Multiple sclerosis (MS)
•
15 gostaram•8,198 visualizações

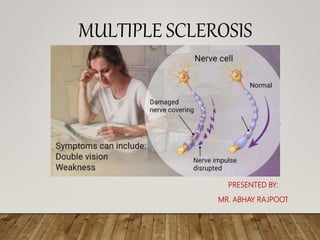
Multiple sclerosis (MS) is a potentially disabling disease of the brain and spinal cord (central nervous system). In MS , the immune system attacks the protective sheath (myelin) that covers nerve fibers and causes communication problems between your brain and the rest of your body.

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Multiple sclerosis (MS)
Semelhante a Multiple sclerosis (MS) (20)
Mais de Abhay Rajpoot
Mais de Abhay Rajpoot (20)
Último
Último (20)
Multiple sclerosis (MS)
- 1. MULTIPLE SCLEROSIS PRESENTED BY: MR. ABHAY RAJPOOT
- 2. NEURON CELL The billions of neurons, or nerve cells, that underlie all the activity of the nervous system form a communication network that coordinates all the systems of the body and enables them to function. Neurons usually receive messages from other neurons through short fibers, called dendrites, that pick up messages and carry them to the neuron's cell body. The axon carries outgoing messages from the cell. A group of axons bundled together makes up a nerve. Some axons are covered with a myelin sheath, made up of glial cells. The myelin sheath increases neuron efficiency and provides insulation.
- 4. INTRODUCTION Multiple sclerosis (MS) is a potentially disabling disease of the brain and spinal cord (central nervous system). In MS, the immune system attacks the protective sheath (myelin) that covers nerve fibers and causes communication problems between your brain and the rest of your body. Eventually, the disease can cause permanent damage or deterioration of the nerves.
- 5. MULTIPLE SCLEROSIS MS is a chronic demyelinating disease that affects the myelin sheath of neurons in the central nervous system ( brain, optic nerve & spinal cord). • Incidence: • App. 4 lakh people in US have MS. • Females are affected two times more than males. • The incidence is highest in young adults. • Whites are affected more common than hispanics.
- 8. RISK FACTORS: • Age. MS can occur at any age, but usually affects people somewhere between the ages of 16 and 55. •Sex. Women are more than two to three times as likely as men are to have relapsing- remitting MS. •Family history. If one of your parents or siblings has had MS, you are at higher risk of developing the disease. •Certain infections. A variety of viruses have been linked to MS, including Epstein- Barr, the virus that causes infectious mononucleosis. •Vitamin D. Having low levels of vitamin D and low exposure to sunlight is associated with a greater risk of MS. •Certain autoimmune diseases •Smoking
- 9. ETIOLOGY : The cause of multiple sclerosis is unknown. It's considered an autoimmune disease in which the body's immune system attacks its own tissues. In the case of MS, this immune system malfunction destroys the fatty substance that coats and protects nerve fibers in the brain and spinal cord (myelin)
- 10. CLASSIFICATION: • Relapsing-Remitting MS (RRMS). This is the most common form of multiple sclerosis. About 85% of people with MS are initially diagnosed with RRMS. People with RRMS have temporary periods called relapses, flare-ups or exacerbations, when new symptoms appear • Secondary-Progressive MS (SPMS). In SPMS, symptoms worsen more steadily over time, with or without the occurrence of relapses and remissions. Most people who are diagnosed with RRMS will transition to SPMS at some point • Primary-Progressive MS (PPMS). This type of MS is not very common, occurring in about 10% of people with MS. PPMS is characterized by slowly worsening symptoms from the beginning, with no relapses or remissions • Progressive-Relapsing MS (PRMS). A rare form of MS (5%), PRMS is characterized by a steadily worsening disease state from the beginning, with acute relapses but no remissions, with or without recovery
- 11. PATHOPHYSIOLOGY: Due to etiological factors Activated T cells which recognize self-antigens expressed in the CNS& macrophages enters the brain the peripheral circulation & initiate the inflammation Production of inflammatory cytokines & reactive oxygen species, activated T lymphocytes & microphages Demyelination & destruction of oligodendrocytes Formation of plaques along the myelin sheath Scarring & destruction of myelin sheath (commonly occurs at optic nerve,
- 12. CLINICAL MANIFESTATION: • Numbness or weakness in one or more limbs that typically occurs on one side of your body at a time, or the legs and trunk • Electric-shock sensations that occur with certain neck movements, especially bending the neck forward (Lhermitte sign) • Tremor, lack of coordination or unsteady gait • Vision problems are also common, including: • Partial or complete loss of vision, usually in one eye at a time, often with pain during eye movement • Prolonged double vision
- 13. CONTI… • Blurry vision • Slurred speech • Fatigue • Dizziness • Tingling or pain in parts of your body • Problems with sexual, bowel and bladder function
- 14. DIAGNOSTIC EVALUATIONS: • History of repeated exacerbations & remission. • MRI- lesions can be found. • CT Scan- atrophy & white matter lesions. • CSF analysis- increased no. of T lymphocytes that are reactive with antigens. • PET scan- it reveals areas with changes in glucose metabolism. • Evoked response testing of visual, auditory impulse may show delayed conduction. • Lumbar puncture
- 18. COMPLICATIONS • Muscle stiffness or spasms • Paralysis, typically in the legs • Problems with bladder, bowel or sexual function • Mental changes, such as forgetfulness or mood swings • Depression • Epilepsy
- 19. MANAGEMENT: • Corticosteroids, such as oral prednisone and intravenous methylprednisolone, are prescribed to reduce nerve inflammation. Side effects may include insomnia, increased blood pressure, mood swings and fluid retention. • Plasma exchange (plasmapheresis). The liquid portion of part of your blood (plasma) is removed and separated from your blood cells. The blood cells are then mixed with a protein solution (albumin) and put back into your body. Plasma exchange may be used if your symptoms are new, severe and haven't responded to steroids
- 20. THANK YOU