
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Facial nerve palsy.pptx
Semelhante a Facial nerve palsy.pptx (20)
Mais de Rohit Paswan
Mais de Rohit Paswan (20)
Último
Último (20)
Facial nerve palsy.pptx
- 1. FACIAL NERVE PALSY DEPARTMENT : ENT- HNS NMCTH , BIRGUNJ DATE : 2079-02-15 DAY : SUNDAY
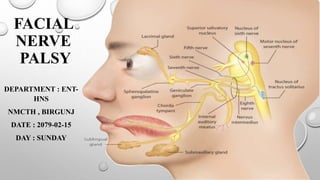
- 2. ANATOMY AND FUNCTIONS OF FACIAL NERVE Facial Nerve Runs From Pons To Parotid. It Is A Mixed Nerve Having Motor And A Sensory Root. The Latter Is Also Called The Nerve Of Wrisberg And Carries Secretomotor Fibres To The Lacrimal Gland And Salivary Glands, And Brings Fibres Of Taste And General Sensation. Thus There Are Two Efferent And Two Afferent Pathways.
- 3. COMPONENTS OF THE FACIAL NERVE INCLUDE: 1. Special Visceral Efferent Forms The Motor Root And Supplies All The Muscles Derived From The Second Branchial Arch, I.E. All The Muscles Of Facial Expression, Auricular Muscles (Now Vestigial), Stylohyoid, Posterior Belly Of Digastric And The Stapedius. 2. General Visceral Efferent Supplies Secretomotor Fibres To Lacrimal, Submandibular And Sublingual Glands And The Smaller Secretory Glands In The Nasal Mucosa And The Palate. 3. Special Visceral Afferent Brings Taste From The Anterior Two-thirds Of Tongue Via Chorda Tympani And Soft And Hard Palate Via Greater Superficial Petrosal Nerve. Taste Is Carried To The Nucleus Of Tractus Solitarius. 4. General Somatic Afferent Brings General Sensation From The Concha, Posterosuperior Part Of External Canal And The Tympanic Membrane. These Fibres Account For Vesicular Eruption In Herpes Zoster Infection Of The Geniculate Ganglion. It Also Brings Proprioceptive Sensation From The Facial Muscles.
- 4. NUCLEUS OF FACIAL NERVE
- 5. COURSE OF FACIAL NERVE Motor fibres take origin from the nucleus of VIIth nerve, hook round the nucleus of VIth nerve and are joined by the sensory root (nerve of wrisberg). Facial nerve leaves the brainstem at pontomedullary junction, travels through posterior cranial fossa and enters the internal acoustic meatus. At the fundus of the meatus (lateral most part of meatus), the nerve enters the bony facial canal, traverses the temporal bone and comes out of the stylomastoid foramen. Here it crosses the styloid process and divides into terminal branches. Intratemporal part consists of four segments: Meatal (1), Labyrinthine (2), Tympanic (3) and Mastoid (4).
- 6. THE COURSE OF THE NERVE CAN THUS BE DIVIDED INTO THREE PARTS. 1. INTRACRANIAL PART. From pons to internal acoustic meatus (15–17 mm). 2. INTRATEMPORAL PART. From internal acoustic meatus to stylomastoid foramen. It is further divided into: (A) MEATAL SEGMENT (8–10 MM). Within internal acoustic meatus. (B) LABYRINTHINE SEGMENT (4.0 MM). From fundus of meatus to the geniculate ganglion where nerve takes a turn posteriorly forming a “genu.” The nerve in the labyrinthine segment has the narrowest diameter (0.61–0.68 mm) and the bony canal in this segment is also the narrowest. This is also the shortest segment of the nerve. (C) TYMPANIC OR HORIZONTAL SEGMENT (11.0 MM). From geniculate ganglion to just above the pyramidal eminence. It lies above the oval window and below the lateral semicircular canal. (D) MASTOID OR VERTICAL SEGMENT (13.0 MM). From the pyramid to stylomastoid foramen. Between the tympanic and mastoid segments is the second genu of the nerve. 3. EXTRACRANIAL PART. From stylomastoid foramen to the termination of its peripheral branches.
- 7. BRANCHES OF FACIAL NERVE 1. GREATER SUPERFICIAL PETROSAL NERVE. It arises from geniculate ganglion and carries secretomotor fibres to lacrimal gland and the glands of nasal mucosa and palate. 2. NERVE TO STAPEDIUS. It arises at the level of second genu and supplies the stapedius muscle. 3. CHORDA TYMPANI. It arises from the middle of vertical segment, passes between the incus and neck of malleus, And leaves the tympanic cavity through petrotympanic fissure. It carries secretomotor fibres to submandibular And sublingual glands and brings taste from anterior two thirds of tongue. 4. COMMUNICATING BRANCH. It joins auricular branch of vagus and supplies the concha, retroauricular groove, posterior meatus and the outer surface of tympanic membrane. 5. POSTERIOR AURICULAR NERVE. It supplies muscles of pinna, occipital belly of occipitofrontalis and communicates with auricular branch of vagus. 6. MUSCULAR BRANCHES. To stylohyoid and posterior belly of digastric. 7. PERIPHERAL BRANCHES. The nerve trunk, after crossing the styloid process, forms two divisions, an upper temporofacial and a lower cervicofacial, which further divide into smaller branches. These are the temporal, zygomatic, buccal, mandibular and cervical and together form pes anserinus (goose-foot). They supply all the muscles of facial expression.
- 10. BLOOD SUPLY OF FACIAL NERVE BLOOD SUPPLY OF FACIAL NERVE. (1) CEREBELLOPONTINE ANGLE: ANTERIOR-INFERIOR CEREBELLAR ARTERY. (2) INTERNAL AUDITORY CANAL: LABYRINTHINE ARTERY. (3) GENICULATE GANGLION AND ADJACENT FACIAL NERVE: SUPERFICIAL PETROSAL. (4) MASTOID SEGMENT: STYLOMASTOID ARTERY. THUS BOTH CAROTID AND VERTEBROBASILAR SYSTEMS SUPPLY THE NERVE AND MEET AT LABYRINTHINE SEGMENT. ALL THE ARTERIES FORM AN EXTERNAL PLEXUS WHICH LIES IN THE EPINEURIUM AND FEEDS A DEEPER INTRANEURAL INTERNAL PLEXUS
- 11. SURGICAL LANDMARKS OF FACIAL NERVE FOR MIDDLE EAR AND MASTOID SURGERY 1. PROCESSUS COCHLEARIFORMIS. IT DEMARCATES THE GENICULATE GANGLION WHICH LIES JUST ANTERIOR TO IT. TYMPANIC SEGMENT OF THE NERVE STARTS AT THIS LEVEL. 2. OVAL WINDOW AND HORIZONTAL CANAL. THE FACIAL NERVE RUNS ABOVE THE OVAL WINDOW (STAPES) AND BELOW THE HORIZONTAL CANAL. 3. SHORT PROCESS OF INCUS. FACIAL NERVE LIES MEDIAL TO THE SHORT PROCESS OF INCUS AT THE LEVEL OF ADITUS. 4. PYRAMID. NERVE RUNS BEHIND THE PYRAMID AND THE POSTERIOR TYMPANIC SULCUS. 5. TYMPANOMASTOID SUTURE. IN VERTICAL OR MASTOID SEGMENT, NERVE RUNS BEHIND THIS SUTURE. 6. DIGASTRIC RIDGE. THE NERVE LEAVES THE MASTOID AT THE ANTERIOR END OF DIGASTRIC RIDGE.
- 12. FOR PAROTID SURGERY 1. Cartilaginous pointer. The nerve lies 1 cm deep and slightly anterior and inferior to the pointer. Cartilaginous pointer is a sharp triangular piece of cartilage of the pinna and “points” to the nerve. 2. Tympanomastoid suture. Nerve lies 6–8 mm deep to this suture. 3. Styloid process. The nerve crosses lateral to styloid process. 4. Posterior belly of digastric. If posterior belly of digastric muscle is traced backwards along its upper border to its attachment to the digastric groove, nerve is found to lie between it and the styloid process. SURGICAL LANDMARKS OF FACIAL NERVE CONTD..
- 13. VARIATIONS AND ABNORMALITIES IN THE COURSE OF FACIAL NERVE. (A)NORMAL, (B) BONY DEHISCENCE, (C) HUMP POSTERIORLY (NEAR THE SECOND GENU), (D)BIFURCATION, (E) TRIFURCATION, (F) BIFURCATING AND REUNITING ROUND THE OVAL WINDOW AND (G)THE NERVE PASSING BETWEEN THE OVAL AND ROUND WINDOWS.
- 14. STRUCTURE OF NERVE From inside out, a nerve fibre consists of axon, myelin sheath, neurilemma and endoneurium. A group of nerve fibres is enclosed in a sheath called perineurium to form a fascicle and the fascicles are bound together by epineurium
- 15. SEVERITY OF NERVE INJURY Degree of nerve injury will determine the regeneration of nerve and its function. Earlier nerve injuries were divided into: 1. Neurapraxia, a conduction block, where flow of axoplasm through the axons was partially obstructed. 2. Axonotmesis—injury to axons. 3. Neurotmesis—injury to nerve.
- 16. Sunderland classified nerve injuries into five degrees of severity based on anatomical structure of the nerve and This classification is now widely accepted. 1°= Partial block to flow of axoplasm; no morphological changes are seen. Recovery of function is complete (Neurapraxia). 2°= Loss of axons, but endoneurial tubes remain intact. During recovery, axons will grow into their respective Tubes, and the result is good (axonotmesis). 3°= Injury to endoneurium. During recovery, axons of one tube can grow into another. Synkinesis can occur (Neurotmesis). 4°= Injury to perineurium in addition to above. Scarring will impair regeneration of fibres (partial transection). 5°= Injury to epineurium in addition to above (complete nerve transection). The first three degrees are seen in viral and inflammatory disorders while fourth and fifth are seen in surgical or accidental trauma to the nerve or in neoplasms. SEVERITY OF NERVE INJURY
- 17. ELECTRODIAGNOSTIC TESTS THESE TESTS ARE USEFUL TO DIFFERENTIATE BETWEEN NEURAPRAXIAAND DEGENERATION OF THE NERVE. THEY ALSO HELP TO PREDICT PROGNOSIS AND INDICATE TIME FOR SURGICAL DECOMPRESSION OF THE NERVE. 1. MINIMAL NERVE EXCITABILITY TEST. 2. MAXIMAL STIMULATION TEST (MST). 3. ELECTRONEURONOGRAPHY (ENOG) 4. ELECTROMYOGRAPHY (EMG).
- 18. CAUSES OF FACIAL PARALYSIS The cause may be central or peripheral. The peripheral lesion may involve the nerve in its intracranial, intratemporal or extratemporal parts. Peripheral lesions are more common and about two-thirds of them are of the idiopathic variety • CENTRAL • BRAIN ABSCESS • PONTINE GLIOMAS • POLIOMYELITIS • MULTIPLE SCLEROSIS • INTRACRANIAL PART (CEREBELLOPONTINE ANGLE) • ACOUSTIC NEUROMA • MENINGIOMA • CONGENITAL CHOLESTEATOMA • METASTATIC CARCINOMA • MENINGITIS
- 19. • INTRATEMPORAL PART • IDIOPATHIC – BELL PALSY – MELKERSSON SYNDROME • INFECTIONS – ACUTE SUPPURATIVE OTITIS MEDIA – CHRONIC SUPPURATIVE OTITIS MEDIA – HERPES ZOSTER OTICUS – MALIGNANT OTITIS EXTERNA • TRAUMA – SURGICAL: MASTOIDECTOMY AND STAPEDECTOMY – ACCIDENTAL: FRACTURES OF TEMPORAL BONE • NEOPLASMS – MALIGNANCIES OF EXTERNAL AND MIDDLE EAR – GLOMUS TUMOUR – FACIAL NERVE NEUROMA – METASTASIS TO TEMPORAL BONE (FROM CANCER OF BREAST, BRONCHUS, PROSTATE) CAUSES OF FACIAL PARALYSIS CONTD.
- 20. CAUSES OF FACIAL PARALYSIS CONTD. • EXTRACRANIAL PART • MALIGNANCY OF PAROTID • SURGERY OF PAROTID • ACCIDENTAL INJURY IN PAROTID REGION • NEONATAL FACIAL INJURY (OBSTETRICAL FORCEPS) • SYSTEMIC DISEASES • DIABETES MELLITUS • HYPOTHYROIDISM • URAEMIA • POLYARTERITIS NODOSA • WEGENER’S GRANULOMATOSIS • SARCOIDOSIS (HEERFORDT’S SYNDROME) • LEPROSY • LEUKAEMIA • DEMYELINATING DISEASE
- 21. LOCALIZATION OF FACIAL LESION A. CENTRAL FACIAL PARALYSIS It is caused by cerebrovascular accidents (haemorrhage, thrombosis or embolism), tumour or an abscess. It causes paralysis of only the lower half of face on the contralateral side. Forehead movements are retained due to bilateral innervation of frontalis muscle. Involuntary emotional movements and the tone of facial muscles are also retained. B. PERIPHERAL FACIAL PARALYSIS All the muscles of the face on the involved side are paralyzed. Patient is unable to frown, close the eye, purse the lips or whistle. A lesion at the level of nucleus is identified by associated paralysis of VIIth nerve. A lesion at cerebellopontine angle is identified by the presence of vestibular and auditory defects and involvement of other cranial nerves such as Vth, IXth, Xth and XIth. A lesion in the bony canal, from internal acoustic meatus to stylomastoid foramen, can be localized by topodiagnostic tests. A lesion outside the temporal bone, in the parotid area, affects only the motor functions of nerve. It may sometimes be incomplete as some branches of the nerve may not be involved in tumour or trauma.
- 22. TOPODIAGNOSTIC TESTS FOR LESIONS IN INTRATEMPORAL PART THE FOLLOWING TESTS ARE USEFUL IN FINDING THE SITE OF LESION IN PARALYSIS OF LOWER MOTOR NEURON. 1. SCHIRMER TEST. 2. STAPEDIAL REFLEX. (TYMPANOMETRY) 3. TASTE TEST. 4. SUBMANDIBULAR SALIVARY FLOW TEST.
- 23. COMPLICATIONS FOLLOWING FACIAL PARALYSIS Peripheral facial paralysis due to any cause may result in any of the following complications: 1. INCOMPLETE RECOVERY. 2. EXPOSURE KERATITIS. 3. SYNKINESIS (MASS MOVEMENT). 4. TICS AND SPASMS. 5. CONTRACTURES. 6. CROCODILE TEARS (GUSTATORY LACRIMATION). 7. FREY’S SYNDROME (GUSTATORY SWEATING). 8. PSYCHOLOGICALAND SOCIAL PROBLEMS.
- 24. HYPERKINETIC DISORDERS OF FACIAL NERVE They are characterized by involuntary twitching of facial muscles on one or both sides. 1. HEMIFACIAL SPASM. It is characterized by repeated, uncontrollable twitchings of facial muscles on one side . it is of two types (I) essential or idiopathic, where cause is not known and (ii) secondary, where cause is acoustic neuroma, congenital cholesteatoma or glomus tumour. Many cases of hemifacial spasm are due to irritation of the nerve because of a vascular loop at the cerebellopontine angle. Microvascular decompression through posterior fossa craniotomy has met with high success rate in these cases. Idiopathic type has been treated by selective section of the branches of facial nerve in the parotid or by puncturing the facial nerve with A needle in its tympanic segment. Botulinum toxin has been used in the affected muscle. It blocks the neuromuscular junction by preventing release of acetylcholine. 2. BLEPHAROSPASM. Twitchings and spasms are limited to orbiculars oculi muscles on both sides. The eyes are closed due to muscle spasms causing functional blindness. The cause is uncertain, but probably lies in the basal ganglia. It is treated by selective section of nerves supplying muscles around the eye on both sides. Botulinum-a toxin injected into the periorbital muscles gives relief for 3–6 months. Injection can be repeated, if necessary.
- 25. Hemifacial spasm. Note all the facial muscles and platysma in the spasm. Picture taken during paroxysm of clonic contractions.
- 26. SURGERY OF FACIAL NERVE 1. DECOMPRESSION. 2. END-TO-END ANASTOMOSIS. 3. NERVE GRAFT (CABLE GRAFT). 4. HYPOGLOSSAL-FACIAL ANASTOMOSIS. 5. PLASTIC PROCEDURES.
- 27. 1. BELL’S PALSY Introduction Sixty to seventy-five per cent of facial paralysis is due to bell’s palsy. It is defined as idiopathic, peripheral facial paralysis or paresis of acute onset. Both sexes are affected with equal frequency. Any age group may be affected though incidence rises with increasing age. A positive family history is present in 6–8% of patients. Risk of bell palsy is more in diabetics (angiopathy) and pregnant women (retention of fluid). Facial paralysis left side. Compare it with normal side. CLINICAL CORRELATION
- 28. AETIOLOGY 1. Viral infection. : Herpes simplex, herpes zoster or the Epstein–barr virus. 2. Vascular ischaemia. 3. Hereditary. Ten percent of the cases of bell palsy have a positive family history. 4. Autoimmune disorder. T-lymphocyte changes have been observed.
- 29. Clinical features. • Onset is sudden. • Patient is unable to close his eye. On attempting to close the eye, eyeball turns up and out (bell phenomenon). • Saliva dribbles from the angle of mouth. • Face becomes asymmetrical. • Tears flow down from the eye (epiphora). • Pain in the ear may precede or accompany the nerve paralysis. • Some complain of noise intolerance (Stapedial paralysis) or loss of taste (involvement of chorda Tympani). • Paralysis may be complete or incomplete. • Bell palsy is recurrent in 3–10% of patients. Facial paralysis left side. Compare it with normal side.
- 30. Diagnosis Diagnosis is always by exclusion. All other Known causes of peripheral facial paralysis should be excluded. This requires careful history, complete otological And head and neck examination, x-ray studies, blood Tests such as total count, peripheral smear, sedimentation Rate, blood sugar and serology. Nerve excitability tests are done daily or on alternate Days and compared with the normal side to monitor Nerve degeneration. Localizing the site of lesion (topodiagnosis) helps in Establishing the aetiology and also the site of surgical decompression Of nerve, if that becomes necessary.
- 31. Treatment General 1. Reassurance. 2. Relief of ear pain by analgesics. 3. Care of the eye Eye must be protected Against exposure keratitis. 4. Physiotherapy or massage of the facial muscles gives Psychological support to the patient. It has not been Shown to influence recovery. Active facial movements Are encouraged when there is return of some movement To the facial muscles.
- 32. Medical management STEROIDS. Prednisolone is the drug of choice. If patient reports within 1 week, the adult dose of prednisolone is 1 mg/kg/day divided into morning and evening doses for 5 days. Patient is seen on the fifth day. If paralysis is incomplete or is recovering, dose is tapered during the next 5 days. If paralysis remains complete, the same dose is continued for another 10 days and thereafter tapered in next 5 days (total of 20 days). Contraindications to use of steroids include pregnancy, diabetes, hypertension, peptic ulcer, pulmonary tuberculosis and glaucoma. Steroids have been found useful to prevent incidence of synkinesis, crocodile tears and to shorten the recovery time of facial paralysis. Steroids can be combined with acyclovir for herpes zoster oticus or bell palsy. OTHER DRUGS. Vasodilators, vitamins, mast cell inhibitors And antihistaminics have not been found useful.
- 33. SURGICAL TREATMENT Nerve decompression relieves pressure on the nerve fibres and thus improves the microcirculation of the nerve. Vertical and tympanic segments of nerve are decompressed. PROGNOSIS. Eighty-five to ninety per cent of the patients recover fully. Ten to fifteen per cent recover incompletely and may be left with some stigmata of degeneration. Recurrent facial palsy may not recover fully. Prognosis is good in incomplete bell palsy (95% complete recovery) and in those where clinical recovery starts within 3 weeks of onset (75% complete recovery).
- 34. 2. MELKERSSON SYNDROME It is also an idiopathic disorder consisting of a triad of facial paralysis, swelling of lips and fissured tongue. Paralysis may be recurrent. Treatment is the same as for bell palsy. • Recurrent facial palsy. Recurrent facial palsy is seen in bell palsy (3–10% cases), melkersson syndrome, diabetes, sarcoidosis and tumours. Recurrent palsy on the same side may be caused by a tumour in 30% of cases. • Bilateral facial paralysis. Simultaneous bilateral facial paralysis may be seen in guillain-barré syndrome, sarcoidosis, sickle cell disease, acute leukaemia, bulbar Palsy, leprosy and some other systemic disorders.
- 35. 3. HERPES ZOSTER OTICUS (RAMSAY–HUNT SYNDROME) There is facial paralysis along with vesicular rash in the External auditory canal and pinna. There May also be anaesthesia of face, giddiness and hearing Impairment due to involvement of Vth and VIIIth nerves. Treatment is the same as for bell palsy.