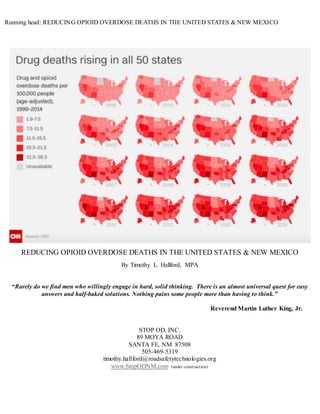
This document provides an analysis of opioid overdose deaths in the United States and New Mexico. It discusses the target populations of opioid abusers and overdose victims, noting that overdoses affect people across demographics, including those prescribed opioids for chronic pain. The document presents data on opioid prescribing rates in New Mexico, finding that approximately one in every New Mexican receives an opioid prescription each year. It argues that redirecting existing resources to widespread naloxone distribution could significantly reduce overdose deaths immediately. The goal is to keep those at risk of overdose alive so that prevention and treatment strategies may help them.
1. Running head: REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO
REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO
By Timothy L. Hallford, MPA
“Rarely do we find men who willingly engage in hard, solid thinking. There is an almost universal quest for easy
answers and half-baked solutions. Nothing pains some people more than having to think.”
Reverend Martin Luther King, Jr.
STOP OD, INC.
89 MOYA ROAD
SANTA FE, NM 87508
505-469-5319
timothy.hallford@roadsafetytechnologies.org
www.StopODNM.com (under construction)
2. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 2
2
TABLE OF CONTENTS
Abstract………………………………………………………………………………….. Page 3
Definitions/Organizations……………………………………………………………….. Page 4
Introduction ……………………………………………………………………………... Page 6
Target Population………………………………………………………………………… Page 8
Opioid Abusers…………………………………………………………………... Page 8
Opioid Overdose Citizens………………………………………………………... Page 10
Where are the Opioid Overdose Deaths?................................................................ Page 12
Synthetic Opioids & Fentanyl……………………………………………………. Page 22
Cost Benefit Analysis of Opioid Overdose Deaths……………………………………….. Page 28
Statewide Naloxone Distribution…………………………………………………………. Page 30
Naloxone Cost…………………………………………………………………….. Page 64
Naloxone Distribution Partners…………………………………………………… Page 68
What Should We Research & Study?................................................................................... Page 69
Critical Thinking & Analysis……………………………………………………………… Page 72
Findings……………………………………………………………………………………. Page 81
Strategic Action Plan………………………………………………………………………..Page 86
Editorial……………………………………………………………………………………. Page 89
References………………………………………………………………………………….. Page 94
About Timothy L. Hallford………………………………………………………………… Page 101
Appendix…………………………………………………………………………………… Page 102
4. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 4
4
Abstract
This paper’s premise is that opioid overdose deaths in the United States, and in New Mexico have not meaningfully
reduced despite all of the research, financial resources, organizations, campaigns, legislation, political statements, and
community participation efforts. In fact, this paper describes a microcosm of the macrocosm of the current situation of
opioid overdose deaths in the United States-in almost all communities, they are unfortunately increasing. This paper offers
a strategy that will reduce opioid overdose deaths almost immediately. It is a call to action, with the already plentiful
resources targeted for this epidemic, and while making it a real emergency priority as portrayed by our leadership.
Keywords: Opioid Overdose, Opioid Abuse, Overdose Deaths, Naloxone, NARCAN, Harm Reduction, New Mexico
(Please note: While this paper is at least partly, in APA style format, bold type words are mine, they are there for emphasis and importance,
please forgive me for the violation of the style.)
5. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 5
5
DEFINITIONS AND RELATED STATE AGENCIES:
1. Epidemic -affecting or tending to affect a disproportionately large number of individuals within a population,
community, or region at the same time.
2. Epidemiology - a branch of medical science that deals with the incidence, distribution, and control of disease in a
population; the sum of the factors controlling the presence or absence of a disease or pathogen
3. Naloxone -a potent synthetic antagonist of narcotic drugs (as morphine and fentanyl) that is administered
especially in the form of its hydrochloride C19H21NO4·HCl. Naloxone is typically administered by injection to
reverse the effects of opioids and especially in the emergency treatment of opioid overdose. It is also administered
in combination with buprenorphine in the form of a dissolvable tablet placed under the tongue or a film placed
inside the cheek to treat opioid dependence. Trademarks for preparations containing naloxone include Bunavail,
Evzio, Narcan, Suboxone, and Zubsolv.
4. Reversal – term used by the New Mexico Department of Health to mean that a citizen who is overdosing does not
die because of the use of the drug, Naloxone or other antagonist of narcotic drugs which revives them.
5. Emergency Declaration - Emergency clause, meaning the law takes effect immediately.
6. Opioid Overdose - Opioid overdoses happen when there are so many opioids or a combination of opioids and other
drugs in the body that the victim is not responsive to stimulation and/or breathing is inadequate. This happens because
opioids fit into specific receptors that also affect the drive to breathe. If someone cannot breathe or is not breathing
enough, the oxygen levels in the blood decrease and the lips and fingers turn blue- this is called cyanosis. This oxygen
starvation eventually stops other vital organs like the heart, then the brain. This leads to unconsciousne ss, coma, and
then death. Within 3-5 minutes without oxygen, brain damage starts to occur, soon followed by death. With opioid
overdoses, surviving or dying wholly depends on breathing and oxygen.
6. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 6
6
ORGANIZATIONS:
NEW MEXICO DEPARTMENT OF HEALTH
MissionStatement:
“Our mission is to promote health and wellness, improve health outcomes, and assure safety net services for all people in
New Mexico.”
Public Health Division:
“Coordinated system of community based public health services focusing on disease prevention and health promotion.”
Epidemiology & Response Division:
“Tracks infectiousdiseases,injuryandhealthstatistics,trainsorganizationsindisease control,injuryprevention,respondstopublic
healthemergenciesandprovidesvital recordsservices.We alsoissue 228,000 birthand deathcertificatesandregister28,000 births
and 14,000 deathseachyear.”
Environmental Health EpidemiologyBureau:
“Reduce the prevalence of environmentally-relatedadverse healthoutcomesby:
Conductingsurveillance of relevant,prioritizedhealthoutcome
Identifyingenvironmental exposuresof concern Implementingpublichealthpromotionthroughevidence-based
approaches
Evaluatingprogramactivitiestofurtherdevelopandimproveeffectiveness”
NEW MEXICO DEPARTMENT OF HUMAN SERVICES
MissionStatement:
“To reduce the impact of povertyonpeople livinginNew Mexicobyprovidingsupportservicesthathelpfamiliesbreakthe cycle of
dependencyonpublicassistance.”
Behavioral ServicesDivisionMission Statement:
“The Behavioral HealthServicesDivision(BHSD) primaryrole istoserve asthe Mental HealthandSubstance
Abuse State Authorityforthe State of NewMexico.The Authority'srole istoaddressneed,services,planning,
monitoringandcontinuousqualitysystemicallyacrossthe state.”
UNIVERSITYOF NEW MEXICO
Health SciencesCenterDivision:
“Our mission is to provide an opportunity for all New Mexicans to obtain an excellent education in the health sciences. We
will advance health sciences in the most important areas of human health with a focus on the priority health needs of our
communities. As a majority-minority state, our mission will ensure that all populations in New Mexico have access to the
highest quality health care. In order to realize our Vision and Mission, we will achieve the following goals:
Improve healthandhealthcare to the populationswe servewithcommunity-wide solutions
Buildthe workforce of NewMexicobyprovidingapremiereducationandtransformativeexperience thatprepares
studentstoexcel inthe workplace
Fosterinnovation,discoveryandcreativity;andtranslate ourresearchanddiscoveriesintoclinical oreducational practice;
7. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 7
7
Provide the environmentandresourcestoenable ourpeople andprogramstodo theirbest
Deliverawell-integratedacademichealthcenterthatprovideshighqualityof care andservice while beingaccessible toall
NewMexicans
Nurture andembrace an environmentof diversity,integrityandtransparency
Project Echo Program:
MissionStatement:
“ProjectECHO isa lifelonglearningandguidedpractice modelthatrevolutionizesmedical educationandexponentiallyincreases
workforce capacityto provide best-practice specialtycare andreduce healthdisparities.The heartof the ECHO model™
isitshub-
and-spoke knowledge-sharingnetworks,ledbyexpertteamswhouse multi-pointvideoconferencingtoconductvirtual clinicswith
communityproviders.Inthisway,primarycare doctors, nurses,andotherclinicianslearntoprovide excellentspecialtycare to
patientsintheirowncommunities.”
INTRODUCTION
New Mexico, consistently has always been at the top of the list for opioid overdose deaths in the United States,
currently #2 (although recent unclear data is indicating we are #9 for all overdose deaths), per capita. As it is in the United
States, it is a true epidemic. We, as a nation, and in New Mexico, were, and are still not ready, to focus ourselves on this
specific issue, marshaling the available resources to reduce this quite manageable problem. It’s actually been going on for
a long time in some parts of the United States, including New Mexico, and our government officials, law enforcement,
politicians, criminal justice, social services, treatment agencies, churches, and community organizations have
strategies in place. What has changed significantly, in the last 5 years, is that now it is epidemic everywhere in the
United States, across all age groups and races, in rural and metropolitan areas, in wealthy, middle class, and poor
communities, among the educated and the illiterate, among the young, adult, and elderly population. Substance
abuse has always been a huge challenge for policymakers, treatment agencies, the medical community, emergency services
personnel, law enforcement, judicial, social services and now suddenly they are asked to deal with this epidemic which has
reached its tentacles out into the whole United States. Frankly, it is unfair to ask them, by themselves, to now address
what was already a huge problem turned epidemic. I submit that, if it is affecting all states, all communities, all
Americans, then we all must stand up together to address it. My daughter, Ashley Seidner, D.O. is a physician in
residency at a hospital in Ohio, she reports that overdoses coming into the emergency room there are now routine. Ohio,
in the middle of the conservative Midwest, now leads the nation in overdose deaths:
8. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 8
8
Ohio leads the nation in deaths due to heroin and otheropioid overdoses.According to the Kaiser Family Foundation,the toll climbed from 2,106
in 2014 to 3,050 last year, with an even higher number projected for 2016. Ohio outpaces New York and California, states with much larger
populations… Epidemic is the fitting description, and state lawmakers, along with Gov. John Kasich, have responded with addit ional resources for
communities. The recent lame-duck session produced strongerregulations for opioid prescriptions, improved access to naloxone (medication to
reverse overdoses) and support for treatment programs… Ohio law gives the governor and lawmakers the authority to declare
emergencies. That is what the heroin and opioid epidemic presents. Will they respond adequately in the new year? {74}
While research (already completed en masse) on education, prevention, and treatment are critical factors to address the
problem, I submit that we must first address keeping opioid abuse citizens alive otherwise the rest of these strategies
mean nothing to that citizen for they are, needlessly, unfortunately already deceased. Several government agencies, even
the Governor’s office, have received significant federal funding to augment state resources for this expressed purpose.
This paper’s premise is that some, in fact, a relatively small amount of these financial resources, already available,
need to be redirected toward reducing opioid overdose deaths in New Mexico and exponentially in the United
States.
The Good News
There is good news about the possibilities of reducing opioid overdose deaths significantly in New Mexico. We
have the drug Naloxone, available to reverse immediately the citizen who is overdosing on opioids, no matter what the
reason – accidental overdose, illicit drug use, or suicide attempt. The cost of the drug is infinitesimal considering all the
available resources, the significant medical, legal, criminal justice, and societal costs of opioid overdose deaths, and the
cost to families, friends, emergency responders, doctors, hospitals, and innocent witnesses to an opioid overdose death.
And finally, the cost of deceased New Mexico citizen themselves-literally their life. New Mexico has garnered a great
deal of grant monies to address opioid abuse and overdose deaths. Federal and state resources are at multi-million dollars
each year, every year. And now there is even more with President Obama’s recent signature of the bill directing $1.8B
expressly for opioid drug abuse and overdose deaths. In New Mexico, we have passed and signed innovative legislation
that includes a standing order for the prescription of the drug Naloxone where it can be distributed by all pharmacies in
New Mexico without an individual prescription. We have a new Good Samaritan Law, passed in 2016 (which actually
already had one years before), signed by Governor Martinez, which provides that there can be no civil liability or criminal
9. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 9
9
penalties for any citizen administering Naloxone in good faith, to an overdosing citizen in New Mexico. We have at least
some supply (the number of which I cannot determine) of the drug Naloxone, currently under control of the New Mexico
Department of Health, which can be, and is, distributed to a small number of pharmacies in New Mexico and to some
community organizations and treatment centers. We even have some big pharmaceutical companies willing to donate for
free or at a reduced cost, Naloxone to our State. And yet we remain, #2 in the nation for overdose deaths. Why? Because
it time that we think critically now, analyze what we have done, are doing, efficiency and effectiveness, and what can be
done immediately to reduce this death rate epidemic. And we must do it now, for, as I write this paper, a few more New
Mexico citizens have died from an opioid overdose.
Target Population. So, who are we targeting in this mission? Any New Mexico citizen who may accidentally, abuse,
or purposely overdose on opioids-legal or illegal. There is a strong belief that most of these citizens are at the street
level, homeless, lifelong drug abusers, and for some, lost causes. And as if, somehow, their lives are worth less than those
who are not overdosing. If they were treated the same as any New Mexico citizen, then why are they still dying at the
same rate? Why aren’t more resources not dedicated towards stopping their deaths? And what if, let’s say, half of the
overdose citizens, get help for the problem, and change their lives. And maybe they then become Naloxone advocates
themselves, saving others like they were saved, exponentially, Suddenly, we have someone still alive saving at least one
more life in New Mexico. Are these “reversal citizens” worth it now? What do we know about opioid overdose citizens?
A plethora of data, studies, and presentations continue to say the same things:
Opioid abusers. The first population to consider is those who accidentally take too many opioids or choose to abuse
opioids but do not actually overdose. They are the potential overdose citizens. They are not just street level addicts, they
are people who may be in chronic pain, have an injury requiring opioids for pain, handicapped, elderly, etc. What do we
know about them? While I could not find demographics for New Mexico for all opioid users, including illicit users (except
for youth), here are the demographics for prescribed opioids by participating pharmacies in Department of Health
program (please note this was from a presentation in 2014 using data only through 2012) a small percentage of
pharmacies, less than 20% of the 300 pharmacies in New Mexico:
10. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 10
10
The age group for those filling prescription opioids is wide with the highest rate for New Mexicans age 85+. Males are
more prevalent than females. Significant usage begins at age 15 and increases in every age group through age 85+.
While this is eye opening, I still do not have more detailed demographics (race, location, prescribed reason, etc.) on
the legal use of opioids that I could find. Perhaps the answer is that opioid prescriptions are crossing all
demographics at an epidemic rate? I suspect the latter. Anyway, I digress… {1}
Total Opioid Prescribing in New Mexico:
Assuming there are approximately 2 million people in our state, this user group alone equals having one opioid
prescription for every New Mexican, men, women, and children. And this is similar to the national rate for America.
Of these citizens, above, it appears that the average number of opioid prescriptions prescribed is 2 prescriptions each.
And this is every year. So, we seemto have little problem getting opioids prescribed in New Mexico, how do we get
Naloxone in every New Mexican’s medicine cabinet?
Controlled Substance and Opioid Prescribing by Year and
Quarter
450,000
400,000
350,000
300,000
250,000
200,000
150,000
100,000
50,000
-
406,259 410,940 423,026
269,069 271,822 283,253
187,159 190,752 200,950
Total number of Controlled Substance patients
Number of patients receiving opioids
Number of opioid prescriptions filled (excluding buprenorphine/naloxone)
2015Q3 2015Q4 2016Q1 2016Q2 2016Q3
389,865 377,087
264,097 258,836
181,278 175,839
11. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 11
11
{75}
Opioid Overdose Citizens. Let’s look at the demographics for those who overdose, for there is no lack of research or data
in this data set in the United States and specifically, New Mexico:
“In NM, the rate of ED visits due to opioid overdose increased almost 30% between 2010 and 2013 The rate increased approximately 36% for
men between 2010 (50.3 visits per 100,000 population) and 2013 (68.5 visits per 100,000 population). For women, the increase was approximately
21% (2010: 42.8 visits per 100,000 population; 2013: 51.8 visits per 100,000 population.) By age group, the rate was highest among men aged 25-
34 (146.5 visits per 100,000 had the highest rate. In 2013, there were a total of 2,506 ED visits due to drug overdose,for a rate of 122.8 visits per
100,000 population.The rate of opioid overdose related ED visits was 60.4 visits per 100,000 population and the rate of heroin overdose-related
ED overdose-related ED an was 70%. Among women, those aged 35-44 (80.5 visits per 100,000 population), representing 57% of all opioid
overdose-related ED visits and 27% of total drug overdose-related ED visits. Both men and women between the ages of 15-54 had high rates of
opioid overdose-related ED visits. However, men between the ages of 15-34 had higher rates compared to females, with the highest rate among
men between the ages of 25-34 (146.5 visits per 100,000 population) being 48% higher than women in the same age group (70.9 visits per
100,000 population). visits per 100,000 population) was almost 27% higher visits per 100,000 population) was almost 27% higher than that for
heroin overdose, representing 57% ofall opioid overdose-related ED visits and 27% of total drug overdose-related ED visits. Poisoning was the
leading cause of unintentional injury death from 2007 through 2014, followed by motor vehicle traffic-related injury and fall-related injury. About
90% of unintentional poisoning deaths in NM are due to drug overdose.” [1}
Mr. Saavedra, form the New Mexico Department of Health, further states:
“The data presented are worrisome since the most affected age group corresponds to the working age population, re-emphasizing the toll
substance abuse imposes on society. Furthermore, the age groups among women correspond to their reproductive ages, which may explain
the increasing trends in rates of neonatal abstinence syndrome that have been observed nationally.” [1]
12. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 12
12
Opioid Overdose Citizens Data Conclusions:
So, lets sum this up in a few sentences.: Opioid overdose emergency visits have increased 30% and are increasing in both
sexes. Both men and women between the ages of 15-54 have the highest rates of opioid overdoses with men ages 25-34 the
highest, women 35-44 the highest, and these women are in reproductive age thus increasing the neonatal abstinence
syndrome. Now one overdose can kill or seriously harm two New Mexicans.
Overdose Deaths. This is the hardest part of the research, the ones who have already died from opioid overdose, many
needlessly, where I believe many could have still been here today. Perhaps their sacrifice will save others yet to come.
How bad is the death now in America? Well, heroin overdoses only have surpassed the homicide rate for guns in
America:
{70}
13. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 13
13
This data represents those who died from opioid overdoses in New Mexico. What we know about this data: Substance
abuse is ravaging the Native American reservations and unfortunately it is no different for deaths from opioids.
Native Americansare dyingatrate double ortriple the rate of the rest of the population. {2}
White,Black, andHispanicNewMexicanshave verysimilaroverdose deathrates.
So, opioid pain reliever overdose deaths occurred 89.2% ofthe time with those with chronic medical conditions.
Andalmost70% of the time theyoccurred in the home and withbystanders yetonly 20% of the heroin users were given
Naloxone andonly 10%of the opioidpain relieveroverdose deaths receivedNaloxone.{3}
Who is dying of opioid overdoses? Native American citizens at rate 2 or 3 times the rest of the New Mexico population.
Hispanic, Black and White New Mexicans are dying at about the same rate. So, those who overdose from prescription
opioids, almost 90% of them have chronic medical conditions. Overdoses predominantly occur at home and with
somebody else there. Only 20% of heroin users received Naloxone and only 10% prescription users received Naloxone,
therefore less than 80% of overdose opioid deaths receivedNaloxone. And I suspect that rural New Mexicans are
dying at disproportionate rates over more populated areas.
Where Are the Deaths in New Mexico? Now that we know the “Who” of opioid overdose New Mexican citizen deaths,
the next important determination is where they are most happening per capita? First, given the rural considerations of New
Mexico, it is important to see that opioid overdose deaths are happening at a rate 45% higher than in rural areas and that
there is rarely any help for substance abuse treatment services nearby when they do not die from an overdose: {4}
15. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 15
15
Recently, Governor Suzanna Martinez and the Department of Health announced a reduction in overdose deaths in New
Mexico and this was spread across the United States media as a triumph. {5} While, we must applaud any and all deaths
saved in New Mexico, and we must thank each and every person who had any involvement in that reduction, 69 New
Mexicans stayedalive in 2015 and total overdose deaths declined by 9% statewide. Yet, we must also think critically
about this newest data. The article, entitled, “Overdose Deaths Decline in Nearly Two-Thirds of New Mexico’s 33
Counties,” we must look closer and think critically about these results. First, this is all overdoses which would include
alcohol, other drugs, etc. Second:
What is the opioid overdose rate for 2015?
The heroin overdose death rate increased although it is not stated by how much?
The drug overdose rate declined by 7.5%, not 9%.
The prescription opioid overdose rate death rate decreased but we do not know by how much?
If we look at where the decreases were, 36% of the death reduction happened in 3 more populated counties:
Valencia, Sandoval, and San Juan counties. If we count in Rio Arriba County’s reduction, 53% of the death
reduction were in these 4 counties. What might have changed in these counties to reflect the decrease? The
drug supply on the street through interdiction by law enforcement, excellent pharmacy participation, better EMS
resources, Naloxone distribution, well-staffed hospital emergency rooms, new and effective education and
prevention programs? We should be studying these 4 counties right now with an eye for things like: what kind
of abusers are overdosing still here and what kind aren’t (prescription, illicit, heroin, age, sex, race, location of
overdoses, changes in local programs, law enforcement interdiction, supply of drugs on the street, interviews of
overdosed citizens, etc.)
How many of these 69 people were reversals using Naloxone?
16. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 16
16
Rio Arriba County, Ground Zero:
Rio Arriba County has steadily remained beyond epidemic for too many years leading New Mexico, and America in
opioid overdose deaths. Opioid abuse is almost acceptable, endemic, in the community:
,
February 2000
“Beautiful Land, Ugly Addictions”
Comparison of heroin overdose death rates per 100,000 people per year from 1996-1998:
US national rate: 2.2
New Mexico Rate: 9.4
Rio Arriba County rate: 35.5
Chimayo is the "heroin capital" of Rio Arriba County, a rural region of 34,000 people with one of the highest rates of
drug overdose in the United States… {6}
And this very insightful, although parts are questionable, article:
New Mexico has not stood by as fatal overdoses skyrocketed in Rio Arriba County — from 7 in 1990 to 40 in 2014,
according to state health department data — and statewide, from 131 to more than 500. The state boasts one of the most
sweeping harm reduction programs in the nation. Rio Arriba County is home to a nationally recognized doctor who
prescribes proven anti-addiction medications, several local drug treatment centers, and an anti-overdose strategy that
puts lifesaving drugs into the hands of law enforcement. Drug-ridden towns elsewhere are just discovering
strategies Española has been practicing for decades.
So why, given New Mexico’s pioneering efforts, hasn’t the situation improved?
“Fernando Espinoza has known dozens of people killed by addiction to drugs and other substances. An aunt. An uncle. A
cousin. Too many friends and fellow inmates to count. Espinoza, 32, has spent 14 consecutive birthdays in jail. When he’s
out, he lives with his mother at her home in Española. He has two daughters, a GED, and an addiction to heroin that feels
like something scratching inside his brain. Here in Rio Arriba County, where one in five residents lives in poverty,
people overdose and die more often than almost anywhere else in the country. Over the past five years, the county’s
overdose rate was three times the statewide average, and more than five times the national rate. According to a 2013
survey of 969 Española teenagers, nearly 5 percent of high school students had used heroin within the last month, as
opposed to 2.9 percent statewide.
Attempts to treat addiction here have been undermined by a failure to focus on prevention, a lack of resources and an
unanticipated boom in prescription drug sales. And for all the state and county have tried, their efforts have not
changed the factors that drive people here to addiction in the first place. Among them: generations of poverty and a lack
of jobs that leave people with few good alternatives. The Naloxone program:
Five days a week Fiuty and harm reduction program manager Dave Koppa drive the streets of Española, visiting homes,
stopping in parking lots and open fields, and pulling over when people wave at them from sidewalks. They offer tips on
how to shoot heroin without creating infected abscesses. They explain the dangers of mixing pills and alcohol, and give
out for free an overdose reversal drug called Naloxone…. In the past year alone, the Santa Fe Mountain Center’s
17. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 17
17
needle exchange programs collected over 1 million needles, gave away more than 3,000 doses of Naloxone, and
recorded more than 700 successful overdose reversals.
…That such recidivism persists despite the state’s efforts haunts Salazar and other advocates. For one thing, the
community’s need has always exceededits resources. Except for pregnant women, Hayes, the buprenorphine-
prescribing doctor, has hardly taken a new patient in three years. A local residential treatment center, Hoy
Recovery, has nearly 50 beds – eight of them for detox – but they are regularly full of people from around the state.
On a recent afternoon at Hoy, the waitlist for men was 28 people long.
“The services that are available work,” said Lauren Reichelt, head of the department of health and human services in
Rio Arriba County. “Just not at a scale to meet the need.” {7}
Kudos to the Santa Fe Mountain Center and its efforts to distribution Naloxone, 3,000 units and 700 recorded
reversal, in one year. That means that four every 4 doses of Naloxone given out, 1 reversal was achieved. The death
rate did go down here some in 2016, perhaps because of their efforts. And yet it remains now 16 years later, by far, the
highest in New Mexico…This county has suffered long enough and if anywhere, why don’t we begin here?
“Sanches, still a certified paramedic, joined Rio Arriba County Sheriff James Lujan, U.S. Attorney Damon Martinez and
other law enforcement leaders at a news conference in Albuquerque on Monday, announcing a program to help local
agencies get funding to start carrying the overdose-reversing drug Narcan, also known by its generic name,
naloxone. “Law enforcement is sworn to protect life, limb and property, and amongst that is dealing with the opiate
crisis that is so prevalent right now,” Sanches said, highlighting the need for officers to carry and administer Narcan.
The antidote wasn’t around when he first started as a medical technician and the awareness surrounding the issue is long
overdue. All 28 Rio Arriba County deputies have been `…. Despite the week presenting an opportunity for Rio Arriba
County to highlight the fact that its people suffer from overdose rates well above national averages, the County did not
participate in these events, did not host any events or make any official announcements…. “Every week is Heroin
Awareness Week for Rio Arriba County government and has been for several decades,” Health and Human
Services Director Lauren Reichelt wrote in an email Tuesday. “We’re glad everybody else in the country has
caught up and realized.” She said her Department is working to develop a local diversion program and a provider
network to get Narcan on the streets. In June, she started purchasing goods and services that will become the backbone
of the Behavioral Health Investment Zone, paid for through the first installment of a five-year, $2.5 million grant
from the state of New Mexico, meant to address behavioral health problems associatedwith drug abuse in the
County…
Sanches said, at a minimum, and as soon as possible, the County needs a 100-bed in-house recovery facility. He said the
entire north central region of the state has no recovery services after a program in Taos closed this summer, and the
state as a whole, does not have enough space available for recovering addicts. “No change is evergoing to occur until
the people in power empower those who can make change,” he said.” {8}
Kudos to Ms. Reichelt and Officer Sanches, they get it…This story is not about Ms. Reichelt not attending the
promotional awareness week efforts. She has been on the front lines of this epidemic in the worst county in the
18. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 18
18
state. Maybe she is tired of hearing all the pronouncements, proclamations, promises, and poor strategies that have not
worked. When everyone goes home after the awareness week, she faces more deaths. This story is about her seeing
that Naloxone needs to be on the streets of Rio Arriba County. And it is about a law enforcement officer who has
seenall the deaths and equipping the department with Naloxone. The story is about the fact that deputies just
started using the Narcan a month ago, in September 2016, in the worst epidemic at the county level in the United
States. It is about them already using it 5 times in a month, which would be 60 lives savedin a year’s time. And it
is about the fact that there is no safety net and treatment for these citizens after they overdose at ground zero in
New Mexico. That means they will be back and more Narcan is used to save their lives, again or they may just die.
I do not know why, with the money we have allotted for this state, that there are not construction companies
building a recovery hospital in the heart of Rio Arriba County right now, where it belongs, with the American and
New Mexican flags flying in front of it? All of these questions are really what needs to be studied, so why aren’t we?
Wouldn’t we want to know this most immediately, then fund and export these strategies to the rest of New Mexico? All we
know is what Cabinet Secretary Designate of the Department of Health, Lyn Gallagher states:
“We are working hard to reduce overdose deaths in New Mexico. The recent decrease shows we’re making progress, but we
still have a lot more work to do,” said Departmentof Health Secretary DesignateLynn Gallagher. “The fact is, our state
continues to suffer from drug abuse. One overdose death is one too many. And until we have zero fatalities related to
drugs, we’re going to continue to do all that we can to address the issue with our partners.” {5}
The truth is the Department of Health does not really know why and I know more about what is not working in the
voluminous data than what does. But at least we have the same goal, “zero fatalities.”
The Behavioral Health Collaborative, headed by Wayne Lindstrom, PhD, who also an employee of the New Mexico Human
Services Division indicates in his annual report:
The Behavioral Health Collaborative administers a yearly $1M dollar federal grant:
19. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 19
19
Mr. Lindstrom’s organization had to withdraw some initiatives that would have also been helpful for opioid abuse
reduction in general in New Mexico.
{9}
20. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 20
20
The Rest of New Mexico: We also know where else there are serious issues with drug overdose deaths: {10}
Why this is 2014 data presented in 2016, I don’t understand? In any event, I suspect that the rates are similar now unless
there has been a community suddenly hit (like Lincoln County, see below) {} So, in the concern for total overdose deaths, I
am very concerned that Bernalillo and Santa Fe Counties are above the state average.
22. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 22
22
This shows that Lomas/Broadway in Bernalillo County, the Agua Fria Neighborhood in Santa Fe County, McKinley County, for
example, are problem areas which will allow more targeting of efforts by area. This is very important and excellent data,
well done Dr. Landen and staff. I am also interested that Dona Ana County, the second largest county in population in
the state, and so near El Paso (see below) and the Mexican Border, would have much lower rates, why? That’s worth a
study…
The Native American Reservations. As with most every other Native American issue in the United States, the Native
American community is often forgotten and/or marginalized. For a culture and people who were in New Mexico before most
of the rest of New Mexicans by many generations, and only had illicit substances that have turned into addictions in the last
few generations, we must devote resources here if they are dying at rate 2 to 3 times the rest of us. And not that it should
matter, but many Native Americans reservations are within or near metropolitan areas where there is not a reservation
hospital. So, they are often taken to New Mexican hospitals, if we want to just look at the economic impact. There are
some promising efforts: {73}
HHS Secretary Sylvia M. Burwell has made addressing opioid abuse, dependence and overdose a priority and through an
evidence-based initiative focused on three promising areas: informing opioid prescribing practices, increasing the use of
naloxone and using medication-assisted treatment to move people out of opioid addiction. The Obama administration
is also committed to combatting the prescription drug and heroin epidemic, proposing significant investments to intensify
efforts to reduce opioid use disorder…. The new agreement formalizes the partnership between IHS and BIA to reduce
opioid overdoses among American Indians and Alaska Natives. In 2016, the more than 90 IHS pharmacies will dispense
naloxone to as many as 500 BIA Office of Justice Services officers and will train these first responders to administer
emergency treatment to people experiencing opioid overdose. The partnership will be reviewed annually by IHS and BIA
and will continue as long as the agencies agree it is delivering the desired results. “I am deeply grateful to the IHS for
working with us to create another level of safety throughout Indian Country for those trapped by the vicious cycle of drug
addiction," said BIA Director Michael S. Black. "Law enforcement officers are usually the first responder to a drug
overdose situation in a tribal community. This partnership greatly strengthens our public safety mission by
enabling our BIA officers to take immediate action to save a life endangered by an overdose. ….an immediate action
to save a life endangered by an overdose."
While I continue to stress within this paper that giving Naloxone to BIA officers is still not going to reach the users
themselves as effectively, it is much better than no Naloxone at all, and as first responders, it will, definitely, save
some lives. And again, we see the belief that the pharmacies should be the gatekeepers for Naloxone, based on an
assumption that is not working.
23. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 23
23
Also, critical to understand is exactly where the overdose death occurred and how often Naloxone was given by drug
type. Here is a study completed in 2012, by The Center For Disease Control, in New Mexico, by using the records of the
Office of Medical Examiner death records: {13}:
Of the 489 overdose deaths reviewed, 49.3% involved OPR, 21.7% involved heroin, 4.7% involved a mixture of OPR and
heroin, and 24.3% involved only non-opioid substances. The majority of OPR-related deaths occurred in non-Hispanic
whites (57.3%), men (58.5%), persons aged 40–59 years (55.2%), and those with chronic medical conditions (89.2%).
Most overdose deaths occurred in the home (68.7%) and in the presence of bystanders (67.7%). OPR and heroin deaths did
not differ with respect to paramedic dispatch and CPR delivery, however, heroin overdoses received naloxone twice as
often (20.8% heroin vs. 10.0% OPR; p < 0.01).
•Most unintentional overdose deaths were due to prescription opioids or heroin.
•Most overdose deaths occurred in the home, often in the proximity of family.
•Decedents most often had a known history of drug dependency or prior overdose.
•Heroin overdoses received naloxone twice as often as prescription opioid overdoses.
Fentanyl and Synthetic Opioids. As if it isn’t bad enough, new, even more dangerous and addictive, synthetic opioids
are being sold on the street of the United States, and New Mexico:
“…officials are investigating the deaths of at least 20 people who overdosed on the powerful painkiller fentanyl in New
Mexico this year, apparently after taking what they thought was black-market oxycodone. The victims ranged in age
from 17 to 63; 17 of the 20 were men. The price of oxycodone is normally $1 per milligram, or $30 for one 30-
milligram pill, but the fentanyl pills have been sold for as little as $5 a pill around the country. The counties of
residence of those who died were Bernalillo, Chaves, Lea, Lincoln, Colfax, Eddy, Guadalupe, Otero, Sandoval, San
Miguel, Santa Fe, Valencia and one unknown. Fentanyl has long been prescribed for people suffering from chronic
pain, often associated with cancer, but in recent years, fentanyl has shown up on the illegal drug market, leading to many
overdose deaths in New England and mid-Atlantic states. There, the drug is often mixed with heroin by dealers to give
their product an extra kick or to cheaply produce more usable heroin. Now the odorless white powder is being made
into pills and passedoff as another drug.” {14}
“…Drug Enforcement Agency agents say the pills were likely manufactured in Mexico using fentanyl powder from
China that can cost a few thousand bucks for a kilogram and be turned into counterfeit oxycodone pills that can net
traffickers millions of dollars. Toxicology tests in the 20 New Mexico deaths showed fentanyl and slightly different
chemical versions of it, called analogs, which can be stronger than legally produced fentanyl and may take more
naloxone (Narcan) to counter than it would to counter a heroin overdose…. If that scares you, and it should, consider
the growing use of carfentanil, a synthetic anesthetic designed to tranquilize elephants and other large animals. It is
not approved for use in humans, but drug traffickers are mixing it with heroin and it has become popular in some states
among addicts looking for ever stronger highs. It has caused hundreds of overdoses and several deaths in states like Ohio,
which has been particularly hard hit. Carfentanil is 10,000 times more potent than morphine and 100 times stronger
than fentanyl, as reported by columnist Diane Dimond in a recent Albuquerque Journal article. So, we have Chinese
chemists and Mexican drug pushers, to thank for introducing evenmore powerful ways to make obscene profits at
American addicts. But part of the solution must lie with slowing the demand on the U.S. side of the border for high-
risk drugs that damage and destroy lives and families. Which is why the HOPE (Heroin and Opioid Prevent and
24. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 24
24
Education) Initiative of the U.S. Attorney’s Office for the District of New Mexico and the University of New Mexico’s
Health Sciences Center is so important. In addition to prosecution, its focus is on diversion, rehabilitation and re-entry
programs and it is working with community organizations, such as the Bernalillo County Opioid Accountability Initiative.
The fact that people are so addicted that they are willing to turn to knock-off drugs or buy pills they think – hope –
are the real thing says a lot about how serious the drug epidemic has become. This is a new kind of drug war.” {15}
Well said, Albuquerque Journal, you get it. And these new drugs are inherently dangerous to everybody:
“Right now we’re seeing the emergence of a new class — that’s fentanyl-type opioids,” Dye’s boss, Jill Head, explained.
“Based on the structure, there can be many, many more substitutions on that molecule that we have not yet seen.
“Entrepreneurial” chemists have been creating designer alternatives to cannabis, amphetamine, cocaine and Ecstasy for
years. But this new class of synthetics is far more lethal. Back in 2012 and 2013, when reports of fentanyl derivatives
started coming in to the U.N. Office on Drugs and Crime in Vienna, chemists chucked them in the “other” category. Today
those “other” substances are one of the fastest-growing groups of illicit chemicals tracked by the agency. “New opioids
keep emerging,” said Martin Raithelhuber, an expert in illicit synthetic drugs at the U.N. They deserve their own category,
he added, but that will take time. Once, forensic chemists like Dye confronted a familiar universe of methamphetamine,
cocaine and heroin. Drug dealers, users and DEA agents generally knew what substance they were handling. Today, things
are different. This is a golden age of chemical discovery — and subterfuge. Dealers may not know that the high-purity
heroin from Mexico they’re selling has been laced with fentanyl. Users may not realize the robin’s-egg-blue
oxycodone tablets they’re taking are spiked with acetylfentanyl. If field agents bust a clandestine drug lab and see
a cloud of white powder in the air, they no longer assume it’s cocaine. They run.” {16}
So, our law enforcement personnel are themselves in danger of accidental poisoning and possible death in busting
these labs. If we are to be so unlucky as to come into a place with unknown white powder floating around, we can die on
the spot and we may not even be users at all. And here is China’s role with a link to our neighboring state, Utah, using the
internet to buy fentanyl:
“Baer said theDEA is actively investigatingU.S.-based vendors who use dark net markets to sell fentanyl and related compounds, as well as
Chinese companies that use U.S. servers to sell carfentanil.Butthe extent to which those U.S. companies aremerely retailingmade-in-China
drugs is not clear.Baer said the DEA doesn’t believe fentanyl is mass-produced in the U.S., though authorities haveuncovered mom-and-pop pill
press operations. One of them was run by a 28-year-old in Utah, who was busted latelastmonth with a pill press,piles of powder and cash,and
nearly 100,000 pillslaced with suspected fentanyl in his Cottonwood Heights home. Accordingto the criminal complaint,theyoung man hired
people to accept packages shipped to their homes, which they’d hand over, unopened. The packages came from China.”{16}
And the newest study, justreleased, from the Center for DiseaseControl on opioid overdosedeaths, using2015,data: {17}
“During 2015,drug overdoses accounted for 52,404 U.S. deaths, including33,091 (63.1%) that involved an opioid.There has been progress in
preventing methadone deaths, and death rates declined by 9.1%. However, rates of deaths involvingother opioids,specifically heroin and
synthetic opioids other than methadone (likely driven primarily by illicitly manufactured fentanyl) (2,3), increased sharply overall and acrossmany
states. A multifaceted, collaborative publichealth and lawenforcement approach is urgently needed. Response efforts includeimplementingthe
CDC Guideline for Prescribing Opioidsfor Chronic Pain (4), improvingaccess to and use of prescription drugmonitoringprograms, enhancing
naloxone distribution and other harm reduction approaches, increasingopioid usedisorder treatment capacity,improving linkageinto
treatment, and supporting law enforcement strategies to reduce the illicit opioid supply.
25. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 25
25
TABLE 1. Number and age-adjusted rate of drug overdose deaths* involving natural and semisynthetic opioids† and methadone,§ ,¶ by sex,
age group, race/ethnicity, ** U.S. Census region, and selected states†† — United States, 2014 and 2015
Natural and semisynthetic opioids Methadone
2014 2015 % change
in rate,
2014 to 2015
2014 2015 % change
in rate,
2014 to 2015Characteristic No. (Rate) No. (Rate) No. (Rate) No. (Rate)
Overall 12,159 (3.8) 12,727 (3.9) 2.6§§ 3,400 (1.1) 3,301 (1.0) -9.1§§
Sex
Male 6,732 (4.2) 7,117 (4.4) 4.8§§ 2,009 (1.3) 1,939 (1.2) -7.7§§
Female 5,427 (3.3) 5,610 (3.4) 3.0 1,391 (0.9) 1,362 (0.8) -11.1§§
Age group (yrs)
0–14 42 (0.1) 48 (0.1) 0.0 14 –¶¶ 13 –¶¶
–¶¶
15–24 726 (1.7) 715 (1.6) -5.9 241 (0.5) 201 (0.5) 0.0
25–34 2,115 (4.9) 2,327 (5.3) 8.2§§ 796 (1.8) 735 (1.7) -5.6
35–44 2,644 (6.5) 2,819 (6.9) 6.2§§ 768 (1.9) 739 (1.8) -5.3
45–54 3,488 (8.0) 3,479 (8.1) 1.3 854 (2.0) 843 (2.0) 0.0
55–64 2,437 (6.1) 2,602 (6.4) 4.9 629 (1.6) 642 (1.6) 0.0
≥65 706 (1.5) 736 (1.5) 0.0 98 (0.2) 127 (0.3) 50.0§§
Sex/Age group (yrs.)
Male
15–24 529 (2.3) 493 (2.2) -4.3 173 (0.8) 149 (0.7) -12.5
25–44 2,869 (6.8) 3,139 (7.4) 8.8§§ 969 (2.3) 926 (2.2) -4.3
45–64 3,015 (7.4) 3,095 (7.5) 1.4 808 (2.0) 777 (1.9) -5.0
Female
15–24 197 (0.9) 222 (1.0) 11.1 68 (0.3) 52 (0.2) -33.3
25–44 1,890 (4.5) 2,007 (4.8) 6.7§§ 595 (1.4) 548 (1.3) -7.1
45–64 2,910 (6.8) 2,986 (6.9) 1.5 675 (1.6) 708 (1.6) 0.0
Race/Ethnicity**
White, non-Hispanic 10,308 (5.0) 10,774 (5.3) 6.0§§ 2,845 (1.4) 2,725 (1.4) 0.0
Black, non-Hispanic 814 (2.0) 878 (2.1) 5.0 256 (0.6) 247 (0.6) 0.0
Hispanic 727 (1.4) 780 (1.5) 7.1 228 (0.5) 235 (0.5) 0.0
U.S. Census region of residence
Northeast 1,851 (3.3) 2,095 (3.6) 9.1§§ 587 (1.0) 643 (1.1) 10.0
Midwest 2,205 (3.3) 2,302 (3.4) 3.0 675 (1.0) 673 (1.0) 0.0
South 5,101 (4.2) 5,374 (4.4) 4.8§§ 1,298 (1.1) 1,228 (1.0) -9.1§§
Synthetic opioids other than methadone Heroin
201
4
201
5
%
change
in rate,
2014 to
2015
201
4
201
5
%
change
in rate,
2014 to
2015
Characteristic No. (Rate) No. (Rate) No. (Rate) No. (Rate)
Selected states††
Stateswith very good or excellent reporting (n = 21)
Alaska 14 –¶¶ 14 –¶¶
–¶¶ 25 (3.3) 37 (4.7) 42.4
28. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 28
28
Virginia 176 (2.1) 270 (3.3) 57.1§§ 253 (3.1) 353 (4.3) 38.7§§
Washington 62 (0.8) 65 (0.9) 12.5 289 (4.1) 303 (4.2) 2.4
West Virginia 122 (7.2) 217 (12.7) 76.4§§ 163 (9.8) 194 (11.8) 20.4
Wisconsin 90 (1.6) 112 (2.1) 31.3 270 (4.9) 287 (5.3) 8.2
Stateswith good reporting (n = 7)
Colorado 80 (1.5) 64 (1.2) -20.0 156 (2.9) 159 (2.8) -3.4
Georgia 174 (1.7) 284 (2.8) 64.7§§ 153 (1.6) 222 (2.2) 37.5§§
Illinois 127 (1.0) 278 (2.2) 120.0§§ 711 (5.6) 844 (6.7) 19.6§§
Minnesota 44 (0.8) 55 (1.0) 25.0 100 (1.9) 115 (2.2) 15.8
Missouri 109 (1.9) 183 (3.1) 63.2§§ 334 (5.8) 303 (5.3) -8.6
Ohio 590 (5.5) 1,234 (11.4) 107.3§§ 1,208 (11.1) 1,444 (13.3) 19.8§§
Tennessee 132 (2.1) 251 (4.0) 90.5§§ 148 (2.3) 205 (3.3) 43.5§§
Source: CDC. National VitalStatistics System,Mortality. CDC WONDER. Atlanta,GA: US Department ofHealth and Human Services, CDC; 2016.
https://wonder.cdc.gov/.
* Rates arefor thenumber of deaths per 100,000 population. Age-adjusted deathrates werecalculated using thedirectmethodand the 2000 standard
population. DeathswereclassifiedusingtheInternationalClassificationofDiseases,TenthRevision(ICD–10).Drugoverdosedeaths wereidentifiedusing
underlyingcause-of-death codes X40–X44, X60–X64, X85,and Y10–Y14.
† Drug overdose deaths,as defined, that have synthetic opioids other than methadone (T40.4) as contributing causes.
§ Drug overdose deaths,as defined, that have heroin (T40.1) as a contributing cause.
¶ Categories ofdeaths arenotexclusivebecausedeathsmightinvolvemorethanonedrug.Summingcategorieswillresultinanumbergreaterthanthetotal
number of deaths in a year.
** Data for Hispanicethnicity should be interpreted with caution; studies comparing Hispanicethnicity on death certificates and on census surveys have
shown inconsistent reporting.
†† Analyses werelimitedto states meeting thefollowingcriteria.Forstates withverygood toexcellentreporting,≥90% ofdrug overdosedeathcertificates
mention at least onespecificdrug in2014,withthechangeinpercentage of drug overdose deaths mentioningatleastonespecificdrugdifferingby <10
percentage points from 2014to 2015.States with good reporting had 80% to <90%of drug overdose death certificates mention at leastone specificdrug
in 2014, with the change inthepercentageofdrugoverdosedeaths mentioningatleastonespecificdrugdiffering by<10percentage pointsfrom2014to
2015. Ratecomparisons between states shouldnotbemadebecauseof variations inreportingacrossstates.
§§ Statistically significantatp<0.05 level. Gamma tests wereusedifthenumber ofdeaths was <100 in 2014or 2015,andz-tests wereusedifthenumberof
deaths was ≥100 inboth 2014 and 2015.
¶¶ Cells with nine or fewer deaths arenot reported, and rates based on <20deaths arenot considered reliable and not reported.
I am unsure why this data is showing a 25% reduction in opioid overdose deaths for New Mexico, when our data and press
conferences indicate 7.5% (?) I also note the 12% increase in heroin overdose deaths in New Mexico. I submit to you
again, we are at a real war, and we are being attacked by increasingly more insidious, habit-forming, overdose death
risk heightened, drugs, brought from around the world and within our country.
Cost/Benefit Analysis of Opioid Overdose Death. When we think of resources to fight this epidemic, we must consider
what we have already. Millions of dollars are poured in annually to address the problem in New Mexico. Criminal justice
and drug treatment organizations, emergency responders, community groups and activists who care about this issue and
want it changed, agencies and organizations already existing who can better address this problem by coordination
and non-duplication of efforts, and finally, most importantly, we have the citizens of New Mexico – the fathers,
mothers, brothers, sisters, neighbors, and evenstrangers of the opioid overdose victim. And we have the saved
overdosed citizens, who are an untapped resource in the opioid overdose death epidemic. I will focus now on the
29. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 29
29
economic costs of opioid overdose death in New Mexico because, in the end, we cannot put a price on the amount of a
saved New Mexico citizen who overdosed – not to his or her family, his friends, his community, and not to all citizens of
New Mexico. And I wonder if we collectively have decided that the death of an opioid overdose citizen is somehow
expendable, deserved, or just the acceptable risk results of drug abuse that cannot be changed.
So, if we want to do a cost benefit analysis of saving opioid overdose citizens from death from a strictly economic
point of view, the numbers are as follows:
The hospital costs of opioid abuse in New Mexico is $192M ($25B in the United States) each year which
equates to a cost of $92.00 for every New Mexican citizen each year. And these are very conservative
estimates. More recent data shows it to be $28B in the United States. {18} And fatal overdoses alone
account for $21B a year. {19}
The average United States cost of every emergency room visit where the overdose victim was treated and
released is $3,640 and if admitted to the hospital, $29,497. 59% of all overdose patients are admitted to
the hospital. [69]
30. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 30
30
Other societal costs include $5B a year in criminal justice costs and another $25B per year in lost workplace
productivity. (While there is a whole plethora of data and studies in New Mexico, I could not find this data for some
reason, specifically related to New Mexico). Newer data now show criminal justice costs at $7B. [19]
And this is every year….
Statewide Naloxone Distribution. I submit to you that the best strategy for the cost is widespread Naloxone distribution
in New Mexico where it is most effective, in the hands of the drug users themselves. And this cannot be done, alone, by
pharmacies for several reasons:
1. How many citizens overdose on opioids in the parking lot of the pharmacy?
2. How many overdose at risk citizens are willing to go into a pharmacy, talk to a pharmacist, and then provide their
information which is then provided to a government agency? And how many families and friends? How many
concerned citizens, who just want to have Naloxone in case they come across an overdosing citizen, will go into a
pharmacy and ask for it?
3. How many, especially rural, overdose prevention citizens can even get to a pharmacy before the person overdosing
dies? What if they are elderly, cannot drive, handicapped, mentally unstable?
4. One big pharmaceutical company, is willing to donate Naloxone kits to every high school in New Mexico.
Have we done this? Apparently not. In addition, they provide a cellular phone application, for both Android
and Apple phones, that tells how to administer the Naloxone, safety information, education, even a video, and 911
call button- Free. And they are offering substantially discounted Naloxone pricing to law enforcement and
government agencies.
5. Opioid overdose abuse victims often take the opioid with at least one other person(s). [2] Often by the time
law enforcement or emergency services personnel arrive, the other person(s) have left the scene, afraid of the
repercussions of being arrested or involved with an overdose victim, especially if they die. What if these other
person(s) had a Naloxone kit with them, could administer the drug, and then leave the scene after calling 911?
31. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 31
31
And what is really, well, disturbing is, we began a Naloxone program in 2001 in New Mexico, from a recent
presentation made by University of New Mexico Project Echo:
“To respond to the highest per capita heroin- related death rate in the nation, NM passed the 1st law which funded
statewide OD prevention and Naloxone distribution (administered by the NM Dept. of Health). The law directs the NM
Dept. of Health to: “Develop a program to train lay persons to administer Naloxone to another person in case of opiate
overdose.” {20}
And this article from 2001, when the program began under Governor Gary Johnson: {21}
…a controversial package of drug-policy reform legislation introduced by New Mexico Gov. Gary Johnson in January, one
law that passed without much of a struggle was aimed at increasing use of naloxone…Fear of infection also plays a role
in the aversion to naloxone use, according to speakers at the recent Lindesmith Center-Drug Policy Foundation annual
conference, held in Albuquerque, N.M. For example, overdose victims who receive naloxone require rescue breathing
immediately after the shot is administered — a dicey prospect for police or even emergency medical personnel, who may
fear infection with HIV or hepatitis via blood, saliva, or other bodily fluids…. But experts at the conference said that
using a protective mask equipped with a one-way breathing tube and a plastic shield can minimize these risks. “I
think the cops will use it if given reassurance by Emergency Medical Services,” said Dr. Steve Jenison of the New
Mexico Department of Health. “It gets the job done.” Harder to overcome may be simple prejudice against addicts.
“What I hear in conversation is that those lives are not necessarily valuable,” according to Maureen Rule, clinical
advisor to Albuquerque's Health Care for the Homeless. “The response I hear is, 'So what if they die?’” But New
Mexico Secretary of Health J. Alex Valdez asserted, “[Naloxone is] used for one reason and one reason alone, and
that's to save lives. You can debate the use of naloxone, but if you value the life of a person regardless of his
addiction to heroin — if saving a life has value — then it's worth $1.50.
The New Mexico legislation also protects individuals from civil liability or criminal prosecution for using an opioid
antagonist, as long as they act in “good faith” and with “reasonable care.” Rule noted that prior to the legislation,
“Doctors were reticent about anything that was outside the standard care, but now the law provides legal protection.” New
Mexico officials said they want to see naloxone distributed via police to injection-drug users and their family members and
friends throughout the state. And speakers at the drug-policy reform conference said that making naloxone more
readily available nationally would help fight an explosion in opioid overdose deaths. The New Mexico legislation
was sparked by the state's alarming overdose death rate, centered in Albuquerque and in Rio Arriba, the huge rural
country stretching north from Santa Fe to the Colorado border. Jenison reported that between 1996 and 1998, the statewide
incidence of fatal overdose from illicit drugs, primarily heroin, was 7.8 deaths per 100,000, nearly four times the national
average. Populated largely by Native Americans and Mexican-Americans, Rio Arriba experienced a catastrophic 35 deaths
per 100,000 population in 1998, and had at least sixteen overdose deaths in 2000. Bigg added — with deliberate
ambiguity — that his program has been distributing naloxone “for a while” in Chicago to about 300 drug users, doctors
and others. “Some doctors were involved who didn't want to be known, but now we have an 'out' physician,” he said.
Among his clients, he reports there are “forty-three people who were blue and unresponsive who are alive today.”
Jenison reported that since discussion about naloxone heated up in January, “a dozen or so private physicians” in New
Mexico have been prescribing it to users and their families in and around Espanola, Rio Arriba County's biggest city.
But physician involvement in prescribing the drug remains scant in Albuquerque, Jenison said. In rural settings,
such as Rio Arriba, experts noted, users are more likely to have a home to store the drug and access to a doctor.
They're also more likely to have an intact family structure to watch over them and administer the drug, since, as
32. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 32
32
Wayne A. Salazar, Espanola's chief of police, stated, “Heroin use is somewhat socially acceptable in the Hispanic
community in Rio Arriba.” With 24 overdoses — including 8 fatalities — in his jurisdiction in the prior four months,
Salazar would like to see his officers carrying naloxone by mid-July. He says he's already gotten positive feedback.
“There's nothing more frustrating during an OD then waiting that eight to 13 minutes for the EMTs to show up
and not being able to do a lot, all the family and friends crying all around you,” said Salazar. Of course, police are as
helpless as ever if no one calls 911. Fearful of arrest, some users will actually let a companion die rather than call for
help. Harm-reduction specialists counsel users on techniques for safely calling 911, but even so, getting naloxone into
users' hands remains a huge stumbling block.
Heather Meschery, executive director of the Santa Cruz Needle Exchange, noted that 11 percent of her clients have been
arrested in conjunction with an overdose. And Salazar said his is one of only two police departments in New Mexico
that doesn't arrest overdose victims. Salazar's do officers confiscate personal-use amounts of heroin found on the scene,
and will investigate anything that looks like potential distribution. To counter this problem, advocates want to make
naloxone widely available in the user community. The New Mexico law currently applies to licensed professionals with
prescription-writing authority, but Cliff Rees, a lawyer for the state health department, said the regulations could be
broadened by mid-September to permit any person to administer the drug without fear of liability. “It’s a goal” to
have it in users' homes, Rees said. Bigg stated that users “have to discuss, plan and prepare for” use of naloxone.
“And you have to have it around — you can't be hunting it down,” he noted. One couple, for instance, keeps an 'OD
box' with a red cross on it. Of course, Bigg said, all bets are off for users who persist in using alone. Asked if naloxone
might give users a false sense of security and thus encourage reckless drug use, Rule said, “Absolutely not — it's really
unpleasant. It initiates withdrawal with such symptoms as cramping, sweats, vomiting, chills, loose bowels, aching bones
and joints. It's like turning a switch.”
Wait a minute, we have had this program since 2001? With Good Samaritan protections? We were giving it to law
enforcement departments? There was a belief that it was important to get Naloxone in the hands of the users and
the individual homes? And Naloxone was only $1.50? What, When, Where? What have been the results, how
many lives have been saved? How many have been distributed and what has been the cost? And how many “lay
persons” have been trained to administer Naloxone? For the life of me, I cannot find one comprehensive study, date,
public comment, or promotion of this program (?) I submit that everything in this article about Naloxone getting into
the hands of the opioid users remains true today, the only thing that have changed is that the overdose death rate has
skyrocketed, Naloxone distribution in New Mexico, and in America, has lagged behind or been non-existent, and that
there have been millions and millions of dollars poured into research, education, prevention, etc. that has not produced the
results intended.
“Approximately 3,000 opioid overdose reversals were reported to the New Mexico Department of Health Harm
Reduction Program through 2013” In the United States – from 1996 through July 2010 – opioid overdose prevention
33. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 33
33
programs in 15 states (including NM) and the District of Columbia reported training and providing naloxone to 53,032
persons, resulting in 10,171 drug overdose reversals using naloxone: {22}
Really? 3,000 lives savedwith Naloxone in New Mexico, where are the press conferences? Where are the pats on the
back, much deserved? Oh, wait, read the small print, the key word is “through” 2013. Ok, so that is still an average
of 250 lives savedevery year of the program. And this also indicates, that for every 19 people trained to administer
Naloxone, and assuming they had Naloxone available, they saved1 life. And for every 5 doses of Naloxone
distributed a life was saved. Why didn’t we, as New Mexicans, or in the United States, expand this exponentially in
any of the last 15 years of this program? I cannot find this answer in New Mexico or in the United States. And
remember much of this time was before pharmaceutical companies jacked the price up, before millions and millions of
dollars, spent each and every year on often meaningless research as it relates to opioid overdose death reduction, and, still
today, without a meaningful injecting of funding for this important and proven program. Alright, now I am just
downright mad, frustrated, ashamed of us as Americans, that this has continued to epidemic proportions right
through today. And I think of my fellow New Mexico citizens, Native Americans dying each and every one of these years
at rates 2 or 3 times over the rest of us, innocent high school and college students with their whole life ahead of them gone,
the citizens of Rio Arriba County and the fallout of death in those communities, and in every other crack and crevice of
New Mexico and the United States.
And the use of real stories of people who survived an overdose, prominently told, has a power much needed now at the
community level, regional, state, and national levels. We can use the media to sell increasingly new and questionably
effective pharmaceuticals and we do not have a campaign that is killing us every year at over 50,000 people?: {20}
34. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 34
34
I am reminded of HIV/AIDS, which remains a serious issue right through today. I remember, in Indiana, when the
HIV/AIDS crisis hit, and the stigmas that were associated with it: drug users, homosexuals, etc. I remember a brave boy
stood up with his family, right there in Indiana, his name was Ryan White. He became, at least for a while, the face of the
AIDS crisis. I also remember as a kid when Walter Cronkite would, every day, list the soldiers who died in Vietnam. Who
are the faces of the opioid overdose death epidemic? The users themselves who have avoided an overdose death. And
what if, every day, we listed on National and New Mexico news, everybody we lost that day to opioid overdose abuse? We
need these faces for they educate the world that opioid overdose death can happen to anyone.
And our own New Mexico Department of Health’s State Health Improvement Plan 2014-2016, states:
“A public health, pain medication overdose prevention model based upon
multi-sector partnership (hospital EDs, County law enforcement, managed
care organizations, county health department, public insurance brokers,
boards of medicine and pharmacy) with following components: (1)
community coalition building, (2) monitoring and epidemiologic
surveillance, (3) provider education, (4) naloxone (5) project evaluation
Evidence Based
69% reduction in poisoning mortality
rate from 2009 to 2011; 15% reduction in
substance abuse and overdose-related ED
visits from 2008 to 2010 in Wilkes
County, NC
“Increase access to overdose prevention education and naloxone for persons at-risk of misuse or overdose of their
prescribed pain medication (Co-prescription Pilots).” {23}
More recently (and finally at least some data on Naloxone distribution in New Mexico):
“We’re encouraged,but we needmore naloxone than this,” saidState EpidemiologistDr.Michael Landen.“Our goal is to getall
pharmaciestostock naloxone.”…Prescriptionopioidsaccountedforabouthalf of overdose deaths.Another154 diedof heroin
35. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 35
35
overdoses. Thirty-fivepharmaciessubmitted285 Medicaidclaimsfor naloxone from Jan. 1 to March 31, up fromjust59 claimsin
the firstquarterlast year. Landennotedthatthe 35 pharmaciesthatsubmittedMedicaidclaimsaccountforonlyafractionof the
state’sapproximately 300 pharmacies. Those totalsalso pale incomparison with the 1.75 millionprescriptionsNewMexico
clinicianswrote for opioiddrugs in 2015, according to the Departmentof Healthdata.…The state isencouragingthe state’s300
pharmaciestodispense naloxonetoanyone withaprescriptionfornarcoticpainkillers. Pharmacychains WalgreensandCVS
recentlyannouncedplans to stock and dispense naloxone inNewMexico.Some Albertsonsand Smith’s Food andDrug stores
stock naloxone,and the state is innegotiationswith Walmart to encourage the company to followsuit,Landen said.The state
alsoencouragesclinicians toco-prescribe naloxone toanyone with a prescriptionfor a narcotic painkiller.For heroinusers,the
Departmentof Healthlastyeardistributed 7,186 dosesof naloxone to people enrolledinthe agency’ssyringe-exchange andharm-
reductionprograms.” {24}
“…That numbershowsthe state needstostep up effortstocurb addiction,includingbettermonitoringof prescriptionpainkillers,
accordingto state EpidemiologistDr.Michael Landen. He saidNew Mexicoalso needsto expandthe use of naloxone,a
prescriptiondrug that can counteract a drug overdose,by making it more widelyavailable to law enforcementofficersandthe
public.Far more NewMexicanscouldhave diedlastyearwithout Naloxone,whichwasusedsuccessfullyinover 900 cases…
Prescriptionopioids – narcotic painkillerssuchas hydrocodone and oxycodone – remainedthe leadingcause of overdosedeathsin
2014, accountingfornearlyhalf the total. Back-to-backdeclinesinoverdosedeathsin2012 and 2013 may have ledto complacency
about the problem,Landen said.“There was a lot of focusfor a couple of years,and I justthinksome of the focushas waned,”he
said.“We now needto redouble our efforts.” {25}
And the New Mexico Department of Human Services launches a public service campaign in 2016:
“Those huge ads on Albuquerque buses soon will include a pitch for a drug that can save lives by reversing the effects of
an overdose. Advertisements for the drug naloxone, also known by the brand-name Narcan, also will appear at other city-
owned properties, including bus shelters and community centers. The purpose of the public awareness campaign is to
encourage anyone who keeps narcotic painkillers around the house, or has a family member who uses heroin, to keepan
emergency dose of Narcan on hand. “The lifesaving potential of naloxone has not been well publicized until just
recently,” Albuquerque City Councilor Diane Gibson said at a news conference Tuesday to announce the effort. Narcan
“is available in many drug stores right now here in Bernalillo County,” Gibson said. “One of my goals is that every
pharmacy in Albuquerque will carry it very soon.” Narcan is available at 22 pharmacies in Bernalillo County, including
eight Walgreens stores, five Smith’s Food and Drug Centers, and a several independent drug stores. The city effort is
part of a statewide public awareness campaign developed by the New Mexico Department of Human Services….
Narcan “is very safe,” said Jennifer Weiss-Burke, who lost her son to a heroin overdose in 2011. “You don’t have to
worry about administering it the wrong way. You get a few minutes training on how to use it and you are good to
go.” …State officials Tuesday said they don’t know how many pharmacies stock naloxone statewide. Gov. Susana
Martinez signed a bill into law last month that expands access to naloxone by making it readily available to opioid
users as well as to their families, friends, community groups and programs. The law also shields people who
administer naloxone from civil liability or criminal prosecution. “If you have an extra glass of wine one night with your
pain meds, you might overdose,” Weiss-Burke said. “Your family needs to understand that and know what the
signs are.” {26}
Well said and well done, Ms. Weiss-Burke, and Human Services Division, a substantial forward step, almost there to
the solution… Alarming is that our state government does not know how many naloxone kits are in pharmacies in
New Mexico? Why not, are you not the distributor? Only 22 pharmacies participating in Bernalillo County, and only
36. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 36
36
35 pharmacies out of 300 in New Mexico, filing Medicaid claims for Naloxone. That’s only 10%, perhaps this should
not be optional. Perhaps it should be mandatory, Governor Martinez and the legislature, it is time to step in again.
All of this effort towards the management of opioid prescriptions but not much participation and even worst results:
Percent C hange in Filled Prescriptions, 2015 vs 2014
O pioid Products
% %
Rank State Change Rank State Change
1 South Dakota -0.7% 27 Oklahoma -6.4%
2 New Mexico -1.9% 28 South Carolina -6.4%
3 New York -2.7% 29 Kansas -6.4%
4 Nevada -3.0% 30 Vermont -6.6%
5 New Jersey -3.2% 31 Missouri -6.9%
6 Arizona -4.5% 32 Montana -7.0%
7 Colorado -4.6% 33 Hawaii -7.1%
8 Washington -4.7% 34 Maine -7.1%
9 Georgia -5.1% 35 Oregon -7.2%
10 Florida -5.3% 36 Connecticut -7.2%
11 Utah -5.3% 37 Virginia -7.3%
12 Tennessee -5.3% 38 Indiana -7.5%
13 New Hampshire -5.4% 39 Michigan -7.6%
14 Iowa -5.6% 40 Ohio -7.8%
15 North Carolina -5.6% 41 Alaska -8.1%
16 Delaware -5.6% 42 Louisiana -8.2%
17 Wyoming -5.6% 43 Massachusetts -8.2%
18 Wisconsin -5.7% 44 Minnesota -8.5%
19 Mississippi -5.7% 45 Alabama -8.6%
20 Maryland -5.8% 46 Kentucky -8.8%
21 Pennsylvania -5.8% 47 California -9.2%
22 North Dakota -5.9% 48 Rhode Island -11.0%
23 Arkansas -6.0% 49 District of Columbia -11.1%
24 Illinois -6.0% 50 Texas -11.5%
25 Nebraska -6.2% 51 West Virginia -13.1%
26 Idaho -6.3% 52 Puerto Rico N/A
{27}
It appears to me that until all pharmacies are required to participate they are not going to participate. Well, so the
past is the past, I’m sure now there is better participation, now right? So, I thought I would find out in my own backyard,
Santa Fe, New Mexico. On January 3, 2017, I went to 4 pharmacies with the following results;
37. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 37
37
Walgreen’s – Cerrillos Road
I approachedthe pharmacytechnicianandsaidI neededsome Naloxone. The technicianandtwoothersdidnotknowwhatthis
was or whatit wasfor. I educatedthemaboutopioidoverdose andwhatthislife-savingdrugwasfor. The pharmaciston duty
steppedinandstatedthat there wasa standingorderfor the drug correctlyandshowedthe technicianhow towrite aprescription
for it. I was nextaskedformy insurance coverage andIaskedif I had to have insurance togetthe drug. They saiditcouldbe sold
to me without insurance so I presentedmyPresbyterianinsurance cardandwastoldthat I couldhave 10 unitsfor$10 or 1 unitfor
$10 (?) I indicatedthatImightas well take 10! (I will be donatingthe Naloxone tothe bestlocal distribution,inmy judgement,to
getit inthe handsof usersthemselves.) Italkedwiththe pharmacistandasked,“Soif I had a guyoverdosinginthe caroutside,
wouldIhave to go throughthisprocessbefore Icouldget the Naloxone. The pharmaciststatedthathe could administeritinan
emergency. Ithenasked howmany people have come in and requestedit, eitherinanemergency,orfortheirfamily,friend, oras
a concernedcitizen, orforthemselves. The answerwas neverand obviouslythere hadnotbeenevenone case of anoverdosed
citizenbeingsavedbycomingtoWalgreens. The pharmacistcommentedthat he thought that the stigma of druguse prevents
those who needit to come and ask for it. The pharmacistindicated thatthe onlytime itisdistributediswhen the referring
physicianwhoprescribesNaloxone alongwithanopioidprescription. He saidthat sometimes the customerwill nottake the
Naloxone because theydo not want to pay the co-pay from their insurance. I was given10 one-dose vialsof Naloxone and9nasal
attachmentsformAmphastarPharmaceuticals. Itoldthe pharmacistthat the new synthetic opioids are onthe streetsnowand that
it oftenrequired2dosesof Naloxone tosave the overdosedcitizen. Iaskedif theywere givenanyinformation togive the person
requestingthe Naloxoneand he saidthere wasnone. I note the Amphastarbox has some directionsonusage butitdoesnotsay to
call 911 and getan ambulance there before orafterthe overdose citizenhasrevived. Iaskedwhatthe cost wouldbe forthe 10 vials
withoutinsurance andwastolditwouldbe $370.00 whichindicatesthatone vial wouldbe $37.00.
CVS – Cerrillos Road
I wentin to thisCVS and askedthe same questionsatthispharmacy. Theyindicatedthattheyhad some andproduceda box
containingtwovialswithnose attachments withinit, by AdaptPharma(Inote theyonlyhadone more box inthe stock inthe back
of the pharmacydesk. The pharmacy technicianlookedupthe directionsonhow todo the Narcan purchase. She indicatedif Ihad
38. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 38
38
insurance the costof the Naloxone wouldbe $37.50 but if not,$116.00. I askedif theyhadanybodyaskedforNaloxone fora family
memberfriend,orasconcernedcitizenandtheysaidtheydidnot. I askedwhatwouldhappenif Ihad an overdose victimoutsidein
the car, couldtheyjustgive me a vial to save hislife? The pharmacistindicatedthathe wouldbe able toadministerthe Naloxonein
an emergencybutIeitherhadto buyit withor withoutinsurance. The pharmacy technician saidtheyhadjuststartedthe program
and were notfamiliarwithit. Iaskedif theywere givenany informationto provide withthe Naloxone and they saidthey didnot.
I note the Amphastarbox had much betterinstructions, includingcalling911. I againeducatedthemaboutopioidabuse andthe
newmore powerful syntheticopioidsthatare hittingthe streets. TheyindicatedthattheirCVSinstructionssell the two-vialsetat
$109.00 withoutinsurance andthattheyhada couponfor$35.00 if I had insurance (?). WhenItriedto use myPresbyterian
Hospital intheirsystem,she indicatedthatthe Naloxonewasnotan approvedmedicationundermyplan(?).
Highland Pharmacy (Across from Saint Vincent’s Hospital)
I wentto thispharmacyand theysaidtheyhad Naloxone. The technicianindicatedthattheydidnothave anyinstock but she could
getit the nextday. She indicatedthattheyusedthe AlphaPharmanaloxone two-pack. She indicatedthatshe hasneverhad
anyone requestNaloxone forthemselvesorothersandthat if there wassomeone needingitoverdosingoutside,thatthe St.
Vincent’sEmergencyRoom wasacross the street.
Del Norte Pharmacy – Galisteo Street
The pharmacy staff here knowthe most about Naloxone andthe pharmacistindicatedthattheydidnothave anyinstock because
the pharmaceutical provider,Amphastar,haddefective sprayers,andthe companyremovedall of themfromthe market. She
statedthat theirorderhas beenbackorderedformonthsandtheyhave none. Again,I educatedthemaboutthe needfortwovials
perkit andtheyindicatedthatthe Amphastarbox has twovials, showingme abox. Unfortunately,theyare incorrect,there isonlya
single vial inthe Amphastarboxes. Theygave me instructionsforthe Naloxone,aone page copiedsheetof paper, whichtheysaid
theyreceivedfromthe SouthwestCare CenterinSantaFe. Theyhave no ideawhentheywill be gettinganymore Naloxone.
Smith’s Pharmacy – Pacheco Street
I talkedwiththe pharmacytechnicianhere whoindicatedthattheyhadNaloxone ‘samples”whichwere providedbythe Southwest
Care Centerinthe summerof 2016 but theyhadto destroythese samplesbecausetheyexpiredinJanuary2017. Theyhave not
receivedanymore naloxone,have none available, andhadnotorderedanyfromany source. She indicatedthat theyhave nobody
asking for it and have had nobody approach themwith an overdose emergencyeither. {28}
SouthwestCare Centerisfundedbythe Behavioral HealthDivisionof the Departmentof HumanServices to:
“The Behavioral Health Services Division(BHSD) contracts with SWCARE to provide technical assistance to pharmaciesrelated to naloxone. The goalis to increase
access to naloxone byincreasing the number of pharmacists credentialed to dispense naloxone, increase patient outreachandeducation about naloxone, and
reduce pharmacybarriers to dispensingandbillingfor naloxone. Increasingaccessto naloxone is a strategyrecommendedbythe Centers for Disease Control and
Prevention(http://www.cdc.gov/vitalsigns/heroin/).
In addition to other communityprevention efforts BHSDOffice of Substance Abuse and Prevention(OSAP) also oversees twopublic awareness campaigns:
Increasing public awareness of, and access to naloxone througha media campaign consisting of radio public service announcements, newsprint ads, billboards,
and a resource website (http://doseofrealitynm.com/2015/08/31/more-info-aboutnaloxone/)
Increasing public awareness of the dangers of prescriptiondrug abuse through“A Dose of Reality” media campaign consisting o f radio public service
announcements, TV ads, newsprint ads, billboards, social media, movie theater ads, andresource website ( http://www.nmprevention.org/Dose-of-
Reality/Home.html).”
39. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 39
39
And they are award-winning for their “Dose of Reality” campaign, an award, really?
“The New MexicoHuman Services Department’s (HSD)campaignto raise awareness of prescriptiondrugabuse, called , A Dose of Reality, has beenawardedthe
2015 Silver Cumbre Award for public service campaigns from the New Mexicochapter of the Public Relations Societyof America.”
As part of the campaign, three commercials designed to capture teens’ attentionappear onyouth-orientedprogramming onComcast, YouTube, movie theaters,
malls, billboards andgas pumps. Additionally, weeklyposts are aimed directlyat teens on Instagramwith combinations ofcommonhashtags kids use to research
and share information about gettinghigh. Advertisements onpharmaceuticaldrugbags promote safe storage andproper disposal, as wellas a parent resource
toolkit. All materials are available for downloadat Susana Martinez, Governor Brent Earnest, Secretaryat http://www.adoseofrealitynm.comfor use byparents
and communitymembers working onprevention. The campaignwill also be featured inanupcoming“Better Call Saul” episode. The campaign is beingfundedby
a grant from the federal Substance Abuse andMental Health Administration(SAMHSA) Center for Substance Abuse Prevention(CSAP). The Cumbre Awards
recognize outstandingstrategic public relations campaigns andtactics byNew Mexico’s communications professionals. {29}
While I understand the need to educate our youth about prescription overdoses, and their rate, especially among
females is rising, the mass amount of prescription overdoses is not with youth. Why wasn’t this campaign aimed at
the 75%+ of the New Mexico population who are overdosing? And again, has it been effective, have the overdose
death rates gone down? And how many Naloxone units did they actually distribute? Are they everplanning on
distributing some more? For Santa Fe pharmacies, and perhaps all 300 New Mexico pharmacies, certainly need
some along with education about what Naloxone is evenfor.
Southwest Care’s main thrust appears to be HIV/AIDS/Hepatitis, prevention and treatment. While, of course, related to
opioid abusers who contract these conditions as well, their website has no information on Naloxone, anywhere, yet they
are funded by the New Mexico Human Services Division for this purpose. {30}
I found they offered a training session in 2016:
Southwest CARE Center, with funding from the Behavior Health Services Division in New Mexico:
Invite you and your Staff …
“A Dose of Rxeality- You Can Be Part of the Solution!Campaign”
Presentedby:
Karen Clark, PharmD, Staff Pharmacist, Southwest CARE Center, Albuquerque, NM
Carly Cloud Floyd, PharmD, PhC, CACP, AAHIVP, Pharmacy Manager, Clinical Pharmacist, Southwest CARE Center, Albuquerque, NM
Kate Morton, PharmD, Director of Pharmacy, Southwest CARE Center, Santa Fe, NM
Craig Schaefer, CPhT, Pharmacy Specialist, Southwest CARE Center, Santa Fe, NM
Date: Monday, May 2, 2016
Place: Southwest CARE Center – 649 Harkle Rd. NE, Santa Fe
Times: Call or email to confirm times or to schedule futuretraining dates.
RSVP: Contact Kate Morton @ 505-989-8154 orkmorton@southwestcare.org
* Pre-Registration is required to guarantee your seat.
40. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 40
40
RPh Objectives # 0104-9999-16-028-L01-P CPhT Objectives # 0104-9999-16-028-L01-T
By the end of this presentation, pharmacists will be able to: Reviewthe
2016 updatedlaw regardingpharmacist naloxone prescriptive authority
and Department ofHealthstanding order
By the end of this presentation, pharmacy technicians will be able to:
Reviewthe 2016 updatedlaw regardingpharmacist naloxone prescriptive
authorityandDepartment of Healthstanding order andhowthis affects
technicians in an outpatient pharmacysetting
Describe the different groups of people that come into the pharmacy
who should receive naloxone
Identifygoodcandidatesfor naloxone at the drop-off andpick-up
windows, or byreviewing prescription profiles
Properlyandefficientlyadjudicate a claimfor naloxone
Properlyandefficientlyadjudicate a Medicaid claimfor naloxone
Effectivelyandefficientlycounsel a patient andfamilymembers on
harm reductionstrategiesandnaloxone use byusing the demo kit(s)
provided
Identifyappropriate vendors for naloxone and mucosal nasal adaptors
The New Mexico Pharmacists Association is accredited by the Accreditation Council for Pharmacy
Education (ACPE) as a provider of continuing pharmacy education. This program provides 2.0 contact
hours (0.2 CEUs) of continuing pharmacy education credit. The knowledge-based program is designed for
pharmacists & pharmacy technicians. Participants are required to turn in a completed program evaluation form
to receive the designated CEUs. Your CPE credits will be submitted into the CPE Monitor Database within 60 days
based on the information provided.
ACPE Program # 0104-9999-16-028-L01-P/T/ Initial Release Date: 5/02/16
And they are recognized as innovative in Naloxone distribution expansion:
“Theincrease in naloxone access can be attributed in large part to a novel pharmacist-initiated naloxone program. Since April, a group of pharmacists who are part
of a nonprofit HIV/Hepatitis C clinic in New Mexico has been traveling to pharmacies in the state to train pharmacists to operatea naloxone program. “Even
though we have this law in New Mexico, we didn’t see claims increase for naloxone, so we felt we needed hands-on training for pharmacists and technicians,” said
Kate Morton, PharmD, director of Pharmacy Services of Southwest CARE Center, thenonprofit that provides the onsite training. She said many pharmacists
intended to take advantage of the law but didn’t know how to develop a program or were too strapped for time to get one started. Providing hands-on, peer-to-peer
training seemed like the most effective tactic, according to Morton. “Peopleare really appreciative that we’ve come to them and taken thetime, especially in the
more rural towns,”Morton told Pharmacy Today.” {31}
And Ms. Morton writes, in her own editorial:
“Since April, nearly 200 outpatient pharmacists and their staff, representing more than 43 pharmacies in 20 communities throughout thestate, have been trained on
how to use patient demonstration kits and how to prescribe lifesaving naloxone to patients with an opioid painkiller prescrip tion or their family members. Newlaws
allowing for easierdistribution of naloxone, including the naloxone prescription orderfrom New Mexico’s Department of Health, have seen an increase in
the number of Medicaid claims for naloxone. More than 77 pharmacies and 160,000 patients receivedtheirprescriptions in pharmacy bags with the Dose
of Reality campaign message to promote the lifesaving benefit of naloxone. Collaboration must continue at thelocal and statelevel. The New Mexico
Behavioral Health Services Division and the stateDepartment of Health have received four federal grants to raise awareness about the dangers of sharing
prescription drugs and reducing opioid overdose deaths, and expanding naloxone distribution andtraining first responders in high-needcommunities. This
is the right direction for all of us. Accidental opioid overdose can happen to anyone. Protect your family by asking your pharmacist today about naloxone.
{32}
It is apparent that the Naloxone distribution strategy providing it in pharmacies, is an utter failure and always has been, I
note the following problems and considerations with this strategy:
41. REDUCING OPIOID OVERDOSE DEATHS IN THE UNITED STATES & NEW MEXICO 41
41
1. There appears to be no continuous source to even get Naloxone stocked in 3 out of the 5 pharmacies in Santa Fe,
with another pharmacy only having two boxes available. One pharmacy could get in 24 hours; another had been
given samples that expired 6 months later with no replenishment of their inventory. And no pharmacy had any
examples of anyone coming and wanting it as an emergency with someone overdosing nearby. If that did happen,
the pharmacists agreed that they could administer the Naloxone themselves.
2. The fact that a person must have insurance to get Naloxone meant a copay anywhere from a $1 a single dose vial
up to $37.00 for a single use vial. For a double-vial pack, one pharmacy had it for $37.00 with insurance and
$116.00 without insurance. So, the cost per 2 does vial ranges from $2 to $37.00 if you have insurance. They only
apparent time that it has been distributed was as a separate prescription by a prescribing doctor who was giving the
patient an opioid prescription in tandem. And it appears that at least some of these customers have refused to pay
the copay for the Naloxone, taking only the opioid prescription.
3. There has been little to no education of the pharmacy staff on the problem of overdose death in New Mexico nor
about the synthetic opioids requiring two vials to revive the overdosing citizen.
4. There is no marketing of Naloxone with any signs or indication that Naloxone is evenavailable. So, nothing
like a poster that might say “Have a friend with an opioid problem?” and a description of the various opioids
including heroin and fentanyl, and the need for two vials. And some information about the cost of it with Medicaid
and conventional insurance coverage would also be important.
5. Nobody is coming in and asking for Naloxone, for those that have it prescribed and have insurance, at least some
won’t even pay a copay for Naloxone. Few claims for Medicaid for Naloxone are being filled. There is a stigma
with asking for Naloxone in a pharmacy setting.
6. There is no tracking and distribution management of the Naloxone. For example, if some of the Naloxone was
expiring in 6 months, that should be pulled from the shelves, and immediately distributed at the street level, where
it could be used the fastest, and before it expired.