Translating Best Practices in Risk Communication and Product Labeling to ENDS Battery Safety
•Transferir como PPTX, PDF•
3 gostaram•1,078 visualizações

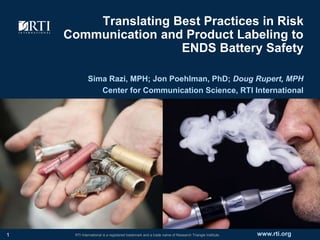
The batteries in e-cigarettes and other vape products can explode if charged or handled improperly, and there have been multiple reports of battery explosions, burns, and shocks. The U.S. Food and Drug Administration hosted a public workshop on Battery Safety Concerns in Electronic Nicotine Delivery Systems (ENDS) in April 2017, and during the workshop, RTI International’s Center for Communication Science showcased best practices for educating consumers about ENDS battery safety and strategies for promoting safe battery behaviors.

Recomendados
Mais conteúdo relacionado
Semelhante a Translating Best Practices in Risk Communication and Product Labeling to ENDS Battery Safety
Semelhante a Translating Best Practices in Risk Communication and Product Labeling to ENDS Battery Safety (15)
Último
Último (20)
Translating Best Practices in Risk Communication and Product Labeling to ENDS Battery Safety
- 1. www.rti.orgRTI International is a registered trademark and a trade name of Research Triangle Institute. Translating Best Practices in Risk Communication and Product Labeling to ENDS Battery Safety Sima Razi, MPH; Jon Poehlman, PhD; Doug Rupert, MPH Center for Communication Science, RTI International 1
- 2. Safe Practices for ENDS Batteries Vape within the amp limit Store batteries in protective cases Don’t store batteries in cars or pockets, near flammable items Avoid excessive temperatures (hot or cold) Use correct charger Replace batteries every 3-6 months 2
- 3. Challenges to Promoting Safe Battery Behavior Scope of unsafe behaviors is unknown Consumer awareness of battery risks not fully examined Limited understanding of why users adopt unsafe behaviors No testing of warning labels 3
- 4. Applying Best Practices Part 1: Product Labeling Best practices in product labeling and risk communication from prescription drug literature Part 2: Consumer Education Best practices in risk communication and behavior change more broadly 4
- 6. Methods 6 Literature Review Date Range 1997 – Present (20 years) Language English only Location U.S. only Keywords (1st tier) Drug n Prescription n Prescription drug n Medication Keywords (2nd tier) Risks n Risk information n Side effects n Adverse events n Label n Error Keywords (3rd tier) Comprehension n Understanding n Perception n Communication n Education Publications Found 120 Abstracts Reviewed 25 Final Pubs Reviewed 21
- 7. Best Practice #1 – Plain Language Plain language labels boost consumer comprehension Plain language elements: Active voice (not passive) Simple sentences Concise / No excess words Direct language (“you” and other pronouns) Bulleted lists or checklists Conversational tone (like you speak) Examples 7 Source: CommunicateHealth http://communicatehealth.com
- 8. Best Practice #1 – Plain Language Before Your initial evaluation may take up to one hour. During the evaluation, your therapist will provide appropriate testing and discuss various treatment strategies designed to help you reach your optimal state of health and function. It is advised that you wear comfortable and loose clothing for this initial evaluation. If your legs or feet are being examined, gym shorts are recommended. After Your first appointment will take about one hour. We will do some tests and talk about your treatment options. Please wear comfortable, loose clothes. If we are looking at your legs or feet, please wear shorts. 8
- 9. Best Practice #2 – Explicit Instructions Explicit Instructions Tell consumers what to do (rather than what not to do) Avoid ambiguity and complexity Before Take two pills twice a day prior to meals. Avoid taking on an empty stomach. After Take two pills before breakfast and two pills before dinner. Be sure to eat soon after taking the pills. 9 7-9 AM 12-2 PM 4-6 PM 9-11 PM 2 pills -- 2 pills --
- 10. Best Practice #2 – Explicit Instructions Before VapeMist XXL is not compatible with other batteries, chargers, or accessories. Batteries may become unstable after 3-6 months of continued use. After Use the charger that came in the VapeMist XXL box to re-charge your batteries. Replace the batteries every 3 months. Use only 50 Amp, 2600 mah batteries: Other batteries won’t work. 10 Amp mah 50 2600
- 11. Best Practice #3 – Low Literacy Structure and Formatting Low-literacy structure reduces cognitive burden, improves comprehension Features of low-literacy structure: Headings / Distinct sections Ample white space Easy to scan Large font size Bulleted lists or checklists 11
- 12. Best Practice #3 – Low Literacy Structure and Formatting 12 Version A Version B
- 13. Best Practice #4 – Icons and Visuals Icons and visuals can improve comprehension under right conditions: Recognizable / Intuitive Compatible with text Tested with audience Culturally appropriate 13
- 14. Best Practice #5 – Numeric Risk Information Numeric information improves consumer understanding of risks Visual depictions of risk are helpful No format or type of visual performs best 14 Risk of Explosion Unsafe Battery Storage Risk of Explosion Safe Battery Storage
- 15. Best Practice #6 – Negative Framing Consumers more attuned to risks when they are framed negatively Positive frame = Focus on potential gain Negative frame = Focus on potential loss Positive Frame If you store your batteries safely, your vape pen will almost always work when you need it. Negative Frame If you don’t store your batteries safely, your vape pen can explode or catch fire. 15
- 17. Ideal Consumer Behavior (Deficit Model) 17 Risk Information Awareness Heightened Risk Perception Protective Behavior
- 18. Real-Life Consumer Behavior 18 Consumer Behavior Self-efficacy Behavioral Beliefs Risk Perceptions Perceived Severity Perceived Susceptibility Benefits vs. Costs Cues to Action Behavioral Intentions Subjective Norms Motivation to Comply Outcome Expectations Previous Experience Self Motivation Environmental Factors Interpersonal Relationships Incentives Perceived Barriers Perceived Facilitators Stage of Change Communication Channels Relative Advantage Complexity Trialability Compatibility Knowledge Response Efficacy
- 19. Risk communication is a necessary but insufficient step for behavior change “Although people may need to have more information or to have information presented more clearly, a focus on knowledge alone often is insufficient for achieving communication goals.” - Communicating Science Effectively: A Research Agenda (National Academies Press, 2017) 19
- 20. Best Practice #1 – Listen to Your Audience Campaigns that leverage stakeholder input are more authentic and believable Understand audience needs, perceptions, and behavior Involve audience in planning process Push audience to develop solutions 20
- 21. Best Practice #2 – Reframe Messages What messages will resonate with your audience? Focus on underlying motivations for behavior Safety may not be important to them Be disruptive 21
- 22. Best Practice #3 – Audience Segmentation Divide audience into segments with similar beliefs, behaviors, motivations, and information needs Customize messages for each segment 22 Safety Convenience Cost
- 23. Best Practice #4 – Multiple Channels Disseminate messages through multiple communication channels Identify trusted and credible sources Leverage mix of channels: Interpersonal Broadcast Digital Point-of-action 23
- 24. Next Steps Formative Research. Investigate consumer battery behavior, including motivations and barriers to change. Warning Labels. Create warning labels based on best practices from other fields and test labels with consumers. Consumer Education. Identify audience segments, develop customized messages, and disseminate through trusted channels. 24
- 25. References Bailey, S.C., Navaratam, P., Black, H. et al. (2015). Advancing best practices for prescription drug labeling. Annals of Pharmacotherapy, 49(11), 1222-1236. Blalock, S.J., & Dixon, M. (2016). Effect of quantitative information concerning medication side-effects on risk perception. Presented at the American College of Rheumatology, Washington, D.C. Davis, T.C., Federman, A.D., Bass, P.F., et al. (2009). Improving patient understanding of prescription drug label instructions. Journal of General Internal Medicine, 24(1), 57-62. Davis, T.C., Wolf, M.S., Bass, P.F., et all. (2006). Low literacy impairs comprehension of prescription drug warning labels, Journal of General Internal Medicine, 21(8), 847-851. Katz, M.G., Kripalani, S., & Weiss, B.D. (2006). Use of pictorial aids in medication instructions: A review of the literature. American Journal of Health Systems Pharmacy, 62(23), 2391-97. Kebodeaux, C., Peters, G., Kindermann, H. et al. (2016). Patient-perceived content and formatting expectations for prescription container labeling. Journal of the American Pharmacists Association, 56(3), 242-247. King, J.P., Davis, T.C., Bailey, S.C., et al. (2011). Developing consumer-centered, nonprescription drug labeling a study in acetaminophen. American Journal of Preventive Medicine, 40(6), 593-598. Law, A.V., & Zargarzadeh, A.H. (2010). How do patients read, understand and use prescription labels? An exploratory study examining patient and pharmacist perspectives. International Journal of Pharmacy Practice, 18(5): 282-289. Locke, M.R., & Shiyanbola, O.O., & Gripentrog, E. (2014). Improving prescription auxiliary labels to increase patient understanding. Journal of the American Pharmacists Association, 54(3), 267-274. Masland, M.C., Kang, S.H., & Ma, Y. (2011). Association between limited English proficiency and understanding prescription labels among five ethnic groups in California. Ethnicity & Health, 16(2), 125-144. McCormack, L., Lefebvre, R.C., Bann, C., et al. (2016). Consumer understanding, preferences, and responses to different versions of drug safety messages in the United States: A randomized controlled trial. Drug Safety, 39(2), 171-184. Murty, S., & Sansgiry, S.S. (2007). Consumer comprehension of OTC medication labels and the scope for improvement in font size. Journal of Pharmacy Technology, 23, 207-213. 25
- 26. References Peters, E., Hart, P.S., & Fraenkel, L. (2011). Informing patients: The influence of numeracy, framing, and format of side effect information on risk perceptions. Medical Decision Making, 31(3), 432-436. Shiffman, S., Gerlach, K.K., Sembower, M.A., Rohay, J.M. (2011). Consumer understanding of prescription drug information: An illustration using an antidepressant medication. Annals of Pharmacotherapy, 45(4), 452-458. Shrank, W., Avorn, J., Rolon, C., & Shekelle, P. (2007). Effect of content and format of prescription drug labels on readability, understanding, and medication use: A systematic review. Annals of Pharmacotherapy, 41(5), 783-801. Vigilante, W.J., & Wogalter, M.S. (1998). Older adults' perceptions of OTC drug labels: Print size, white space and design type. In Kumar, S., Advances in Occupational Ergonomics and Safety. West, S.L., Squiers, L.B., McCormack, L., et al. (2013). Communicating quantitative risks and benefits in promotional prescription drug labeling or print advertising. Pharmacoepidemiology and Drug Safety, 22(5), 447-458. Wolf, M.S., Davis, T.C., Bass, P.F., et al., (2010). Improving prescription drug warnings to promote patient comprehension. Archives of Internal Medicine, 170(1), 50-56. Wolf, M.S., Davis, T.C., Curtis, L.M., et al. (2011). Effect of standardized, patient-centered label instructions to improve comprehension of prescription drug use. Medical Care, 49(1), 96-100. Wolf, M.S., Davis, T.C., Shrank, W., et al. (2007). To err is human: Patient misinterpretations of prescription drug label instructions. Patient Education and Counseling, 67(3), 293-300. Wolf, M.S., Davis, T.C., Tilson, H.H., et al. (2006). Misunderstanding of prescription drug warning labels among patients with low literacy. American Journal of Health System Pharmacy, 63(11), 1048-1055. 26
- 27. Contact Information 27 Doug Rupert, MPH Center for Communication Science RTI International PHONE: (919) 541-6495 EMAIL: drupert@rti.org TWITTER: @DougRupertMPH