New and Emerging Biomarkers in Patient-Centered MS Management: The Future of Personalized Patient Care Begins Now
•
0 gostou•4 visualizações

Chair and Moderator, Jiwon Oh, MD, PhD, FRCPC, Jacci Bainbridge, PharmD, FCCP, MSCS, FAES, and Kathleen M. Costello, RN, MS, NP, MSCN, prepared useful Practice Aids pertaining to multiple sclerosis for this CME/NCPD/CPE/IPCE activity titled “New and Emerging Biomarkers in Patient-Centered MS Management: The Future of Personalized Patient Care Begins Now.” For the full presentation, downloadable Practice Aids, and complete CME/NCPD/CPE/IPCE information, and to apply for credit, please visit us at https://bit.ly/3L4Wdjl. CME/NCPD/CPE/IPCE credit will be available until July 2, 2024.

Recomendados
Mais conteúdo relacionado
Semelhante a New and Emerging Biomarkers in Patient-Centered MS Management: The Future of Personalized Patient Care Begins Now
Semelhante a New and Emerging Biomarkers in Patient-Centered MS Management: The Future of Personalized Patient Care Begins Now (20)
Mais de PVI, PeerView Institute for Medical Education
Mais de PVI, PeerView Institute for Medical Education (20)
Último
Último (20)
New and Emerging Biomarkers in Patient-Centered MS Management: The Future of Personalized Patient Care Begins Now
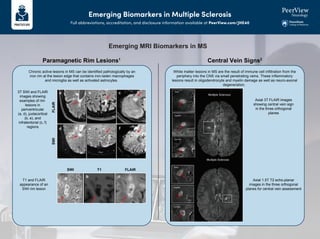
- 1. Emerging Biomarkers in Multiple Sclerosis Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 Emerging MRI Biomarkers in MS White matter lesions in MS are the result of immune cell infiltration from the periphery into the CNS via small penetrating veins. These inflammatory lesions result in oligodendrocyte and myelin damage as well as neuro-axonal degeneration. Chronic active lesions in MS can be identified pathologically by an iron rim at the lesion edge that contains iron-laden macrophages and microglia as well as activated astrocytes. Paramagnetic Rim Lesions1 Central Vein Signs2 3T SWI and FLAIR images showing examples of rim lesions in periventricular (a, d), juxtacortical (b, e), and infratentorial (c, f) regions T1 and FLAIR appearance of an SWI rim lesion Axial 3T FLAIR images showing central vein sign in the three orthogonal planes Axial 1.5T T2 echo-planar images in the three orthogonal planes for central vein assessment SWI T1 FLAIR SWI FLAIR
- 2. Emerging Biomarkers in Multiple Sclerosis Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 Main MRI Sequences Used for Detecting Each Biomarker3 Disease Activity/Prognosis Diagnosis/Classification Compartment SWI SWI QSM Phase 2 GRE/EPI SWI SWI T2 GRE/EPI FLAIR QSM Phase 2 GRE/EPI T2 GRE/EPI Paramagnetic rim Central vein sign With or without a contrast agent 7T 3T MRI (Field Strength and Image Modalities)
- 3. Emerging Biomarkers in Multiple Sclerosis Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 Emerging Fluid Biomarkers for MS Disease Activity and Prognosis4 Disease Activity/Prognosis Diagnosis/Classification Compartment Biomarker • Serum: ↑ CIS or RIS that converts to MS • ↓ with DMT in RMS or PMS • ↑ disease activity in RMS • ↑ risk of new MRI lesions • ↑ risk of brain/spinal cord atrophy • CSF and serum: ↑ in RMS and PMS vs HC • ↑↓ in PMS vs RMS (conflicting results) CSF, serum, plasma; good correlation NfL • Serum: ↑ risk of worsening EDSS • ↑ lesion progression on MRI • Serum: ↑ in active RMS vs NIND and HC • ↑↓ in PMS vs RMS (conflicting results) • ↑ in NMOSD vs MS or HC CSF, serum, plasma; good correlation GFAP • CSF: ↑ CIS that converts to MS • ↑ likelihood of disability progression • ↓ with DMT • ↑ risk of new MRI lesions • CSF: ↑ in RMS vs HC • ↑ in PMS vs RMS and SPMS CSF; CSF levels do not correlate with serum CHI3L1/YKL-40 • ↑ increased cortical lesion number • ↑ cortical thinning • ↑ cognitive impairment • CSF: ↑ PMS vs HC CSF Parvalbumin • ↑ lower risk of developing MS • ↓ neonatal vitamin D increased risk of developing MS • ↑ lower degree of brain atrophy • ↑ less clinical progression at year 5 • ↓ increased relapse risk Serum — Vitamin D • CSF: ↑ CIS that converts to MS • ↑ disease activity in RMS • CSF > serum: ↓ with DMT • Serum: Predict response to fingolimod • CSF: ↑ RMS and PMS vs NIND and OIND CSF; serum does not correlate with CSF CXCL13
- 4. Emerging Biomarkers in Multiple Sclerosis Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 1. Kwong K et al. Neuroradiology. 2022;64:109-117. 2. Maggi P et al. AnnNeurol. 2018;83:283-294. 3. La Rosa F et al. NeuroimageClin. 2022;36:103205. 4. Gill AJ et al.EurJImmunol. 2023;e2250228. Emerging Fluid Biomarkers for MS Disease Activity and Prognosis4 Central nervous system Cerebrospinal fluid Peripheral tissues Blood Blood brain barrier Peripheral neuron NfL Muscle Parvalbumin GFAP ? ? Nonmyelinating Schwann cell CHI3L1 Chondrocyte Neutrophil Macrophage Monocyte Activated microglia Activated macrophage CNS-restricted clonal B cells CHI3L1 Reactive astrocyte GFAP Clonal antibodies Detected as oligoclonal bands Damaged cortical interneuron Degenerating myelin and axon NfL Parvalbumin Blood-CSF barrier
- 5. 2021 MAGNIMS-CMSC-NAIMS Consensus Recommendations on the Use of MRI in Patients With Multiple Sclerosis1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 a Isotropic preferred, if over-contiguous (through-plane and in-plane), not >1.5 mm with 0.75-mm overlap. b Diffusion-weighted imaging, slice thickness should be <5 mm with a 10%-30% slice gap. Basic MRI Parameters Optic Nerve Spinal Cord Brain MRI Protocols ≥1.5T ≥1.5T (3T no added value) ≥1.5T (preferably 3T) Field strength 2D or 3D 2D or 3D 3D (preferred) or 2D Acquisition ≤2-3 mm, no gap Sagittal ≤3 mm, no gap Axial ≤5 mm, no gap 3D: 1 mm isotropica 2D: ≤3 mm, no gapb Slice thickness ≤1 mm x 1 mm ≤1 mm x 1 mm ≤1 mm x 1 mm In-plane resolution Optic nerve and chiasm Whole cord (cervical, thoracolumbar including conus) Whole brain (include as much of cervical cord as possible) Coverage Align to optic nerve/chiasm orientation Perpendicular to sagittal axis of cord Subcallosal plane Axial slice orientation
- 6. 2021 MAGNIMS-CMSC-NAIMS Consensus Recommendations on the Use of MRI in Patients With Multiple Sclerosis1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 Brain MRI Protocol Safety Monitoring Follow-Up Diagnostic Workup Brain Sequences Recommended (optional if 3D FLAIR acquired) Recommended (optional if 3D FLAIR acquired) Recommended Axial T2-weighted (TSE or FSE) sequences Recommended Recommended Recommended Sagittal T2-weighted FLAIR (preferably 3D; fat suppression is optional) Recommended Recommended Recommended Axial T2-weighted FLAIR (unnecessary if a sagittal 3D FLAIR with multiplanar reconstruction is obtained; fat suppression is optional) Optional Optional Recommended Axial (or 3D sagittal) T1-weighted sequences after contrast Recommended (for PML detection) Optional (useful for diff Dx) Optional Diffusion-weighted imaging Optional Optional Optional (for cortical lesions) Double inversion recovery or PSIR for detecting cortical or juxtacortical lesions Not Required Optional Optional (for brain atrophy monitoring) High-resolution T1-weighted sequences (isotropic 3D acquisition; for quantitative assessment of brain volume) Not Required Not Required Optional (for central vein sign) Susceptibility-weighted imaging
- 7. 2021 MAGNIMS-CMSC-NAIMS Consensus Recommendations on the Use of MRI in Patients With Multiple Sclerosis1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 Safety Monitoring Follow-Up Diagnostic Workup Spinal Cord Sequences Not required Optional 2 sequences recommended Sagittal at least 2 of T2, PD, or STIR Not required Optional Optional (substitutes for one of above) Sagittal 3D T1 (PSIR, MP-RAGE) cervical only Not required Optional Optional (through lesions) Axial T2 or T2 Not required Optional Optional Pre-Gd sagittal T1 Not required Optional Recommended Post-Gd sagittal T1 Not required Optional Optional Post-Gd axial T1 Optic Nerve Sequences Not required Not required Optional Axial and coronal fat- suppressed T2 or STIR Not required Not required Optional Post-Gd axial and coronal fat-suppressed T1 Spinal Cord and Optic Nerve MRI Protocol
- 8. 2021 MAGNIMS-CMSC-NAIMS Consensus Recommendations on the Use of MRI in Patients With Multiple Sclerosis1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 a Shorter follow-up MRI (ie, 6 months) if substantial isolated MRI activity or isolated clinical activity. b Add spinal cord MRI to brain MRI if disability worsening is not explained by brain MRI. c Add spinal cord MRI to brain MRI if never done. d Longer intervals to be considered in patients treated with disease-modifying treatments (eg, up to 9 months with glatiramer acetate and until completion of the full initial course with induction therapies). e Less frequent MRI in clinically stable patients treated with interferon beta or glatiramer acetate. f Consider gadolinium administration in patients with highly active disease at baseline or in patients with unexpected clinical activity after treatment initiation. Initial Pretreatmentc Follow-Upsa,b Every year while on treatmente Gadolinium optional Second Follow-Upa,b 24 mo after treatment onset Gadolinium optional First Follow-Upa,b 12 mo after treatment onset Gadolinium optional New Baseline 3-6 mo after treatment onsetd Gadolinium usually not requiredf Gadolinium recommended MRI in Pediatrics and Pregnancy • Brain and full spinal cord with gadolinium • Optic nerve when MOG/NMOSD under consideration Pediatrics diagnostic MRI • Same as adults for follow-up and safety monitoring • Every 6 months for highly active disease Pediatric monitoring • Assessed case by case (unexpected clinical course) • Gadolinium contraindicated Pregnancy • New baseline 2-3 mo post partum • Gadolinium should only be used judiciously Post partum and lactation MRI Timing in Monitoring of Multiple Sclerosis
- 9. 2021 MAGNIMS-CMSC-NAIMS Consensus Recommendations on the Use of MRI in Patients With Multiple Sclerosis1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 1. Wattjes M et al.LancetNeurol. 2021;20:653-670. Summary of Key Recommendations • 3D-FLAIR brain MRI most important for diagnosis and monitoring • Gadolinium use is restricted to diagnosis and early monitoring • Spinal cord MRI is important for diagnosis and prognosis; dual contrast • Re-baseline brain MRI after switching treatment (no gadolinium) • Annual brain MRI while on treatment • PML monitoring every 3-4 months with abbreviated protocol • Central vein sign, cortical lesions, and brain volume change quantification is not recommended
- 10. Shared Treatment Decision-Making in Multiple Sclerosis1-6 Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 Yes Consider different MOA and/or route of administration Change therapy? • Suboptimal response? • Intolerable adverse events? • Inadequate treatment adherence? • Disease-related factors (phenotype, activity, severity) • Patient-related factors (preference, comorbidities) • Drug-related factors (efficacy, safety, route of administration) • Relapsing or progressive • Active or not active • With or without progression or worsening Identify the multiple sclerosis phenotype • Clinical • MRI • Safety • Biomarkers Monitor No Oral Self- injection Infusion Choose therapy in collaboration with the patient
- 11. Shared Treatment Decision-Making in Multiple Sclerosis1-6 Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 Please provide your answers to the following questions. 2. How do you prefer to take your medicine? 4. What are your thoughts about laboratory monitoring? 3. How much risk are you truly willing to accept? I prefer to self-inject I prefer to take a pill I prefer to have an IV infusion I have no preference of how I take my medication as long as it can be taken as infrequently as possible Risk averse: I am a safety first, benefits second type of person Moderately risk averse: I am willing to accept a little bit of risk for some extra benefit Mildly risk averse: I can accept risks for more benefit, as long as they are not serious High risk, high reward: I can accept any potential risks if they are outweighed by the potential benefits No evidence of disease activity (no attacks, no new findings on my MRI, no new disability) Preserve or improve my current level of functioning Sustain employment and normal daily activities All of the above I don’t want to be required to have any laboratory testing during treatment I am okay with laboratory testing as long I don’t have to do it every month or after I stop treatment I have no issues with the frequency or duration of laboratory testing that may be required during or after treatment 1. What are your goals for treatment?
- 12. Shared Treatment Decision-Making in Multiple Sclerosis1-6 Full abbreviations, accreditation, and disclosure information available at PeerView.com/JHE40 1. Giovannoni G et al. Curr Opin Neurol. 2012;25(Suppl):S20-S27. 2. Rae-Grant A et al. Neurology. 2018;90:777-788. 3. Lublin FD et al. Neurology. 2014;83:278-286. 4. Gaetani L et al. J Neurol Neurosurg Psychiatry. 2019;90:870-881. 5. Hanson KA et al. Patient Prefer Adherence. 2014;8:415-422. 6. Wilson LS et al. Int J MS Care. 2015;17:74-82. The Key Components of Engaging Patients in the Decision-Making Process 2. Describe options 3. Help make decisions Determine what patient already knows List and describe options including risks and benefits Provide decision support such as decision aids, which can help patients understand their options List options again and apply teach-back method by asking patient how they would describe the options to a loved one Focus on preferences Check to see if patient is ready to make a decision or if they need more time or have additional questions Agree on treatment plan Ensure patient understands plan can be modified and decisions can be reviewed at any time Identify/summarize problem Offer choices Emphasize importance of personal preferences Discuss any uncertainties in treatment Check reaction Defer final decision until you are able to discuss options in more detail if patient asks, “What would you do?” 1. Introduce choice