
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a 9 nosocomial pneumonia combating MDROs
Semelhante a 9 nosocomial pneumonia combating MDROs (20)
Mais de Yaser Ammar
Mais de Yaser Ammar (16)
Último
Último (20)
9 nosocomial pneumonia combating MDROs
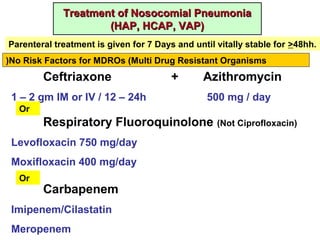
- 1. Treatment of Nosocomial PneumoniaTreatment of Nosocomial Pneumonia (HAP, HCAP, VAP)(HAP, HCAP, VAP) No Risk Factors for MDROs (Multi Drug Resistant Organisms) Ceftriaxone + Azithromycin 1 – 2 gm IM or IV / 12 – 24h 500 mg / day Or Respiratory Fluoroquinolone (Not Ciprofloxacin) Levofloxacin 750 mg/day Moxifloxacin 400 mg/day Or Carbapenem Imipenem/Cilastatin Meropenem Parenteral treatment is given for 7 Days and until vitally stable for >48hh.
- 2. Risk Factors for MDROs • Initial empiric antibiotic treatment should include: o Antipseudomonal agent: - Antipseudomonal penicillin (Pipracillin/Tazobactan). - Antipseudomonal cephalosporin (Ceftazidime or Cefepime). - Carbapenem (Imipenem/Cilastatin or Meropenem). In severe infection, 2 classes of anti-pseudomonal agents are used. o Anti- MRSA agent (Vancomycin or Linezolid). In severe infection, Vancomycin is started by a loading dose of 25 – 30 mg/Kg, then maintained at 15 – 20 mg/kg/ 8 – 12h. • Aminoglycosides or colistin may be used as alternative choices in patients with Gram –ve MDROs. They should be used for the shortest possible course, with close monitoring of renal functions. Dose adjustment may be required according to renal function.
- 3. Multi Drug Resistant Organisms (MDROs)Multi Drug Resistant Organisms (MDROs) • They are microorganisms, predominantly bacteria, that are resistant to one or more classes of antibacterial agents. • Lack of a standardized definition limits comparison of resistance data from different populations. Hazards MDROs constitute one of the most serious and growing threats to public healyh: • ↑ hospital stay, cost and complications. • Compulsory use of more toxic antibiotics → adverse effects, eg, nephrotoxicity of aminoglycosides, colistin. • ↑ Mortality • Perpetuation of the problem of MDROs through: o Colonization/infection of other patients or health care workers. o Contamination of equipment, environmental surfaces. o Transmission of resistant traits to other bacteria.
- 4. Increasing Prevalence of MRSA MRSA was 1st isolated in USA in 1968
- 5. • Introduction of a resistant organism to a potentially susceptible population. • Dissemination of resistant organisms. Potentially preventable by Infection Control Program, particularly isolation precautions. • Selection of a resistant subpopulation. • Expression of dormant resistance. • Acquisition of resistance by a previously susceptible strain. Potentially preventable by Antibiotic Stewardship Program. The selection of resistance in one organism in one part of the world, even within an animal population, may have long- term important implications for human health globally. Mechanisms of Appearance and Spread of MDROs
- 6. Evidence that Organism Resistance is Closely Related to Antibiotic Use • Antimicrobial resistance is more common in nosocomial bacterial strains than in community- acquired infections. • Patients infected with resistant strains are more likely to have received prior antibiotics. • Hospital areas with highest rates of antimicrobial resistance have the highest rates of antimicrobial use. • Increasing duration of patient exposure to antimicrobials ↑ the likelihood of colonization with resistant organisms. Examples of Improper Antibiotic Use Favoring Development of MDROs • Antibiotics for viral infection. (eg, upper respiratory infection) • Antibiotics for specimen contamination. (eg, by skin flora) • Antibiotics for asymptomatic colonization. ((eg, UTI) • Improper antibiotic selection: overuse of broad spectrum agents / or using non- clinically effective agents (even if effective in vitro). • Improper antibiotic dose or duration.
- 7. Risk Factors for Acquisition of MDROs • Recent IV antimicrobial therapy (last 3 months). • Hospitalization for > 5 days. • Attendance of an extended care facility. • Maintenance haemodialysis. • Home infusion therapy (including antibiotics). • Home wound care. • Family member with MDROs. • Environmental colonization with MDROs (common in ICU). • Immunocompromized state (cancer chemotherapy, immunosuppressive treatment, HIV infection). • Risk factors for MDROs-VAP: o Septic shock before VAP. o ARDS before VAP. o Acute renal replacement therapy before VAP.
- 8. Combating Multi Drug Resistant OrganismsCombating Multi Drug Resistant Organisms • It is recommended that all hospitals, large and small, with or without perceived problems of bacterial resistance to antimicrobials, implement a set of measures to reduce the burden and transmission of MDROs. • All efforts in this respect generally fall under 2 basic strategic programs: infection control and antibiotic stewardship. • Such programs should be considered a shared responsibility of the whole medical institution personnel from top administration down to service workers. • A dedicated program leader (physician – pharmacist) should be assigned and authorized to manage a team work to achieve well defined goals. • Hospital committees particularly involved in these programs are Infection Control Committee (ICC), Pharmacy and Therapeutics Committee (PTC) and Morbidity Mortality Committee (MMC). An Antibiotic Utilization Subcommittee may also be launched to set local antibiotic guidelines and supervise antibiotic use.
- 9. Infection Control ProgramInfection Control Program • Most of the health care delivery related factors are due to poor adherence to recommended evidence based infection prevention/control practices. • Despite recognition that poor hand hygiene practice is a leading cause of pathogen transmission, the existence of major national and international guidelines, and initiatives to improve hand hygiene practices among health care workers, compliance with recommended hand hygiene practices among health care personnel remains unacceptably low. • The CDC Guidelines for Isolation Precautions in Hospitals should be strictly applied, particularly concerning isolation of patients colonized or infected with resistant organisms. • It is recommended that hospitals choose organisms which are of special clinical and epidemiologic importance to identify patients in need for isolation. • The validity of treatment of colonized patients is controversial, but their isolation may be required exactly as infected patients.
- 10. Antibiotic Stewardship Program (ASP)Antibiotic Stewardship Program (ASP) • It is a hospital- based program intended to track and improve antibiotic use in order to improve their efficiency, reduce their costs and adverse effects and, particularly, reduce their potential to cause selection and spread of MDROs. • ASP includes not only limitation of the use of inappropriate agents, but also the appropriate selection and dosing of antimicrobial agents in order to achieve the optimal efficiency in managing infections. • It aims to have all patients treated with the most efficient, least toxic and least costly antibiotic for the optimal duration of time.
- 11. Role of Microbiologist Restricted Reporting of Some Selected Broad Spectrum Antibiotics • Sensitivity to some selected broad spectrum antibiotics might not be released in the report, unless: o resistance to narrower spectrum antibiotics documented (eg, sensitivity to carbapenems released in case of resistance to β-lactams). o requested by an authorized physician. • Advantage: more prudent, less costly antibiotic selection. • Disadvantage: possibly ineffective treatment, resistance. Selective Reporting of C/S (Culture and Sensitivity) results Disc diffusion method for Antibiotic Sensitivity
- 12. Restricted Reporting of Clinically Ineffective Antibiotics even in Presence of Documented in-vitro Organism Susceptibility Demonstration of in-vitro susceptibility of an isolate to a particular antibiotic in the lab does not necessarily indicate clinical effectiveness when this antibiotic is given to treat a clinical infectious disease. Clinical resistance may result from: • Low systemic bioavailability. • Low penetration into the infection site → failure to achieve target MIC, particularly if it is relatively high (intermediate resistance). • Presence or retained pus or foreign body. • Rapid development of resistant strains. Examples of “in-vitro only” susceptibility that should not be reported: - ESBL (extended spectrum β-lactamase producing) organisms should not be reported sensitive to β-lactams. - Oxacillin resistant Staph. aureus (MRSA) should not be reported sensitive to β-lactam/β-lactamase inhibitors and carbepenems.
- 13. Inclusion of Useful Hints in the C/S Report • Blood sample probably contaminated with skin flora. • Sputum sample probably contaminated with mouth flora. • Starting with an antibiotic combination recommended to prevent rapid development of resistance. Examples: Recognition and Reporting of Antimicrobial Resistance Patterns • Unusual antibiograms, especially multiply resistant patterns, can be helpful for early identification of outbreak- related isolates. • An even earlier indicator is a trend towards increasing resistance in quantitative susceptibility tests (which are generally preferred to simple break point systems): o ↓ mean zone diameter around antibiotic discs. o ↑ MIC. • WHONET is a free web application supported by WHO that checks quantitative susceptibility test results and alerts for unusual drug resistance.
- 14. Role of Pharmacist There are 4 possible general strategies to improve antibiotic utilization in order to reduce the burden of MDROs: • Use the proper. • Do not use / modify the improper. • Rotate. • Combine. Use the Proper Antibiotic Antibiotic Selection Should Consider • National guidelines. • Local guidelines based on local microbial epidemiology, antimicrobial susceptibility patterns and drugs available in hospital formulary. Such guidelines should cove in particular the most commonly encountered conditions as CAP, UTI, blood stream infection and surgical prophylaxis. • Expert advice from highly qualified consultants and infectious disease specialists. • Discussion of complex issues in dedicated committees as ICC, PTC, MMC.
- 15. Pharmacist Role to Support Proper Antibiotic Selection • Selection of antibiotics to be included or excluded from hospital formulary. On light of clinical and microbiologic data, the most effective and potentially least toxic antibiotics are to be included. • Dispensing certain broad spectrum antibiotics is restricted unless ordered by an authorized consultant or infectious disease specialist. Do Not Use / Modify the Improper Antibiotic Pharmacy Tracking Pharmacy Driven InterventionsPharmacy Tracking • Review of Medical Records: to ensure full documentation of antibiotic prescription, including indication, dose and duration so that antibiotic courses can be easily identified and tracked. • Analysis of Antibiotic Utilization Trends: for both in- patients and out- patients. • Reporting issues of antibiotic use and misuse to the administration and relevant staff.
- 16. Pharmacy Driven Interventions in collaboration with the treating physician, microbiologist and infectious disease specialist: • De- escalation of antibiotic therapy based on culture results and clinical response. • Conversion of open- ended antibiotic orders to automatic stop orders, eg, in surgical prophylaxis. • Shift from parenteral to oral therapy, eg, quinolones. • Stop unnecessary antibiotics in patients diagnosed with Clostridium difficile infection. • Dose modification based on changes in renal / liver function and other variables.
- 17. • Dose optimization, eg, extended infusion of β-lactams to improve time- dependent killing.
- 18. Rotate Antibiotics Combine Antibiotics The validity of rotational or cyclic antibiotic use is controversial, eg, rotating gentamycin with amikacin Combination therapy may be recommended to prevent emergence of resistance strains, particularly in conditions requiring prolonged antibiotic courses. This is the basis for current treatment recommendations for TB. This approach may, however, ↑ costs and the potential for MDROs.
- 19. Other Components of ASP Administration should be serious in provision of the required human, financial and IT resources as well as authoritative privileges required. IT (Information Technology) Presence of a computerized MIS (Medical Information System) allows: • Faster and more efficient communication between physicians, pharmacists and microbiologists. • Easier documentation and tracking of antibiotic prescriptions. Health education Campaigns including fliers, multimedia and awareness weeks: • Targeting Physicians and Health Care Workers. • Targeting Patients and Families: o Use only antibiotics prescribed by health care professionals. o Use antibiotics exactly as prescribed. o Complete the treatment course, even if you feel better.
Notas do Editor
- Asymptomatic carriage of MDROs is relatively common among persons with health care related exposures. Patients with clinically apparent MDROs infection represent a relatively small proportion of the total burden. Some organisms survive long on inanimate objects. Some resist disinfectants as Pseudomonas aeroginosa. Some survive in an adherent biofilm, eg, on catheters.
- AHRQ: Agency for Health Care Research and Quality
- Antibiotics should not be used unnecessarily. We should generally aim to shield the eyes of our enemies from seeing our weapons. Strong weapons should be stored to surprise strong enemies when required. Our enemies (organisms) should not be given the opportunity to be prepared for our weapons (antimicrobials).
- CDC: Centers for Disease Prevention and Control, USA