
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (19)
Destaque
Destaque (20)
Semelhante a Celebral Palsy
Semelhante a Celebral Palsy (20)
Mais de sangita_chosencaregroup
Mais de sangita_chosencaregroup (20)
Último
Último (20)
Celebral Palsy
- 2. Causes Cerebral palsy is due to damage occurring to the developing brain. This damage can occur during pregnancy, delivery, the first month of life, or less commonly in early childhood. Structural problems in the brain are seen in 80% of cases, most commonly within the white matter .More than three quarters of cases are believed to result from issues that occur during pregnancy.
- 3. Causes While in certain cases there is no identifiable cause, typical causes include problems in intrauterine development (e.g. exposure to radiation, infection),hypoxic of the brain, and birth trauma during labour and delivery, and complications around birth or during childhood.
- 4. Prematurity Between 40% and 50% of all children who develop cerebral palsy were born prematurely. Most of these cases (75-90%) are believed to be due to issues that occur around the time of birth, often just after birth. Multiple-birth infants are also more likely than single-birth infants to have CP. They are also more likely to be born with a low birth weight. In those who are born with a weight between 1 kg and 1.5 kg CP occurs in 6%.Among those born before 28 weeks of gestation it occurs in 11%. Genetic factors are believed to play an important role in prematurity and cerebral palsy generally. While in those who are born between 34 and 37 weeks the risk is 0.4% (three times normal).
- 5. Terminfants In babies that are born at term risk factors include: problems with the placenta, birth defects, low birth weight, breathing meconium into the lungs, a delivery requiring either the use of instruments or an emergency caesarean section, birth asphyxia, seizures just after birth, respiratory distress syndrome, low blood sugar, and infections in the baby. It is unclear how much of a role birth asphyxia plays as a cause. It is believed, however, that only a small number of cases are caused by lack of oxygen during birth. It is unclear if the size of the placenta plays a role.
- 6. Genetics About 2% of all CP cases are inherited, with glutamate decarboxylase -1 being one of the possible enzymes involved. Most inherited cases are autosomal recessive, meaning both parents must be carriers for the disorder in order to have a child with the disease.
- 7. Early childhood After birth, other causes include toxins, severe jaundice, lead poisoning, physical brain injury, shaken baby syndrome, incidents involving hypoxia to the brain (such as near drowning), and encephalitis or meningitis. The three most common causes of asphyxia in the young child are: choking on foreign objects such as toys and pieces of food, poisoning, and near drowning.
- 8. Other Infections in the mother, even infections that are not easily detected, may triple the risk of the child developing the disorder. Infections of the fetal membranes known as chorioamnionitis increases the risk. Intrauterine and neonatal insults (many of which are infectious in nature) increase the risk. It has been hypothesised that many cases of cerebral palsy are caused by the death in very early pregnancy of an identical twin.
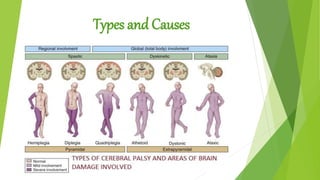
- 9. Types Physiological Grouping Spasticity Spasticity is defined as a velocity-dependent increased muscle tone, determined by passively flexing and extending muscle groups across a joint. A satisfactory, reproducible system of grading muscle tone has never been developed, although the Ashworth and Tardieu scales are commonly used in research. Most physicians describe the tone as being normal, increased or decreased. Associated with spasticity are enhanced deep tendon reflexes, usually associated with clonus and extensor plantar responses. However, the latter are sometimes difficult to elicit in the infant and even in the older child with spastic CP.
- 10. Dyskinesia Dyskinesia is defined as abnormal motor movements that become obvious when the patient initiates a movement. When the patient is totally relaxed, usually in the supine position, a full range of motion and decreased muscle tone may be found.
- 11. Dyskinesia patients are subdivided into twosubgroups The hyperkinetic or choreo-athetoid children show purposeless, often massive involuntary movements with motor overflow, that is, the initiation of a movement of one extremity leads to movement of other muscle groups. The dystonic group manifest abnormal shifts of general muscle tone induced by movement. Typically, these children assume and retain abnormal and distorted postures in a stereotyped pattern. Both types of dyskinesia may occur in the same patient. Simply stated, spasticity you feel; dystonia you see.
- 12. Dyskinesia Ataxias Patients with ataxias have a disturbance of the coordination of voluntary movements due to muscle dyssynergia. These patients may be hypotonic during the first two or three years of life. They commonly walk with a wide-based gait and have a mild intention tremor (dysmetria).
- 13. Dyskinesia Mixed Group The fourth category that is commonly used in the physiologic and motor classification is the mixed group. Patients in this category commonly have mild spasticity, dystonia, and/or athetoid movements. Ataxia may also be a component of the motoric dysfunction in patients placed in this group.
- 14. AnatomicGrouping Diplopia refers to involvement predominantly of the legs.
- 15. Quadriplegia Quadriplegia refers to dysfunction of all four extremities; in some children one upper extremity might be less involved; the term triplegia then would be substituted
- 16. Hemiplegia Hemiplegia refers to individuals with unilateral motor dysfunction; and in most children the upper extremity is more severely involved than the lower. Finally, an unusual situation may occur where the upper extremities are much more involved than the lowers; the term double hemiplegia is applied to this group of patients.