Closed Sinus Lift Surgery
•
2 gostaram•359 visualizações

Closed sinus lift surgery Techniques and Criteria References: Linde - Clinical Periodontology and Implant Dentistry Newman and Carranza Clinical Periodontology 13th Edition 2019

Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Closed Sinus Lift Surgery
Semelhante a Closed Sinus Lift Surgery (20)
Último
Último (20)
Closed Sinus Lift Surgery
- 2. Boyne (1960) Boyne & James (1980) : Bladed Implant • two‐stage : 1. Autogenous particulate iliac bone 2. Blade implants were placed (after 3month) Tatum (1986) • TransAlveolar Tech (A) : Socket Former -- Green Stick F -- Root for Implant Summer (1994) • TransAlveolar Tech (B) : Using tapered Osteotomes : conservative Tech Drilling was not performed
- 3. Two‐stage technique using the lateral window approach One‐stage technique using a lateral or a transalveolar approach How to decision? Amount of residual bone available Possibility of achieving primary stability
- 4. the most important of which is the availability of bone removable prostheses, short implants, cantilevered restorations (Carranza)
- 5. Placement of short implants : • most canservative : at least 6 mm of residual bone Tilted Implant Extra‐long zygomatic implants Minor augmentation – TransAlveolar Tech Lateral approach (one or two satge): • Most Invasive Shortened Dental Arch
- 6. distal aspect of the implant is more apical than at the time of implant placement
- 7. Patients maintained adequate (51–80%) chewing capacity with a premolar occlusion
- 8. Implant success rates are equal to or better than that of implants placed in nongrafted maxillary bone Interocclusal dimension is normal or only moderately increased
- 10. Advantage : more conservative and less invasive approach Disadvantage : possibility of perforation Elevated by up to 5 mm without perforating the membrane
- 11. Flat sinus floor Residual bone height of at least 5 mm Adequate crestal bone width
- 12. less than 7 mm of existing vertical bone height
- 13. Intraoral contraindications Medical conditions Local contraindications
- 14. Chemotherapy or radiotherapy of the head and neck area Immunocompromised patients Medical conditions affecting Bone metabolism Uncontrolled diabetes Drug or alcohol abuse Patient non‐compliance Psychiatric conditions
- 16. Viral, bacterial, and mycotic rhinosinusitis Allergic sinusitis Sinusitis caused by intrasinus foreign bodies Odontogenic sinusitis resulting from necrotic pulp tissue All odontogenic, periapical, and radicular cysts of the maxillary sinus
- 17. Acute sinusitis Allergic rhinitis Chronic recurrent sinusitis Scarred and hypofunctional mucosae Local aggressive benign tumors Malignant tumors
- 18. patients with a history of inner ear complications positional vertigo oblique sinus floor (>45° inclination) : • high risk perforating
- 19. sloped sinus floor presence of septa
- 21. The goal of sinus elevation and bone augmentation is to lift the schneiderian membrane from the floor of the sinus originally used as a preprosthetic surgical procedure
- 22. 5 mm of existing native bone 1 mm of remaining bone Ability to achieve implant stability
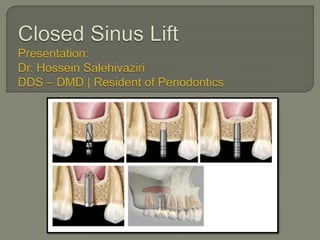
- 23. 1. Presurgical patient preparation 2. Local anesthesia (buccal and palatal) 3. Mid‐crestal incision with or without releasing 4. Implant positions are marked 5. Crestal floor to the floor of the maxillary sinus, measured
- 24. Exact position of the implant site is first marked with a small round bur
- 25. 6. Pilot drills 7. The first Tapered Osteotome: • Greenstick fracture an osteotome is chosen to minimize the force needed to fracture the compact bone.
- 26. 8. The seccond Tapered Osteotome: • Increase the fracture area diameter slightly larger then the first one
- 27. 9. The third Osteotome used is straight diameter about 1–1.5 mm smaller than that of the implant to be placed
- 29. Advantage: • Reduce the risk of membrane perforation • Reduce the risk of benign paroxysmal positional vertigo Disadvantage : • More time consuming
- 30. 1. the straight osteotome penetrates the sinus floor 2. Form and diameter that are suitable for the implant 3. Final step before placing the implant is to check that the preparation is patent to the planned insertion depth
- 31. 1. osteotomes are not supposed to enter the sinus cavity 2. sinus membrane must by tested for any perforations
- 32. 3. preparation is filled with grafting material
- 33. Preparation is checked for patency by repeating the Valsalva maneuver.
- 34. Antiseptic rinsing 0.1–0.2% CHX: • Twice daily - 3 weeks Antibiotic prophylaxis: • for 1 week in cases where bone substitutes are used
- 35. There is still controversy with regards to the necessity of using grafting material to maintain the space for new bone formation after elevating the sinus • Rosen 1999 • Nedir 2010 • Schmidlin 2008 • Petursson 2009 • Bragger 2004
- 36. Radiograph taken at the 5‐year follow‐up visit of an implant placed in the first quadrant utilizing the osteotome technique without grafting material. A new cortical bony plate at the inferior border of the maxillary sinus is clearly visible, but no bony structure can be detected apical to the implant
- 37. Radiograph (same patient) taken after 5 years in function of an implant placed in the second quadrant utilizing the osteotome technique with xenograft grafting material. A dome‐shaped structure is clearly visible, documenting a definite increase in bone volume compared to the initial situation. The “dome” is surrounded by a new cortical bony plate.
- 38. (a) Radiograph taken immediately after implant insertion with the osteotome technique and grafting material, showing a cloudy dome‐shaped structure extending 2–3 mm apical to the implant. (b) Radiograph of the same implant taken 1 year later showing significant reduction of the size of the “dome”, but the new bony structure is clearly visible apical to the implant
- 39. Autogenous bone is often referred to as the gold standard Anorganic bovine bone-derived mineral (ABBM) demineralized freeze-dried bone allograft (shrinkage)
- 42. Increased bone height from 2 to 7 mm (average, 3.8 mm) If more vertical bone height is needed, the lateral wall osteotomy approach may be more advantageous.
- 43. the implant survival rate was 96% when residual bone height was 5 mm or more, but dropped to 85.7% when residual bone height was 4 mm or less
- 44. Transalveolar sinus floor elevation technique was most predictable when the residual alveolar bone height was ≥5 mm and with implants of ≥8 mm.
- 45. Indications: Filling material for the sinus: (either alone or in combination with a bone substitute) Membrane to seal the lateral window for protection of the schneiderian membrane after detachment from the underlying bone Close a membrane rupture.
- 46. L-PRF can be used successfully as the sole filling material during sinus augmentation, but only if it is used simultaneously with the placement of implants
- 47. when L-PRF as the sole filler material, natural bone regeneration occurred around the implants • 10 mm vertical bone gain with the Window technique • 3.5 to 4 mm with the Transalveolar approach All gain in radio opaque areas in the sinus, observed on (CBCT), is “Vital” bone, with 0% substitute remnants.
- 48. When implants have to be placed in a second stage L-PRF can also be used, but it should be mixed with a bone substitute to delay its resorption. Lambert: • use of pure autologous bone resulted in greater loss of the augmented volume after 5 weeks A mixture (DBBM) and L-PRF resulted in more new bone formation than when DBBM was used exclusively.
- 49. Fibrin glue : newly formed epithelium L-PRF for the treatment of perforations of the schneiderian membrane 1. L-PRF membranes are resilient 2. Pliable 3. easy to manipulate 4. have an adhesive nature They have the capacity to seal the connection to the sinus in minutes
- 54. Rotary drill systems Piezoelectric bone surgery
- 55. 1. Outlining the bony window directly 2. Lateral wall erosion (0% perforation)
- 56. Tapping can be bother some patients with dense cortical bone and for those with loose trabecular bone benign paroxysmal positional vertigo (BPPV) patients must be able to open wide enough
- 57. benign paroxysmal positional vertigo
- 58. the most common intraoperative complication is perforation of the sinus membrane. • Smaller perforations : using Tissue Fibrin Glue • Larger perforations : achieved through a Lateral Window • Perforations before any grafting material procedure should be aborted or shorter implants used
- 59. Postoperative infections after transalveolar sinus lift are rare complications Postoperative hemorrhage Nasal bleeding Hematomas Loosening of cover screws resulting in: • Suppuration • (BPPV)
- 60. In the posterior maxilla: • High initial stability • Rough surface geometry. Implants with • Slightly conical morphometry or • implants with a Wider implant neck tend to give better primary stability
- 61. Residual bone height of ≥8 mm and a flat sinus floor: • standard implant placement
- 62. Residual bone height of ≥8 mm and an oblique sinus floor: • standard implant placement using a short implant • elevation of the maxillary sinus floor using the osteotome technique without grafting material
- 63. Residual bone height of 5–7 mm and a relatively flat sinus floor: • elevation of the maxillary sinus floor using the osteotome technique with grafting material that is resistant to resorption
- 64. Residual bone height of 5–7 mm and an oblique sinus floor: • elevation of the maxillary sinus floor using the lateral approach with grafting material, and simultaneous implant placement (one‐stage)
- 65. Residual bone height of 3–4 mm and a flat or oblique sinus floor: • elevation of the maxillary sinus floor using the lateral approach with grafting material, and simultaneous implant placement (one‐stage)
- 66. Residual bone height of 1–2 mm and a flat or oblique sinus floor: • elevation of the maxillary sinus floor using the lateral approach with grafting material and delayed implant placement 4–8 months later (two‐stage)