Blood glucose homeostasis revised
•Transferir como PPT, PDF•
111 gostaram•53,990 visualizações

Blood glucose homeostasis, Role of insulin, glucagon, hypoglycemia, hyperglycemia and glycosuria

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Blood glucose homeostasis revised
Semelhante a Blood glucose homeostasis revised (20)
Mais de Namrata Chhabra
Mais de Namrata Chhabra (20)
Último
Último (20)
Blood glucose homeostasis revised
- 1. BLOOD GLUCOSE HOMEOSTASIS Professor (Dr.) Namrata Chhabra Biochemistry for medics- Lecture notes 11/07/14 Biochemistry for medics- Lecture notes 1
- 2. Homeostasis Biochemistry for medics- Lecture notes 11/07/14 2 Homeostasis is the maintenance of a stable internal environment within an organism, and maintaining a stable internal environment in a human means having to carefully regulate many parameters including glucose levels in the blood.
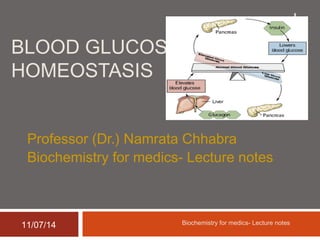
- 3. Glucose homeostasis Biochemistry for medics- Lecture notes 11/07/14 3 Glucose homeostasis reflects a balance between hepatic glucose production and peripheral glucose uptake and utilization. Insulin is the most important regulator of this metabolic equilibrium, but neural input, metabolic signals, and other hormones (e.g., glucagon) result in integrated control of glucose supply and utilization.
- 4. Homeostasis Of Blood Glucose Levels Biochemistry for medics- Lecture notes 11/07/14 4 Glucose is an obligate metabolic fuel for the brain under physiologic conditions. The brain cannot synthesize glucose or store it as glycogen Therefore requires a continuous supply of glucose from the arterial circulation.
- 5. Brain and glucose Biochemistry for medics- Lecture notes 11/07/14 5 As the arterial plasma glucose concentration falls below the physiologic range, blood-to-brain glucose transport becomes insufficient to support brain energy metabolism and function. However, redundant glucose counter regulatory mechanisms normally prevent or rapidly correct hypoglycemia.
- 6. Plasma glucose concentrations Biochemistry for medics- Lecture notes 11/07/14 6 Plasma glucose concentrations are normally maintained within a relatively narrow range, roughly 70–110 mg/dL (3.9–6.1 mmol/L) in the fasting state with transient higher excursions after a meal, despite wide variations in exogenous glucose delivery from meals and in endogenous glucose utilization by, for example, exercising muscle.
- 7. Plasma glucose concentrations Biochemistry for medics- Lecture notes 11/07/14 7 Between meals and during fasting, plasma glucose levels are maintained by- Endogenous glucose production, hepatic (and renal) gluconeogenesis, Hepatic glycogenolysis.
- 8. Hepatic glycogen stores Biochemistry for medics- Lecture notes 11/07/14 8 Although hepatic glycogen stores are usually sufficient to maintain plasma glucose levels for approximately 8 hour , this time period can be shorter if glucose demand is increased by exercise or if glycogen stores are depleted by illness or starvation.
- 9. Gluconeogenesis Biochemistry for medics- Lecture notes 11/07/14 9 Gluconeogenesis requires a coordinated supply of precursors from muscle and adipose tissue to the liver (and kidneys). Muscle provides-o Lactate, o Pyruvate, o Alanine, glutamine, and other amino acids.
- 10. Gluconeogenesis Biochemistry for medics- Lecture notes 11/07/14 10 Triglycerides in adipose tissue are broken down into fatty acids and glycerol, which is a gluconeogenic precursor. Fatty acids provide an alternative oxidative fuel to tissues other than the brain (which requires glucose). Fatty acids can not be used for glucose production.
- 11. Systemic glucose balance Biochemistry for medics- Lecture notes 11/07/14 11 Maintenance of the normal plasma glucose concentration—is accomplished by- A network of hormones, Neural signals, and Substrate effects that regulate endogenous glucose production and glucose utilization by tissues other than the brain
- 12. Role of Insulin Biochemistry for medics- Lecture notes 11/07/14 12 Glucose is the key regulator of insulin secretion by the pancreatic beta cells Glucose levels > 3.9 mmol/L (70 mg/dL) stimulate insulin synthesis Glucose stimulation of insulin secretion begins with its transport into the beta cell by the GLUT2 glucose transporter Insulin promotes peripheral glucose uptake and utilization, and inhibits gluconeogenesis as well as glycogenolysis.
- 13. Systemic glucose balance Biochemistry for medics- Lecture notes 11/07/14 13
- 14. Role of insulin in the fasting state Biochemistry for medics- Lecture notes 11/07/14 14 In the fasting state, low insulin levels increase glucose production by- Promoting hepatic gluconeogenesis and glycogenolysis and Reducing glucose uptake in insulin-sensitive tissues (skeletal muscle and fat), thereby promoting mobilization of stored precursors such as amino acids and free fatty acids (lipolysis). These effects are mediated by Glucagon.
- 15. Role of Glucagon in the fasting state Biochemistry for medics- Lecture notes 11/07/14 15 Glucagon, secreted by pancreatic alpha cells when blood glucose or insulin levels are low, stimulates – Glycogenolysis Gluconeogenesis by the liver and renal medulla and Prevents glucose uptake by the peripheral cells
- 16. Postprandial Glucose homeostasis Biochemistry for medics- Lecture notes 11/07/14 16 Postprandially, the glucose load elicits a rise in insulin and fall in glucagon, leading to a reversal of these processes. Insulin, an anabolic hormone, promotes the storage of carbohydrate and fat and protein synthesis. The major portion of postprandial glucose is utilized by skeletal muscle, an effect of insulin-stimulated glucose uptake. Other tissues, most notably the brain, utilize glucose in an insulin-independent fashion.
- 17. Phases of glucose homeostasis Biochemistry for medics- Lecture notes 11/07/14 17 Phase 1 Phase 2 Phase 3 Phase 4 Nutritional status Well fed state Post- Absorptive state Fasting Prolonged fasting/ Starvation Source of glucose Diet Hepatic glycogen and Gluconeogenesis Hepatic and Renal gluconeogenesi s Renal and hepatic gluconeogenesi s Tissues using glucose All All tissues, but in Liver, muscle and adipose tissue, the rate of utilization is slowed. Brain and RBCs and cells lacking mitochondria; small amount by muscle. Brain at a slower rate, RBCs normal rate Major fuel of brain Glucose Glucose Glucose and ketone bodies Ketone bodies and glucose
- 18. Glucose homeostasis in well fed state Biochemistry for medics- Lecture notes 11/07/14 18 In the well fed state, glucose absorbed from gut is supplied to all cells; it acts as a signal for the release of insulin from Beta cells of pancreas; it is oxidized completely to provide energy; the surplus is stored as glycogen in liver and muscle. Acetyl co A obtained from pyruvate, can be used for lipogenesis , the triglycerides are stored in adipose tissue.
- 19. Glucose homeostasis in post- Absorptive Phase Biochemistry for medics- Lecture notes 11/07/14 19 1) Glucose utilization is decreased in the liver, muscle and adipose tissue 2) Liver glycogenolysis provides the most glucose (75%) 3) gluconeogenesis providing the remainder 4) The glucose-alanine cycle becomes active. 5) 50-60% of glucose is consumed by the
- 20. Glucose homeostasis in the early fasting state Biochemistry for medics- Lecture notes 11/07/14 20 1) The peripheral cells switch to alternative fuels, such as fatty acids and ketone bodies. 2) Ketone bodies are synthesized by the liver but utilized in the peripheral cells. 3) Glycerol and amino acids released form the adipose tissue and muscle respectively are used for glucose production. 4) Glucose is the main fuel for brain.
- 21. Glucose homeostasis in the state of Starvation Biochemistry for medics- Lecture notes 11/07/14 21 1) Glucose alanine cycle is active. 2) Alanine and glutamine released from muscle are used in liver and kidney respectively for glucose production 3) Ketones play a central role in prolonged starvation, replacing glucose as the primary fuel for the brain and signaling a reduction in protein catabolism and alanine output from muscle.
- 22. Role of hormones in glucose homeostasis Biochemistry for medics- Lecture notes 11/07/14 22 Insulin Glucagon Catechol amines Glucocort icoids Growth hormone Thyroid hormone Glucose absorption No effect No effect No effect No effect No effect Peripheral uptake Glycolysis Gluconeogen esis Glycogenesis Glycogenolysi s Lipolysis Protein catabolism Net effect Hypogly cemia Hyperglyc emia Hypergly cemia Hyperglyc emia Hypergly cemia Hyperglycemia
- 23. Variations in blood glucose levels Biochemistry for medics- Lecture notes 11/07/14 23 A) Hypoglycemia- Decrease in blood glucose below the normal is called hypoglycemia. A decrease in insulin secretion is the first defense against hypoglycemia. As plasma glucose levels decline just below the physiologic range, glucose counter regulatory (plasma glucose–raising) hormones are released. Among these, pancreatic α cell glucagon, which stimulates hepatic glycogenolysis, plays a primary role. Glucagon is the second defense against hypoglycemia.
- 24. A) Hypoglycemia (contd.) Biochemistry for medics- Lecture notes 11/07/14 24 Adreno- medullary epinephrine, which stimulates hepatic glycogenolysis and gluconeogenesis (and renal gluconeogenesis), is not normally critical, however, it becomes critical when glucagon is deficient. Epinephrine is the third defense against hypoglycemia. When hypoglycemia is prolonged, cortisol and growth hormone also support glucose production and limit glucose utilization.
- 25. Hypoglycemia Biochemistry for medics- Lecture notes 11/07/14 25 Hypoglycemia is a laboratory ‘diagnosis’ which is usually considered a blood glucose level below 60 mg/dL. Symptoms begin at plasma glucose levels in the range of 60 mg/dL and Impairment of brain function at approximately 50 mg/dL.
- 26. Types of Hypoglycemia Biochemistry for medics- Lecture notes 11/07/14 26 Spontaneous hypoglycemia in adults is of two principal types: 1) Fasting hypoglycemia is often sub acute or chronic and usually presents with neuroglycopenia as its principal manifestation. 2) Postprandial hypoglycemia is relatively acute and is often heralded by symptoms of neurogenic autonomic discharge (sweating, palpitations, anxiety, and tremulousness).
- 27. Common causes of hypoglycemia Biochemistry for medics- Lecture notes 11/07/14 27 A) Physiological- Pronged fasting or starvation. B) Pathological 1) Fasting hypoglycemia o Drug induced- Insulin, oral hypoglycemic drugs, alcohol, sulfonamides etc. o Critical illnesses - Hepatic, renal, or cardiac failure, and sepsis. o Hormone deficiencies- Cortisol, growth hormone, or both, Glucagon and epinephrine (in insulin-deficient diabetes)
- 28. Common causes of hypoglycemia Biochemistry for medics- Lecture notes 11/07/14 28 o Endogenous hyperinsulinism o Insulinoma o Autoimmune (autoantibodies to insulin or the insulin receptor) o Ectopic insulin secretion o Congenital hyperinsulinism and o Inherited enzyme deficiencies
- 29. Common causes of hypoglycemia Biochemistry for medics- Lecture notes 11/07/14 29 2) Postprandial (reactive) hypoglycemia a) Alimentary (Postgastrectomy) b) Hereditary fructose intolerance, c) Galactosemia d) Idiopathic.
- 30. B) Hyperglycemia Biochemistry for medics- Lecture notes 11/07/14 30 Increase in blood glucose level above the normal physiological limit is called as Hyperglycemia Causes of hyperglycemia Diabetes mellitus Diseases of pancreas(pancreatitis, hemochromatosis, carcinoma head of pancreas, Cystic fibrosis) Infections and sepsis Anesthesia Asphyxia
- 31. B) Hyperglycemia Biochemistry for medics- Lecture notes 11/07/14 31 Causes of hyperglycemia (contd.) Hormonal tumors-o Acromegaly, o Cushing's syndrome, o Glucagonoma and o Pheochromocytoma
- 32. B) Hyperglycemia Biochemistry for medics- Lecture notes 11/07/14 32 Causes of hyperglycemia (contd.) o Pharmacologic agents (corticosteroids, sympatho mimetic drugs, thiazide diuretics and niacin) o Liver disease (cirrhosis, hemochromatosis) o Muscle disorders (myotonic dystrophy) o Adipose tissue disorders (Lipodystrophy and truncal obesity)
- 33. Clinical implication of disturbed glucose homeostasis-Glycosuria Biochemistry for medics- Lecture notes 11/07/14 33 Although normal urine contains virtually no sugar but under certain circumstances, glucose or other sugars may be excreted in urine. This condition is called ‘Melituria’. The term Glucosuria, Fructosuria, Galactosuria, Lactosuria and Pentosuria are applied specifically for urinary excretion of glucose, fructose, galactose, lactose and pentose respectively.
- 34. Types of Glycosuria 34 Glycosuria(Glucosuria) can be classified in to two main groups A) Hyperglycemic glycosuria B) Renal glycosuria Biochemistry for medics- Lecture notes 11/07/14
- 35. A) Hyperglycemic glycosuria Biochemistry for medics- Lecture notes 11/07/14 35 Alimentary Glycosuria(Excessive ingestion of carbohydrates) Emotional Glycosuria(Excessive catecholamine release)- Stress, anxiety etc.
- 36. Hyperglycemic glycosuria Biochemistry for medics- Lecture notes 11/07/14 36 Glycosuria due to endocrinal disorders e.g. o Diabetes Mellitus o Hyperthyroidism o Epinephrine hyper secretion o Hyperactivity of anterior pituitary(Acromegaly) o Hyperactivity of Adrenal cortex(Cushing’s syndrome/disease) o Increased secretion of glucagon
- 37. B) Renal Glycosuria Biochemistry for medics- Lecture notes 11/07/14 37 Renal Tubular disease Fanconi's Syndrome Toxic renal tubular disease o Lead Toxicity o Mercury Toxicity
- 38. Renal glycosuria Biochemistry for medics- Lecture notes 11/07/14 38
- 39. Diabetes mellitus Biochemistry for medics- Lecture notes 11/07/14 39 Diabetes mellitus is a syndrome with disordered metabolism and inappropriate hyperglycemia due to either a deficiency of insulin secretion or to a combination of insulin resistance and inadequate insulin secretion to compensate. Type 1 diabetes is due to pancreatic islet B cell destruction predominantly by an autoimmune process, and these patients are prone to ketoacidosis. Type 2 diabetes is the more prevalent form and results from insulin resistance with a defect in compensatory insulin secretion
- 40. Blood glucose homeostasis (Summary) Biochemistry for medics- Lecture notes 11/07/14 40 Glucose homeostasis reflects a balance between hepatic glucose production and peripheral glucose uptake and utilization. Insulin is the most important regulator of this metabolic equilibrium. In the fasting state, low insulin levels increase glucose production by promoting hepatic Gluconeogenesis and glycogenolysis and reduce glucose uptake in insulin-sensitive tissues Glucagon, secreted by pancreatic alpha cells when blood glucose or insulin levels are low, stimulates glycogenolysis and gluconeogenesis by the liver and renal medulla.
- 41. Blood glucose homeostasis (Summary) Biochemistry for medics- Lecture notes 11/07/14 41 Postprandially, the glucose load elicits a rise in insulin and fall in glucagon, leading to a reversal of these processes. Insulin, an anabolic hormone, promotes the storage of carbohydrate and fat and protein synthesis. The major portion of postprandial glucose is utilized by skeletal muscle, an effect of insulin-stimulated glucose uptake. Other tissues, most notably the brain, utilize glucose in an insulin-independent fashion.