypertension, and by the administration of a medication such as aspirin, which decreases the likelihood of platelet or small clot embolization. Carotid endarterectomy of asymptomatic carotid stenosis is most commonly limited to lesions with a 70% or greater degree of stenosis.8 Asymptomatic carotid stenosis may be detected by the auscultation of a cervical (neck) bruit or other screening method. Symptomatic carotid stenosis (SCS) is characterized by an associated stroke, TIA, transient monocular (1 eye) blindness, or other objective symptom or sign of an ipsilateral cerebral vascular event. Treatment for most SCS is surgical. More recently, carotid stenosis has been successfully managed by means of endovascular carotid stent placement. The selection of a specific clinical treatment is based upon the degree of stenosis, the condition of the arterial vessels proximal to the carotid stenosis, and the availability of specific treatment options. Preferred Examination A complete medical history should be taken first. On the basis of risk factors and the family history and current symptoms, selecting a screening examination such as duplex carotid sonography, CT angiography (CTA), or magnetic resonance angiography (MRA) of the carotid 9 artery may be appropriate (see Image 1, Images 13-15). Four of the most common methods of imaging the carotid artery are compared. Angio = angiography, CTA = CT angiography, Duplex = duplex ultrasonography, Gd = gadolinium enhancement, ICA = internal carotid artery, MRA = magnetic resonance angiography, TOF = time of flight. Oblique 3-dimensional contrast-enhanced magnetic resonance (MR) angiogram of the aortic arch and brachiocephalic vessels shows high-grade stenosis of the proximal left subclavian artery (white arrow). By using such a model, full depiction of the arch, brachiocephalic vessels, and carotid bulbs is possible. Because of superimposed structures, full rotation of the arterial model is necessary. Note the left common carotid artery (LCCA) behind the left jugular vein. The left subclavian artery (LSCA) is seen well (blue arrow). http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 10. View Carotid Artery, Stenosis Page 10 of 54 Carotid Artery, Stenosis. Axial CT of the brain in a patient with the sudden onset of aphasia. Carotid Artery, Stenosis. Duplex carotid sonography in a patient with sudden onset of aphasia. The images are taken from the common carotid artery. After obtaining the medical history, carotid duplex imaging is performed most commonly in patients with moderate risk factors. In the author's practice, duplex sonography is the initial triage examination for patients with an asymptomatic bruit, known asymptomatic carotid vascular disease, and in patients with a complete stroke without prior history of carotid stenosis. In symptomatic patients and in most who present with abnormal carotid sonographic findings, another imaging test is performed. MRA or CTA offer full depiction of the cervical and cerebral portions of the CCA and ICA. In most cases, a diagnostic evaluation for cerebral vascular disease can be performed by using either MRA or CTA. The immediate availability of CTA in many critical hospitals on a 24-hour basis makes CTA attractive in the care of patients who present after hours in the emergency department. In the selection of patients for acute treatment for cerebral ischemia, axial CT images should be reviewed by using the criteria of less than one-third involvement of the middle cerebral distribution or by using the Alberta Stroke Program Early CT Score (ASPECTS). The role of cervical-cerebral angiography is evolving as less invasive alternative tests have become available. Many experienced vascular surgeons are more comfortable with cervical-cerebral catheter angiography than with other studies. In the author's practice, clinicians perform carotid angiography routinely, and cerebral angiography or digital subtraction angiography (DSA) is reserved for patients who are likely candidates for surgery or for patients who may benefit from angiographically based carotid intervention. Limitations of Techniques Although carotid duplex imaging offers an excellent means of initial evaluation of the extracranial cerebral vessels, the presence of dense calcifications in the carotid plaque tends to make the http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 11. View Carotid Artery, Stenosis Page 11 of 54 study less accurate (see Image 20). Because carotid duplex imaging does not help in assessing the intracranial portion of the carotid artery, tandem lesions of the ICA may be missed. In a similar manner, proximal stenosis of the innominate artery and the left carotid artery cannot be evaluated near the origins from the aortic arch. Carotid Artery, Stenosis. The anterior communicating artery (AComA) represents an important collateral circulation which preserves blood flow to the left middle cerebral artery (L MCA) in this patient with sudden onset of aphasia. The proximal left ICA was noted to be occluded on the CTA of the cervical carotid arteries. MRA is contraindicated in patients who have cardiac pacemakers or cerebral aneurysm clips or in those who have undergone certain other medical procedures. In addition, MRA is highly motion sensitive. Many patients require sedation. Because of artifacts related to the MRA image, the degree of stenosis may be overestimated. CTA requires iodinated contrast agents to be injected at a relatively high flow rate. Patients with renal disease may not tolerate intravenous contrast agents. Motion artifacts remain a problem if the examination is performed by using older CT equipment (see Images 20-21). Carotid Artery, Stenosis. Duplex sonography of the external carotid artery in a patient who presented with the sudden onset of aphasia. Lateral selective right common carotid arteriogram. Only the proximal few centimeters of the internal carotid artery are patent (arrow). Selective catheterizations in the performance of carotid angiography provide higher resolution (smaller field of view), http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 12. View Carotid Artery, Stenosis Page 12 of 54 high concentrations of intraluminal contrast agent, and extended angiographic imaging (longer runs of images). The almost occluded internal carotid artery is evaluated better by using selective common carotid angiography. Lateral common carotid arteriogram in a patient with a neck bruit. Note the focal narrowing of the proximal internal carotid artery (arrow). In severe cases, the kink may require carotid artery reconstruction. Anterior left common carotid arteriogram in a patient who presented with a loud left neck bruit. Note the horizontal line (arrow) in the proximal internal carotid artery, which represents a focal folding of the carotid artery. This configuration has been termed a kink. The bruit results from the turbulent blood flow through the focal narrowing. Lateral common carotid arteriogram in a patient with transient ischemic attacks. A small filling defect is noted in the common carotid bulb (arrow). A small blood clot was found at surgery, with intimal ulceration at the base of the clot. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 13. View Carotid Artery, Stenosis Page 13 of 54 Carotid Artery, Stenosis. Proximal duplex sonography of the left ICA in a patient who presented with the sudden onset of aphasia. Cerebral angiography also involves the injection of iodinated contrast agents. The overall contrast dose is similar to that required for CTA. The performance of catheter-based cervical- cerebral angiography depends on the skill and experience of the angiographer. Overall major morbidity rates are 0.1-1%. Injury may occur in the form of iatrogenic stroke or bleeding around the catheter introduction site. Angiograms do not provide much information concerning the nature of the plaque lesion. Cerebral angiography is the most costly means of carotid stenosis evaluation. If cases are selected carefully, the overall risk of diagnostic angiography together with the morbidity related to carotid surgery is less than the risk of stroke for the untreated patient (see Images 6-9, Image 11, Image 17). Differentials Alzheimer Disease Aorta, Dissection Arteritis, Giant Cell Brain, Aneurysm Brain, Arteriovenous Malformation Brain, Capillary Telangiectasia Brain, Cavernous Angiomas Brain, Hypertensive Hemorrhage Brain, MRI Appearance of Hemorrhage Brain, Stroke Brain, Venous Sinus Thrombosis Coronary Artery Disease Embolization, Hemorrhage Other Problems to Be Considered Radiograph Findings Standard radiographs may demonstrate calcification in the carotid vessels in the neck; however, only large calcified plaques are demonstrated on radiographs. In general, the information provided by radiographs of the neck or skull is not clinically helpful except to alert the clinical physician that the patient may be at risk for carotid stenosis. Degree of Confidence In general, calcification in a plaque indicates a chronic disease pattern. The absence of calcification on radiographs of the neck or lateral aspect of the skull does not exclude significant extracranial carotid disease. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 14. View Carotid Artery, Stenosis Page 14 of 54 False Positives/Negatives Calcification in the carotid bulb is not fully correlated with significant carotid arterial stenosis. High-grade stenosis of the proximal carotid artery may occur in the absence of calcifications, and dense carotid calcification may be seen in the absence of a high-grade carotid stenosis. CT SCAN Carotid Artery, Stenosis. Axial CT of the brain in a patient with the sudden onset of aphasia. CT and CT angiography in a patient with a load left neck bruit and symptoms of a transient ischemic attack. A, CT scan demonstrates that the left jugular vein (LJV) is superimposed on the left common carotid artery (LCCA). B, After electronic removal of the superficial left jugular vein, a high-grade stenosis of the origin of the left external carotid artery (LECA) is demonstrated clearly. Dense calcifications are seen (red arrows) near the origins of both the left external carotid artery and the carotid bulb. The left internal carotid artery is not significantly stenotic. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 15. View Carotid Artery, Stenosis Page 15 of 54 Oblique multiplanar reformatted CT angiogram demonstrates a mild degree of stenosis in the proximal right internal carotid artery (RICA). RJV = right jugular vein. Maximum intensity CT angiogram demonstrates mild bilateral carotid stenosis. L = left, R = right. Surface-rendered 3-dimensional volume CT angiogram demonstrates a complete occlusion of the right common carotid artery (CCA). Axial CT angiograms (A and B) demonstrate bilateral occlusions of the right and left common carotid arteries (arrows). http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 16. View Carotid Artery, Stenosis Page 16 of 54 Intracranial CT angiogram in a patient with bilateral common carotid occlusion shows an absence of flow in the right and left internal carotid arteries (ICAs). ACA = anterior cerebral artery, MCA = middle cerebral artery, PCA = posterior cerebral artery, PCCA = posterior communicating cerebral artery. Axial CT image of a patient with a focal stenosis of the internal carotid artery. The cavernous sinus (CS) is distended, with an abscess (arrowheads). Stenosis of the intracavernous internal carotid artery was a response to the abscess in this patient. Findings Axial CT images of the cerebral circulation provide both an accurate means of assessing stenosis and carotid plaque. Although early attempts to apply CT in the evaluation of the carotid artery were limited by movement artifacts and thick scanning sections, current multisection CT scanners allow for the acquisition of thin (eg, 1.0-2.0 mm) axial images within a brief time (a single breath hold). Intravenous contrast material must be injected rapidly enough (3-4 mL/s for a total volume of 120-150 mL of 300-320 mg/mL nonionic contrast agent) to achieve a contrast density of at least 150 HU or in the innominate and carotid inflow to continuing distally into the intracranial carotid artery. Imaging begins just before the contrast density peaks in the carotid 10 artery. Initially, all images should be reviewed in the axial plane (see Image 34). Multiplanar and curved multiplanar reformatted images are often helpful (see Image 21, Image 24). The intraluminal diameter should be measured by using an electronic workstation with electronic calipers. If the image of the carotid artery is enlarged before measurement, error is reduced. Measurements are made across the lumen through the narrowest portion of the proximal ICA and across the area of the ICA that is above the stenosis and is believed to be normal. The degree of stenosis is calculated according to criteria developed by the North American Symptomatic Carotid Endarterectomy Trial (NASCET) and is reported as a percentage of stenosis (see Image22, Images 24-25). Carotid ulceration http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 17. View Carotid Artery, Stenosis Page 17 of 54 Another mechanism related to cerebral infarction is embolization from the heart or great vessels. Except to acknowledge the need to evaluate some patients after MI by using echocardiography, the heart as a source of cerebral emboli is beyond the scope of consideration for this article. The carotid arteries may be a source of cerebral emboli via release of the contents of the plaque, via turbulence or clot formation on the ulcerated surface. Carotid ulcers are best demonstrated by using the higher resolution of catheter angiography; however, the use of multisection CTA increases the likelihood of carotid ulcer identification. Larger deeper ulcers are successfully depicted with most CTA techniques (see Image 29). Carotid plaque Dense calcifications in the carotid artery limit the accuracy of measurements of the degree of stenosis across the plaque if maximum intensity projection (MIP) or shaded-surface display imaging is used. After first attempting to measure the degree of stenosis by using axial images, curved multiplanar reformatted images obtained through the lumen help show the stenosis. Certain workstation techniques can be applied that can image reverse the pixels above 300 HU. Image inversion subtracts calcified plaque from the image, which tends to result in a clearer image of the contrast agent–filled carotid lumen. Occasionally, contrast may be seen entering the subintimal area of the plaque. Complex and dissected carotid plaques may be detected in this manner (see Image 20). Carotid thrombosis Care must be exercised in cases of carotid thrombosis. Very slow flow rates may be missed if the timing of the intravenous contrast agent bolus or the peak density of the contrast material is less than optimal. Comparison of 3-dimensional (3D) volume images should always be made to axial images (Images 33-34). The intracranial collateralization pattern helps make the diagnosis of thrombosis and offers important clinical information (see Images 35-38). Tumors of the cervical region may surround the CCA or the ICAs. One of the advantages of cross -sectional imaging, such as CTA, is the identification of the tissues that surround the carotid and vertebral arteries. Degree of Confidence Carotid CTA represents a reliable means of estimating the degree of stenosis in both extracranial and intracranial vessels. Limitations in the degree of confidence are related to technical factors. Current multisection CT scanners allow for the acquisition of up to 16 sections for each gantry rotation. Each rotation may require as little as 0.4 seconds. Axial collimation for cervical-cerebral CTA is performed by using a collimation of 0.75 mm with a reconstruction of 1.5 mm for each axial image. Axial images, multiplanar reformatted images, and 3D volume MIP and volume-model images contribute to the sensitivity and accuracy of multisection CTA. By using available multisection CT scanners, extracranial carotid stenosis can be diagnosed to a degree of accuracy equal to or exceeding that of catheter-based angiography. CT offers an excellent means of detecting a tumor that might surround the carotid artery in the neck. When the carotid artery is imaged by using CTA, artifacts include motion, poor cardiac function, and dense carotid calcification. Overall accuracy for carotid CTA exceeds 95%. Intracranial CTA with a multisection scanner reportedly helps in identifying intracranial carotid stenosis with a sensitivity of greater than 98%, a specificity of 99%, and an accuracy of greater than 98%. Multisection CT scanners have been introduced that acquire 8 scans with each gantry rotation. With this newest technology, CTA represents the best overall means with which to investigate carotid stenosis in a less invasive and more cost-effective manner. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 18. View Carotid Artery, Stenosis Page 18 of 54 False Positives/Negatives False-positive results of carotid CTA are related to motion artifacts. Sudden movement, breathing, or swallowing by the patient during scanning may result in a misregistration of the axial images on 3D or multiplanar reformatted images. In such cases, only measurements taken from the axial images should be considered. False-negative results may occur if the vessels of the carotid bulb are very dilated and torturous. Superimposed jugular veins and arteries may hide a stenosis (see Image 21). A careful review of axial images, together with carefully performed curved multiplanar reformatted images through the carotid lumen, demonstrate the stenotic area in most patients. MRI Oblique 3-dimensional contrast-enhanced magnetic resonance (MR) angiogram of the aortic arch and brachiocephalic vessels shows high-grade stenosis of the proximal left subclavian artery (white arrow). By using such a model, full depiction of the arch, brachiocephalic vessels, and carotid bulbs is possible. Because of superimposed structures, full rotation of the arterial model is necessary. Note the left common carotid artery (LCCA) behind the left jugular vein. The left subclavian artery (LSCA) is seen well (blue arrow). Axial T1-weighted echo-planar diffusion image in a patient with high-grade internal carotid stenosis. Arrows point to multiple, small, subacute cerebral infarcts that have resulted from left internal carotid artery stenosis. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 19. View Carotid Artery, Stenosis Page 19 of 54 Carotid MR angiogram demonstrates very high-grade stenosis (arrow) in the proximal internal carotid artery in a patient with a recent onset of stroke. Axial T1-weighted diffusion MRI demonstrates 3 subacute infarcts (arrows) in the medial parietal aspect of the brain in a patient known to have a very high-grade proximal stenosis of the right internal carotid artery. Magnetic resonance (MR) angiograms of the cervical vessels and the circle of Willis show marked narrowing of the internal carotid artery (arrow). Flow is nearly absent in the right intracranial internal carotid artery and in the M1 segment of the right middle cerebral artery. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 20. View Carotid Artery, Stenosis Page 20 of 54 Carotid artery stenosis. Axial 3-dimensional maximum intensity magnetic resonance (MR) angiogram in a patient with bilateral carotid artery occlusion. Note the absence of flow in the intracranial internal carotid arteries (yellow arrows). The remaining blood flow to the cerebral hemispheres is the result of collateral branches of the vertebral arteries, including the posterior communicating arteries (white arrows). Findings MRA usually is performed by using 2 primary methods, ie, time-of-flight and ultrashort T1- weighted imaging. Time-of-flight imaging is performed without intravenous contrast agent by using a spoiled gradient-echo sequence. The images are displayed with a MIP protocol in multiple projections. Contrast-enhanced MRA is performed by using a timed and rapid injection of a gadolinium-based contrast, such as gadolinium dimeglumine. Because the volume of contrast agent is limited to 15-20 mL in most cases, timing of the contrast agent bolus and good venous access are essential. The images are obtained by using a short recovery time (TR), short echo time (TE), and T1-weighted technique (TR/TE/flip angle, 4.9/2.4/35°). The images are displayed 11 in multiple projections by using an MIP technique. A 3D time-of-flight image of the carotid artery or a contrast-enhanced short-TE short-TR image is interpreted in much the same manner as CTAs or carotid angiograms of the same area. The stenotic area of the ICA should be evaluated according to the NASCET criteria. Because of the effects of turbulence, 3D time-of-flight imaging tends to cause overestimation of high-grade stenoses. In some cases, an area of discontinuity may be generated in the area of the stenosis. This results from turbulent blood flow patterns at the point of a high-grade stenosis and within very stenotic longer stenoses. The results of contrast-enhanced MRA are closely correlated with angiographic and operative findings. Gadolinium-based contrast agent has the effect of shortening the T1 qualities of the blood flowing through the stenosis (see Images 12-13, Image 27). Residual lumen is displayed with high signal intensity. High-grade stenosis tends to remain an attenuated but visible 12 lumen. Results of contrast-enhanced MRA are usually better than those of 3D time-of-flight imaging. Recent advances in contrast-enhanced MRA allow for improved imaging speed without the need for temporal interpolation. Time-resolved contrast-enhanced carotid MRA with a sensitivity- encoding (SENSE) reconstruction technique enables visualization of the carotid artery without superimposed venous structures. The early identification of stroke in the vascular distribution of a related carotid stenosis helps in focusing on an ipsilateral carotid lesion. T1-weighted diffusion-based imaging effectively depicts focal cerebral ischemia (see Image 28), and the finding is often correlated with a proximal carotid stenosis (see Image 27, Image 30). In other cases, intracranial MRA demonstrates no flow pattern, confirming carotid thrombosis (see Image 36). http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 21. View Carotid Artery, Stenosis Page 21 of 54 Gadolinium-based contrast agents (gadopentetate dimeglumine [Magnevist], gadobenate dimeglumine [MultiHance], gadodiamide [Omniscan], gadoversetamide [OptiMARK], gadoteridol [ProHance]) have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). For more information, see the eMedicine topic Nephrogenic Fibrosing Dermopathy. The disease has occurred in patients with moderate to end- stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness. For more information, see the FDA Public Health Advisory or Medscape. Degree of Confidence Both systematic and random errors affect the results of cerebrovascular MRA. Systematic errors are primarily the result of artifacts and are related to 3D time-of-flight imaging. Areas within the carotid artery that generate turbulence may develop a recirculating pattern of blood flow. In the returning blood flow, the lumen is recorded as artifactually narrowed. Short-segment occlusions may be suggested in patients with very high-grade stenosis (>85% stenosis). Time-of-flight MRA results should be reported in a manner similar to those of carotid duplex sonography. Although measurements obtained by using the NASCET criteria should be attempted, the significance of the recorded stenosis should be reported with caution. Random errors may occur when measurements of the internal lumen are made mechanically. Measuring from enlarged images reduces the relative degree of random error. MRA results obtained by using a very short-TR, short-TE, gadolinium-enhanced, timed bolus technique can be interpreted in much the same manner as those of carotid angiography and CTA. Intracranial MRA has a sensitivity of 92-95%, a specificity of 91%, and an overall accuracy of 91% in the detection of intracranial carotid stenosis. False Positives/Negatives Certain variations of the CCA may be difficult to interpret by using MRA findings. Narrow bands of intimal thickening may result in a high degree of stenosis; however, the central luminal narrowing is difficult to demonstrate on MRA examination. The proximal ICA may become folded or kinked. Such a kink generates turbulence just beyond the fold. A short-segment pseudo- occlusion may be seen on a time-of-flight study. The ectatic appearance of fibromuscular hyperplasia may be difficult to resolve by using time-of-flight imaging alone. The spasm of migraine can simulate carotid dissection on MRA studies performed during an acute migraine event. Assessment of the proximal carotid artery near its origin from the aortic arch requires a good contrast bolus, breath-holding and, in general, good cooperation on the part of the patient. False-negative carotid MRA results are primarily the result of limitations of resolution. Small surface ulcers may not be resolved on MRA images. At other times, deeper ulcers may contain blood clots, which reduce the apparent size of some ulcers. Ultrasound Findings B-mode ultrasonography http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 22. View Carotid Artery, Stenosis Page 22 of 54 The earliest manifestation of carotid vascular disease is characterized by increased arterial intimal-medial thickness. The normal range for combined intimal-medial thickness of the CCA has been reported to vary with age, up to a maximum thickness of 0.8 mm. Incremental increased thickening of the carotid intima is associated with increased risk of cerebral ischemic events, coronary ischemia, and first-time MI. Treatment with lipid-lowering drugs has been shown to decrease the intimal thickness of the carotid artery. Decrease in the thickness of the intima of the CCA has been correlated directly with successful treatment with drugs that lower serum low-density lipoprotein levels. The sonographic characteristics of symptomatic and asymptomatic carotid plaques are different. Symptomatic plaques are more likely to be hypoechoic and highly stenotic while asymptomatic plaques are hyperechoic and moderately stenotic. Evaluation of the surface of the plaque has not been demonstrated to be a satisfactory index of plaque instability. After carotid endarterectomy, intimal thickness varies in the surgical site. The thickness of the neointima has been correlated with carotid wall stiffness and restenosis after carotid surgery. Comparison of current carotid sonographic velocities to those obtained before carotid endarterectomy is important. In general, the velocity of flow should become reduced with successful surgery. However, velocities may remain elevated after surgery due to scar formation, which results in carotid wall stiffness. Restenosis may occur as a result of surgery or generalized atherosclerotic vascular disease. Doppler ultrasonography 13 Doppler ultrasonography is the primary noninvasive test for evaluating carotid stenosis. Primary examination of the carotid plaque is somewhat subjective because terms such as soft plaque or irregular surface are often used to describe the primary sonographic images. The degree of stenosis is better measured on the basis of the waveform and spectral analysis of the CCA and its major branches, especially the ICA. As an example, consider the following case history. A 70-year-old man presented with a suspected stroke. Symptoms included right-sided hemiparesis and dysphasia. Duplex ultrasound findings revealed a significant stenosis of the proximal left ICA (see Images 14-15). The image showed mostly soft echogenic plaque protruding from the posterior aspect of the bulb and origin of the ICA. A fairly narrow residual lumen remained. Spectral Doppler imaging confirmed the high-grade stenosis, with peak systolic velocity of 325 cm/s and diastolic velocity of 105 cm/s. In the author's laboratory, a diastolic cutoff of 90cm/s is used to distinguish 60-79% from 80-99% lesions in patients such as this man. Carotid Artery, Stenosis. Duplex carotid sonography in a patient with sudden onset of aphasia. The images are taken from the common carotid artery. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 23. View Carotid Artery, Stenosis Page 23 of 54 Carotid Artery, Stenosis. Duplex sonographic image take from the common carotid bulb several hours following the sudden onset of aphasia. Note the blunted flow in the distal ICA compatible with the high-grade proximal obstruction. The CCA shows narrowing of approximately 40%. The opposite ICA was only mildly narrowed and demonstrated normal findings on spectral Doppler examination. The patient underwent carotid angiography. Angiographic findings helped confirm an 80% ICA stenosis. The patient was eventually treated with carotid endarterectomy. Follow-up studies in the author's laboratory (not shown) demonstrated a fully patent ICA. Some residual hemiparesis has remained on the right side, but the patient is much improved from his status after the initial stroke. Many published lists exist of carotid flow velocities, which are associated with a graduated degree of stenosis. A listing of flow velocity/carotid stenosis criteria used in the author's department is shown in the Table below. Carotid Stenosis Criteria Peak Systolic Peak End Diastolic Peak Systolic Stenosis Velocity (cm/s) Velocity (cm/s) Velocity Ratio <50 <150 <50 <2.0 50-59 150-200 50-70 2.0-2.5 60-69 200-250 50-70 2.5-3.0 70-79 250-325 70-90 3.0-3.5 80-89 325-400 70-100 3.5-4.0 90-99 >400 >100 >4.0 Occlusion Not applicable Not applicable Not applicable Doppler ultrasonographic findings associated with stenosis include the following: • Ipsilateral CCA-to-ICA flow ratios may not be valid in the setting of contralateral ICA occlusion. • CCA waveforms may have a high-resistance configuration in ipsilateral ICA lesions. • ICA waveforms may have a high-resistance configuration in ipsilateral distal ICA lesions. • ICA waveforms may be dampened in ipsilateral CCA lesions. • Long-segment ICA stenosis may not have high end-diastolic velocity. • Velocities supersede imaging in grading stenosis. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 24. View Carotid Artery, Stenosis Page 24 of 54 • Imaging can be used to downgrade stenosis in the setting of turbulence caused by kinking. In addition to the typical evaluation of the flow rate in the proximal ICA, it has been shown that the flow directly within the ophthalmic artery is highly specific for severe carotid stenosis. Transcranial Doppler ultrasonography Transcranial Doppler imaging is both sensitive and specific in the detection of intracranial ICA stenosis that is hemodynamically significant. By using a mean flow velocity of 100 cm/s, transcranial Doppler images help in identifying most intracranial stenotic lesions, with good specificity. Degree of Confidence The success of duplex sonography depends on careful technique. Results vary somewhat among laboratories. The author's practice has chosen to base its results on a composite mix of the published results comparing the degree of proven stenosis versus flow velocity and ICA-to-CCA velocity ratios. Results should be reported in the context of established criteria as a percentage of stenosis. The Table, above, represents the criteria used in the author's practice. The results should be confirmed with carotid CTA or carotid MRA before surgery. Discovery of a reversed direction of flow in the ophthalmic artery is closely associated with high- grade ipsilateral ICA stenosis, with a sensitivity of 55%, a specificity of 100%, a negative predictive value of 82%, and a positive predictive value of 100%. Transcranial duplex sonography with a threshold of 100 cm/s helps in identifying hemodynamically significant lesions, with a sensitivity of 93.9% and a specificity of 91.2%. False Positives/Negatives Use of duplex sonography is not valid in the setting of contralateral ICA occlusion. CCA waveforms may have a high-resistance configuration with ipsilateral ICA lesions. ICA waveforms may have a high-resistance configuration with ipsilateral distal ICA lesions. ICA waveforms may be dampened with ipsilateral CCA lesions. Long-segment ICA stenosis may not have high end- diastolic velocity. Velocities supersede imaging in grading stenosis. Imaging can be used to downgrade stenosis in the setting of turbulence caused by kinking. After carotid surgery, recorded flow velocities may be elevated more than those recorded during preoperative examinations. Comparison of the results of the current examination to those of a prior study is essential. Nuclear Medicine Findings Single photon emission CT (SPECT) and positron emission tomography (PET) of the brain may 14, 15 demonstrate areas of cerebral ischemia versus areas of complete cerebral infarction. However, these studies provide only indirect imaging information related to carotid stenosis. By using a dynamic imaging method, an assessment of the inflow of technetium Tc 99m hexamethylpropylamine oxime (HMPAO) can be used to estimate the hemispheric cerebral blood flow. If such an assay is combined with a provocative challenge with acetazolamide, it is possible to differentiate patients with migraine from patients with an irreversible cerebral ischemia. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 25. View Carotid Artery, Stenosis Page 25 of 54 Degree of Confidence SPECT and PET of the brain both demonstrate cerebral infarction, which may indicate a related carotid stenosis. An acetazolamide challenge can successfully differentiate certain subclasses of cerebral ischemic syndromes, but all such studies provide indirect evidence of carotid stenosis. False Positives/Negatives False-positive results may occur as a result of confusion in the findings between an infarct of the brain and a low-grade brain neoplasm or abscess. In the evaluation of stroke, false-negative findings may occur in small areas of infarction, which may be below the resolution of a nuclear examination. Comparison with other studies (such as CT or MRI), which have higher resolution, is recommended. Angiography Thoracic arch angiography demonstrates one of the common variants of normal aortic arch (AA) development in which both the innominate artery (IA) and the left carotid artery share a common origin. The right common carotid artery (RCA) and the right internal carotid artery are irregular and narrowed. The long, multisegment areas of stenosis are believed to result from the effects of radiation therapy to the right side of the neck in this patient. Effects of radiation therapy are related to adverse effects on the vascular supply to the carotid or vertebral artery in the radiation field. Oblique lateral cervical arteriogram displayed by using a subtraction technique. Although the contrast agent was injected into the arch, both the carotid stenosis (arrows) and the carotid ulcerations (arrowheads) are demonstrated. ICA = internal carotid artery http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 26. View Carotid Artery, Stenosis Page 26 of 54 Oblique lateral cervical angiogram obtained by using an injection into the aortic arch. Although a very high-grade right internal carotid stenosis is depicted (rc), superimposition of the jugular vein (v) makes its evaluation difficult. Selective common carotid angiography has the advantage of fewer superimposed vessels. lc = left carotid. Common carotid angiogram shows normal findings. Note the slightly dilated shape of the distal common carotid artery and the proximal internal carotid artery (carotid bulb). ec = external carotid artery; f = facial artery; l = lingual artery; ic = internal carotid artery; im = internal maxillary artery; o = occipital artery; p cer = posterior cerebral artery; p com = posterior communicating artery Lateral selective right common carotid arteriogram. Only the proximal few centimeters of the internal carotid artery are patent (arrow). Selective catheterizations in the performance of carotid angiography provide higher resolution (smaller field of view), high concentrations of intraluminal contrast agent, and extended angiographic imaging (longer runs of images). The almost occluded internal carotid artery is evaluated better by using selective common carotid angiography. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 27. View Carotid Artery, Stenosis Page 27 of 54 Lateral common carotid arteriogram in a patient with a neck bruit. Note the focal narrowing of the proximal internal carotid artery (arrow). In severe cases, the kink may require carotid artery reconstruction. Anterior left common carotid arteriogram in a patient who presented with a loud left neck bruit. Note the horizontal line (arrow) in the proximal internal carotid artery, which represents a focal folding of the carotid artery. This configuration has been termed a kink. The bruit results from the turbulent blood flow through the focal narrowing. Lateral common carotid arteriogram in a patient with transient ischemic attacks. A small filling defect is noted in the common carotid bulb (arrow). A small blood clot was found at surgery, with intimal ulceration at the base of the clot. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 28. View Carotid Artery, Stenosis Page 28 of 54 Lateral angiogram of the internal carotid artery (ICA) in a patient with a prior complete occlusion of the internal carotid artery. The irregular lumen (arrows) is consistent with recanalization of the thrombosis. Lateral carotid angiogram in a patient who had a recent transient ischemic attack. Note the multiple areas of deep ulceration in the proximal internal carotid artery and carotid bulb (arrows). Lateral common carotid angiography demonstrates collateral vessels that form after a long-standing complete occlusion of the internal carotid artery. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 29. View Carotid Artery, Stenosis Page 29 of 54 CT and CT angiography in a patient with a load left neck bruit and symptoms of a transient ischemic attack. A, CT scan demonstrates that the left jugular vein (LJV) is superimposed on the left common carotid artery (LCCA). B, After electronic removal of the superficial left jugular vein, a high-grade stenosis of the origin of the left external carotid artery (LECA) is demonstrated clearly. Dense calcifications are seen (red arrows) near the origins of both the left external carotid artery and the carotid bulb. The left internal carotid artery is not significantly stenotic. Lateral common carotid angiogram shows appropriate measurements (arrows) for calculating the degree of stenosis by using the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria. Oblique multiplanar reformatted CT angiogram demonstrates a mild degree of stenosis in the proximal right internal carotid artery (RICA). RJV = right jugular vein. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 30. View Carotid Artery, Stenosis Page 30 of 54 Maximum intensity CT angiogram demonstrates mild bilateral carotid stenosis. L = left, R = right. Common carotid arteriogram demonstrates dilatation (black double arrow) of the internal carotid artery beyond the high-grade stenosis (white arrow). This poststenotic dilatation is associated with hemodynamically significant stenosis. Lateral carotid angiogram shows that the cervical carotid artery (CCA) is narrowed, but it has a smooth outline. The supraclinoid internal carotid artery (ICA) is occluded. Note the enlarged ophthalmic artery (Opthal A.), which functions as a major collateral. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 31. View Carotid Artery, Stenosis Page 31 of 54 Anteroposterior intracranial carotid angiogram shows absence of the normal middle cerebral arterial branches. Image also shows incomplete occlusion of the suprasellar internal carotid artery near the origin of the M1 segment of the right middle cerebral artery. Angiogram of the carotid artery near the skull base in a patient with a significant fracture of the skull base. Internal carotid artery compression and focal spasm is due to hemorrhage resulting from a pseudoaneurysm (arrow) of the upper cervical internal carotid artery. Treatment of this stenosis requires vascular control of the proximal and distal carotid artery. In this case, the stenosis is primary spasm, which might be considered a protective response to direct carotid artery injury. Findings Carotid angiography via a catheter injection of contrast agent is considered the standard of diagnostic imaging of the cervical and intracranial carotid arteries against which other techniques are often judged (see Image 5). The NASCET study was based on images created during catheter angiography. The diameters of stenosis can be measured directly. Luminal diameter ratios can be expressed. All contrast-enhanced angiographic studies depend on the radiographic density of iodinated contrast agent compared with normal blood and the density of the wall of the carotid artery (see Image 2-4, Image 6). Lesions may be smooth, irregular, or focal, or they may involve a long segment (see Image 2). Angiographic technique In the author's institution, all cervical-cerebral angiography is performed by using the Seldinger technique. The procedure initially involves entering the lumen of the artery of access with a needle. The femoral artery is used as access in most cases, while the axillary arteries may be entered as an alternative. A heparin-coated guide wire is passed through the hub of the needle into the lumen of the artery. Often a J-shaped guide wire is used initially to avoid intimal trauma. A 4F pigtail catheter is generally introduced over the guidewire into the ascending aortic arch. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 32. View Carotid Artery, Stenosis Page 32 of 54 Nonionic contrast (320 mg/mL of organically bound iodine) is injected at a rate of 20-25 mL for a total volume of 40-50 mL. The left anterior oblique projection is most common. If imaging is performed by using a digitally subtracted technique, less contrast material is needed. After the shape, smoothness, and patency of the proximal right CCA, the right subclavian artery, the left CCA, and the left subclavian artery are inspected, a catheter is selected to assist in the selective catheterization of the right CCA, the left CCA, and either or both of the vertebral arteries. A 0.035-in guidewire with a soft, straight tip is used to exchange the pigtail catheter for either a simple angle-tip catheter (eg, one with an HN1 shape) or one with a more complex hook or short-radius, curved shape. The guidewire chosen for the exchange may have a variable degree of flexibility in the distal several centimeters near the tip. With the guidewire leading into the proximal right and left CCA origins, the cerebral-shaped catheter is positioned in the CCAs below the carotid bulb. Vertebral injections are performed with the catheter in the vertebral artery near the origin of the vertebral artery to avoid spasm. After a small test injection is disinterred to verify the location and security of the catheter tip position, each of the carotid arterial circulations is studied. Images in a 30° ipsilateral left anterior oblique or right anterior oblique projection are obtained to clearly outline the carotid bifurcations. In some cases, the lateral and the anterior projections are needed. DSA performed by using a C-arm imager permits an optimal degree of rotation based on the patient's anatomic form. Imaging should include the intracranial carotid circulation in most cases. Selective catheterization of 1 or both vertebral arteries should be performed if clinically indicated in patients with vertebral basilar symptoms. Each injection of contrast agent into the CCA is given at a rate of 6-7 mL/s for a total volume of 10-12 mL depending on the estimated flow rate in the CCA. Selective vertebral artery angiography is generally performed by using an injection rate of 4-5 mL/s for a total volume of 6 -8 mL. Somewhat less contrast agent is needed if DSA imaging techniques are applied. The degree to which intracranial arteries beyond the ICA-MCA trifurcation must be studied should be based on an understanding of the patient's clinical presentation and symptoms. Collateral circulation is best understood by having full visualization of the intracranial circulation as well as the aortic arch and cervical carotid circulations. Measurements and other findings The most common method used to express measurements of the carotid artery is the NASCET criteria, which state that a percentage of stenosis is expressed as a factor of 100, ie, the diameter of the normal ICA located above the carotid bulb divided by the diameter of the proximal ICA at the narrowest point (see Images 22-23). Special consideration must be given for critical degrees of stenosis, often termed the string sign (see Image 4Image 6). The presence of contrast agent in a markedly restricted lumen may be an indication of a critical proximal focal stenosis or longer segmental narrowing. Depiction of residual intracranial arterial flow helps establish patency (see Images 31-32). Other findings noted on carotid angiography include calcification, ulceration (see Image 11), fibromuscular hyperplasia, carotid kinking or folding (see Images 7-8), focal thrombus formation (see Image 9), and intimal dissection. The plaque may become complicated by marked intimal thickening or subintimal hemorrhage (see Images 17-18). After a carotid thrombosis form, extensive collateralization patterns may be demonstrated (see Image 19), or partial recanalization may occur, resulting in a complex pattern of alternating narrowing and dilatation (see Image 10). http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 33. View Carotid Artery, Stenosis Page 33 of 54 Degree of Confidence Findings on catheter-contrast angiography of the carotid artery are accurate if measurements and calculation of the degree of stenosis are made carefully by using an enlarged image. Both systematic and random errors may occur during stenosis measurement. The calculation of the degree of stenosis should be based on the NASCET criteria if possible. Catheter-based angiographic studies remain the most accurate means of assessment of the degree of carotid stenosis. False Positives/Negatives False-positive examinations may occur if injection of the contrast agent is not timed properly, resulting in a washed-out appearance on the image. If subtracted images are developed, overlying metal or dense calcifications result in shadowing of some of the plaque-artery lumen, making an accurate measurement of the residual lumen difficult. Movement, coughing, and the presence of metal artifacts may prevent an accurate examination. Rapid injection may cause a standing wave to form, which may appear similar to fibromuscular hyperplasia. False-negative results may occur if a nonselective angiographic technique is used (see Images 3- 4). Superimposition of other arterial and venous structures may prevent adequate depiction or measurement of the stenosis. Despite technical limitations, catheter-based angiography remains the criterion standard against which other imaging techniques are compared. Intervention Intervention in patients with acute CVA is usually based on an attempt to relieve the intracranial thrombosis or an embolization by using thrombolytic agents. The success of such treatment depends on early intervention (during the first 4 h) after the onset of the ischemic event. With the demonstration of a thrombosis by using perfusion CT or perfusion-diffusion MRI techniques, catheter-directed thrombolytic therapy may be administered by using recombinant tissue-type plasminogen activator (rTPA) or another thrombolytic agent. The success of this therapy remains controversial and is the subject of ongoing research. Another important area of primary intervention is the treatment of ICA stenosis by using an endovascular stent across the stenotic vessel segment. This treatment results in improved vascular flow rates across the stenotic segment. Suboptimal anatomic results have been reported with the use of the self-expanding Wallstent in this application. Restenosis and recurrent cerebral embolization have been reported following endovascular treatment of carotid stenosis. The increased application of carotid stent placement can be expected to preserve the role of catheter-based cervical-cerebral carotid catheter angiography. Recent study The use of intravenous tissue plasminogen activator (t-PA) for stroke 3-4.5 hours after symptoms has been recommended by the American Heart Association, although time to treatment remains of extreme importance and should not be delayed. The European Cooperative Acute Stroke Study 3 (ECASS 3) showed benefit from t-PA in patients treated 3-4.5 hours after onset of symptoms of stroke.31, 32, 33, 34 Medical/Legal Pitfalls http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 34. View Carotid Artery, Stenosis Page 34 of 54 • Use of interventional therapies in the treatment of acute CVA and carotid stenosis represents complex clinical decision making, which is subject to alternative interpretations of what constitutes a good standard of care. ◦ Patients with acute cerebral infarct may have significant morbidity if a large infarction is not corrected on an emergency basis, whereas thrombolytic therapy (intra-arterial or intravenous) may result in fatal intracerebral hemorrhage. ◦ The benefits of interventional treatment of patients with carotid stenosis must compare favorably with those of conventional surgery of the carotid artery to avoid medical/legal challenges. ◦ Interventional therapies, including angioplasty and angioplasty with stent placement, may result in a hyperperfusion syndrome. ◦ Hemorrhage can occur within the zone of hyperperfusion. ◦ Preoperative CT scans and MRIs of the brain must be used to exclude focal hemorrhage. ◦ Hyperperfusion syndrome has also been described after angioplasty of an MCA stenosis. See also the Medscape topic Medical Malpractice and Legal Issues. Special Concerns Test Questions Question 1: Which of the following statements regarding time-of-flight magnetic resonance angiography (MRA) of the carotid artery is true? A. The findings tend to underestimate the degree of stenosis. B. The findings are somewhat less accurate than those of conventional angiography. Calcification of the carotid arterial bulb adversely affects the results in the same way that C. dense calcifications degrade carotid duplex sonography. D. Time-of-flight MRA requires the use of intravenous contrast agent. Compared with contrast-enhanced MRA, time-of-flight MRA provides more accurate results E. in the proximal neck and near the origins of the innominate, subclavian, and common carotid arteries. The correct answer is B: Although 3-dimensional time-of-flight MRA is often successful, the degree of stenosis tends to be overestimated in high-grade stenosis and carotid lesions that generate significant turbulence. These limitations may result in an apparent vascular thrombosis in areas of extreme narrowing. Time-of-flight images are obtained without the use of intravenous gadolinium-based contrast agent. As a result of the higher resolution of the angiogram, catheter- based angiography improves imaging in most patients; however, CT angiography and MRA findings are fully diagnostic in most clinical settings. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 35. View Carotid Artery, Stenosis Page 35 of 54 Question 2: Which of the following risk factors in not found in patients with carotid artery stenosis? A. Poorly managed hypertension B. A diet rich in saturated fat C. High doses of radiation to the neck, as in cancer therapy D. Poorly managed diabetes E. High levels of high-density lipoprotein The correct answer is E: In addition to the common risk factors for carotid artery and coronary arterial stenosis (eg, poorly managed hypertension and diabetes and saturated fat in the diet), radiation to the neck causes severe and premature vascular disease to develop within the irradiated vessels. Levels of high-density lipoprotein (good cholesterol) are usually low. Question 1 (T/F): The degree of stenosis that requires surgery is 60% in young patients, as measured according to the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria. The correct answer is False: The results of the NASCET studies have supported endarterectomy for asymptomatic patients with a stenosis greater than 70%. Surgery is indicated for symptomatic patients with a stenosis of 60% or greater. Question 2 (T/F): Densely calcified carotid stenosis makes it difficult to accurately measure the lumen with CT angiography (CTA); therefore, magnetic resonance angiographic (MRA) findings are interpreted more easily in patients with this condition. The correct answer is True: Time-of-flight MRA findings are less affected by dense calcifications than those of angiography or CTA. Question 3 (T/F): Carotid duplex sonography is more accurate in patients with severe stenosis of the internal carotid artery than in those with less stenosis. The correct answer is False: Very high-grade stenosis may appear as a complete occlusion. The results of duplex sonography are reported in ranges of stenosis based primarily on peak velocity of flowing blood measured in the proximal internal carotid artery during systole. Question 4 (T/F): After carotid surgery, the peak systolic velocity may remain slightly elevated in the absence of recurrent stenosis. The correct answer is True: After otherwise successful carotid endarterectomy, peak systolic velocities may remain above normal values. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 36. View Carotid Artery, Stenosis Page 36 of 54 Further Reading Clinical guidelines Acute stroke management. Carotid artery imaging. In: Canadian best practice recommendations for stroke care: 2006. Canadian Stroke Network - Disease Specific Society Heart and Stroke Foundation of Canada - Disease Specific Society. 2006. 2 pages. [NGC Update Pending] NGC:006262 Screening for carotid artery stenosis: U.S. Preventive Services Task Force recommendation statement. United States Preventive Services Task Force - Independent Expert Panel. 1996 (revised 2007). 6 pages. NGC:005970 Antithrombotic therapy for peripheral artery occlusive disease. American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). American College of Chest Physicians - Medical Specialty Society. 2001 Jan (revised 2008 Jun). 29 pages. NGC:006669 Clinical trials Comparing Carotid Stenting With Endarterectomy in Severe Asymptomatic Carotid Stenosis Stenting Versus Best Medical Treatment of Asymptomatic High Grade Carotid Artery Stenosis Cost-Effectiveness of a Specialized Ultrasound Instrument to Diagnose Carotid Stenosis as a Way to Reduce the Risk of Stroke Related eMedicine topics Carotid Ultrasound Atherosclerotic Disease of the Carotid Artery Stroke, Ischemic Aortoiliac Occlusive Disease MULTIMEDIA Media file 1: Four of the most common methods of imaging the carotid artery are compared. Angio = angiography, CTA = CT angiography, Duplex = duplex ultrasonography, Gd = gadolinium enhancement, ICA = internal carotid artery, MRA = magnetic resonance angiography, TOF = time of flight. Media type: Image http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 37. View Carotid Artery, Stenosis Page 37 of 54 Media file 2: Thoracic arch angiography demonstrates one of the common variants of normal aortic arch (AA) development in which both the innominate artery (IA) and the left carotid artery share a common origin. The right common carotid artery (RCA) and the right internal carotid artery are irregular and narrowed. The long, multisegment areas of stenosis are believed to result from the effects of radiation therapy to the right side of the neck in this patient. Effects of radiation therapy are related to adverse effects on the vascular supply to the carotid or vertebral artery in the radiation field. Media type: X-RAY Media file 3: Oblique lateral cervical arteriogram displayed by using a subtraction technique. Although the contrast agent was injected into the arch, both the carotid stenosis (arrows) and the carotid ulcerations (arrowheads) are demonstrated. ICA = internal carotid artery Media type: X-RAY Media file 4: Oblique lateral cervical angiogram obtained by using an injection into the aortic arch. Although a very high-grade right internal carotid stenosis is depicted (rc), superimposition of the jugular vein (v) makes its evaluation difficult. Selective common carotid angiography has the advantage of fewer superimposed vessels. lc = left carotid. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 38. View Carotid Artery, Stenosis Page 38 of 54 Media type: X-RAY Media file 5: Common carotid angiogram shows normal findings. Note the slightly dilated shape of the distal common carotid artery and the proximal internal carotid artery (carotid bulb). ec = external carotid artery; f = facial artery; l = lingual artery; ic = internal carotid artery; im = internal maxillary artery; o = occipital artery; p cer = posterior cerebral artery; p com = posterior communicating artery Media type: X-RAY Media file 6: Lateral selective right common carotid arteriogram. Only the proximal few centimeters of the internal carotid artery are patent (arrow). Selective catheterizations in the performance of carotid angiography provide higher resolution (smaller field of view), high concentrations of intraluminal contrast agent, and extended angiographic imaging (longer runs of images). The almost occluded internal carotid artery is evaluated better by using selective common carotid angiography. Media type: X-RAY Media file 7: Lateral common carotid arteriogram in a patient with a neck bruit. Note the focal narrowing of the proximal internal carotid artery (arrow). In severe cases, http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 39. View Carotid Artery, Stenosis Page 39 of 54 the kink may require carotid artery reconstruction. Media type: X-RAY Media file 8: Anterior left common carotid arteriogram in a patient who presented with a loud left neck bruit. Note the horizontal line (arrow) in the proximal internal carotid artery, which represents a focal folding of the carotid artery. This configuration has been termed a kink. The bruit results from the turbulent blood flow through the focal narrowing. Media type: X-RAY Media file 9: Lateral common carotid arteriogram in a patient with transient ischemic attacks. A small filling defect is noted in the common carotid bulb (arrow). A small blood clot was found at surgery, with intimal ulceration at the base of the clot. Media type: X-RAY Media file 10: Lateral angiogram of the internal carotid artery (ICA) in a patient with a prior complete occlusion of the internal carotid artery. The irregular lumen (arrows) is consistent with recanalization of the thrombosis. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 40. View Carotid Artery, Stenosis Page 40 of 54 Media type: X-RAY Media file 11: Lateral carotid angiogram in a patient who had a recent transient ischemic attack. Note the multiple areas of deep ulceration in the proximal internal carotid artery and carotid bulb (arrows). Media type: X-RAY Media file 12: Oblique magnetic resonance angiogram of the aortic arch and proximal subclavian and common carotid arteries in a patient who presented with dizziness, which was worsened by exercise. Blood pressure readings from each arm were of different in value, with the left arm blood pressure more than 20 mm Hg lower than that on the right side. High-grade stenosis of the proximal left subclavian artery is demonstrated (arrow). Media type: MRI Media file 13: Oblique 3-dimensional contrast-enhanced magnetic resonance (MR) angiogram of the aortic arch and brachiocephalic vessels shows high-grade stenosis of the proximal left subclavian artery (white arrow). By using such a model, full depiction of the arch, brachiocephalic vessels, and carotid bulbs is possible. Because of http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 41. View Carotid Artery, Stenosis Page 41 of 54 superimposed structures, full rotation of the arterial model is necessary. Note the left common carotid artery (LCCA) behind the left jugular vein. The left subclavian artery (LSCA) is seen well (blue arrow). Media type: MRI Media file 14: Carotid Artery, Stenosis. Axial CT of the brain in a patient with the sudden onset of aphasia. Media type: CT Media file 15: Carotid Artery, Stenosis. Duplex carotid sonography in a patient with sudden onset of aphasia. The images are taken from the common carotid artery. Media type: X-RAY Media file 16: Carotid Artery, Stenosis. Duplex sonographic image take from the common carotid bulb several hours following the sudden onset of aphasia. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 42. View Carotid Artery, Stenosis Page 42 of 54 Media type: X-RAY Media file 17: Carotid Artery, Stenosis. Proximal duplex sonography of the left ICA in a patient who presented with the sudden onset of aphasia. Media type: X-RAY Media file 18: Carotid Artery, Stenosis. Axial image of a carotid CTA in a patient with right sided weakness and sudden onset of aphasia. The left ICA (yellow arrow) is occluded. Media type: CT Media file 19: Carotid Artery, Stenosis. Sagittal MPR image from a carotid CTA in a patient with sudden onset of aphasia. The proximal left ICA demonstrates a short segment of complete occlusion with flow preserved in the more distal left ICA. The common carotid artery (CCA) has a normal diameter. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 43. View Carotid Artery, Stenosis Page 43 of 54 Media type: CT Media file 20: Carotid Artery, Stenosis. The anterior communicating artery (AComA) represents an important collateral circulation which preserves blood flow to the left middle cerebral artery (L MCA) in this patient with sudden onset of aphasia. The proximal left ICA was noted to be occluded on the CTA of the cervical carotid arteries. Media type: CT Media file 21: Carotid Artery, Stenosis. Duplex sonography of the external carotid artery in a patient who presented with the sudden onset of aphasia. Media type: X-RAY Media file 22: Longitudinal sonogram of a left internal carotid stenosis of the proximal internal carotid artery (Prox. ICA). The peak systolic velocity (PV) recorded from within the lumen of the proximal internal carotid artery was greater than 325 cm/s. Media type: Image Media file 23: Cross-sectional sonogram of a moderately high-grade stenosis of the left internal carotid artery (ICA). Longitudinal and axial images are helpful in identification http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 44. View Carotid Artery, Stenosis Page 44 of 54 of the branches of the internal carotid artery (I) versus those of the external carotid artery (E). Media type: CT Media file 24: Axial T1-weighted echo-planar diffusion image in a patient with high- grade internal carotid stenosis. Arrows point to multiple, small, subacute cerebral infarcts that have resulted from left internal carotid artery stenosis. Media type: MRI Media file 25: Lateral carotid angiogram shows a high-grade stenosis of the proximal internal carotid artery in comparison with a photograph of the plaque after endarterectomy. Media type: Image Media file 26: Intraoperative image obtained during carotid endarterectomy shows dissection of the plaque (black arrow). A bypass shunt (yellow arrow) allows blood to flow around the operative site, creating a bloodless surgical field without cross- clamping of the carotid artery. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 45. View Carotid Artery, Stenosis Page 45 of 54 Media type: Photo Media file 27: Lateral common carotid angiography demonstrates collateral vessels that form after a long-standing complete occlusion of the internal carotid artery. Media type: X-RAY Media file 28: Dense calcifications (arrows) of the common carotid bulb and proximal internal carotid artery. Calcifications such as these complicate assessment of the degree of internal carotid artery stenosis. Media type: CT Media file 29: CT and CT angiography in a patient with a load left neck bruit and symptoms of a transient ischemic attack. A, CT scan demonstrates that the left jugular vein (LJV) is superimposed on the left common carotid artery (LCCA). B, After electronic removal of the superficial left jugular vein, a high-grade stenosis of the origin of the left external carotid artery (LECA) is demonstrated clearly. Dense calcifications are seen (red arrows) near the origins of both the left external carotid artery and the carotid bulb. The left internal carotid artery is not significantly stenotic. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 46. View Carotid Artery, Stenosis Page 46 of 54 Media type: CT Media file 30: North American Symptomatic Carotid Endarterectomy Trial (NASCET) stenosis measurement. CCA = common carotid artery, D = narrowed diameter, ECA = external carotid artery, ICA = internal carotid artery, and N = normal diameter. Media type: Image Media file 31: Lateral common carotid angiogram shows appropriate measurements (arrows) for calculating the degree of stenosis by using the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria. Media type: X-RAY Media file 32: Oblique multiplanar reformatted CT angiogram demonstrates a mild degree of stenosis in the proximal right internal carotid artery (RICA). RJV = right jugular vein. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 47. View Carotid Artery, Stenosis Page 47 of 54 Media type: CT Media file 33: Maximum intensity CT angiogram demonstrates mild bilateral carotid stenosis. L = left, R = right. Media type: CT Media file 34: Common carotid arteriogram demonstrates dilatation (black double arrow) of the internal carotid artery beyond the high-grade stenosis (white arrow). This poststenotic dilatation is associated with hemodynamically significant stenosis. Media type: X-RAY Media file 35: Carotid MR angiogram demonstrates very high-grade stenosis (arrow) in the proximal internal carotid artery in a patient with a recent onset of stroke. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010
- 48. View Carotid Artery, Stenosis Page 48 of 54 Media type: MRI Media file 36: Axial T1-weighted diffusion MRI demonstrates 3 subacute infarcts (arrows) in the medial parietal aspect of the brain in a patient known to have a very high-grade proximal stenosis of the right internal carotid artery. Media type: MRI Media file 37: Even in the absence of a high-grade stenosis, carotid ulceration may result in cerebral infarct. Note the deep ulceration (arrow) demonstrated on this 3- dimensional volume image of the right carotid artery. The large vessel shown to the right is the right jugular vein (RJV). CCA = common carotid artery. Media type: CT Media file 38: Magnetic resonance (MR) angiograms of the cervical vessels and the circle of Willis show marked narrowing of the internal carotid artery (arrow). Flow is nearly absent in the right intracranial internal carotid artery and in the M1 segment of the right middle cerebral artery. http://progps1.emedicine.com/gps/displaytopic.gps?view=plain&docid=417524 5/4/2010