South University College of Nursing and Public Health Graduate Online
Nursing Program
Aquifer Internal Medicine
Internal
Medicine
08: 55-year-
old male
with chronic
disease
management
Author/Editor:Author/Editor: Cynthia A. Burns, MD
INTRODUCTION HISTORY
You review Mr. Morales' records on the computer.You review Mr. Morales' records on the computer.
!
You are working with Dr. Clay in her outpatient diabetes clinic this morning.
https://southu-nur.meduapp.com/
https://southu-nur.meduapp.com/document_sets/6094
Your first patient, Mr. Morales, was seen by Dr. Clay once before, eight years ago,
but was lost to follow-up after that time.
Based on review of the electronic medical record you are able to collect the
following information prior to heading into the room to meet Mr. Morales:
Mr. Morales is a 55-year-old Hispanic male, diagnosed with Type 2 diabetes
mellitus thirteen years ago after experiencing a 20-pound unintentional weight
loss, blurry vision, and nocturia.
He was hospitalized six weeks ago with a non-ST elevation myocardial infarction
and required three vessel coronary artery bypass grafting. During his admission,
he was found to have a reduced ejection fraction of 20%.
He was referred for today's visit by the cardiologist to focus on optimizing his
glycemic control and reducing his risk of the comorbidities associated with poorly
controlled Type 2 diabetes mellitus.
His last hemoglobin A1c (HbA1c) was 9.5% eight years ago, and he had
microalbuminuria at that time.
DIABETES CHRONIC DISEASE
MANAGEMENT 1
MANAGEMENT
You review diabetes chronic disease management with Dr. Clay.You review diabetes chronic disease management with Dr. Clay.
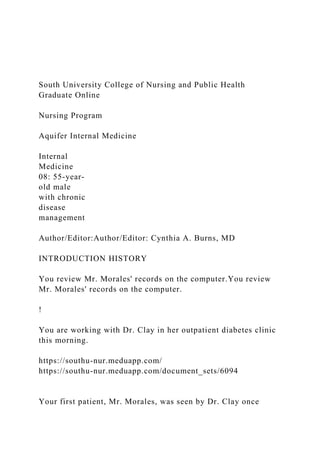
!
Before you see Mr. Morales, Dr. Clay reviews diabetes chronic disease
management with you.
Diabetes Chronic Disease Management
Evaluate for and optimize prevention of diabetic complicationsEvaluate for and optimize prevention of diabetic complications
Macrovascular complications:
Cardiovascular disease
Cerebrovascular disease
Microvascular complications:
Retinopathy
Nephropathy
Neuropathy
In particular, cardiovascular disease is the No. 1 cause of mortality for people
with diabetes, and one of the top causes of morbidity.
Hypoglycemia, infections, foot ulcers, and amputations are additional causes of
morbidity and mortality in patients with diabetes.
The American Diabetes Association publishes annual guidelines to assist in the
management of a patient with diabetes.
Remember the large role that the psychosocial aspects of a diabetesRemember the large role that the psychosocial aspects of a diabetes
diagnosis play in managementdiagnosis play in management
Non-adherence with medical recommendations could be due to economic,
work-related, religious, social, or linguistic barriers to care. Care must be taken
to assess the psychosocial status of each person with diabetes at each clinic
visit to ensure that barriers to successful diabetes care are minimized.
Question
Which .
South University College of Nursing and Public Health Graduate.docx
1. South University College of Nursing and Public Health
Graduate Online
Nursing Program
Aquifer Internal Medicine
Internal
Medicine
08: 55-year-
old male
with chronic
disease
management
Author/Editor:Author/Editor: Cynthia A. Burns, MD
INTRODUCTION HISTORY
You review Mr. Morales' records on the computer.You review
Mr. Morales' records on the computer.
!
You are working with Dr. Clay in her outpatient diabetes clinic
this morning.
https://southu-nur.meduapp.com/
https://southu-nur.meduapp.com/document_sets/6094
Your first patient, Mr. Morales, was seen by Dr. Clay once
2. before, eight years ago,
but was lost to follow-up after that time.
Based on review of the electronic medical record you are able to
collect the
following information prior to heading into the room to meet
Mr. Morales:
Mr. Morales is a 55-year-old Hispanic male, diagnosed with
Type 2 diabetes
mellitus thirteen years ago after experiencing a 20-pound
unintentional weight
loss, blurry vision, and nocturia.
He was hospitalized six weeks ago with a non-ST elevation
myocardial infarction
and required three vessel coronary artery bypass grafting.
During his admission,
he was found to have a reduced ejection fraction of 20%.
He was referred for today's visit by the cardiologist to focus on
optimizing his
glycemic control and reducing his risk of the comorbidities
associated with poorly
controlled Type 2 diabetes mellitus.
His last hemoglobin A1c (HbA1c) was 9.5% eight years ago,
and he had
microalbuminuria at that time.
DIABETES CHRONIC DISEASE
MANAGEMENT 1
MANAGEMENT
You review diabetes chronic disease management with Dr.
3. Clay.You review diabetes chronic disease management with Dr.
Clay.
!
Before you see Mr. Morales, Dr. Clay reviews diabetes chronic
disease
management with you.
Diabetes Chronic Disease Management
Evaluate for and optimize prevention of diabetic
complicationsEvaluate for and optimize prevention of diabetic
complications
Macrovascular complications:
Cardiovascular disease
Cerebrovascular disease
Microvascular complications:
Retinopathy
Nephropathy
Neuropathy
In particular, cardiovascular disease is the No. 1 cause of
mortality for people
with diabetes, and one of the top causes of morbidity.
Hypoglycemia, infections, foot ulcers, and amputations are
additional causes of
morbidity and mortality in patients with diabetes.
The American Diabetes Association publishes annual guidelines
4. to assist in the
management of a patient with diabetes.
Remember the large role that the psychosocial aspects of a
diabetesRemember the large role that the psychosocial aspects
of a diabetes
diagnosis play in managementdiagnosis play in management
Non-adherence with medical recommendations could be due to
economic,
work-related, religious, social, or linguistic barriers to care.
Care must be taken
to assess the psychosocial status of each person with diabetes at
each clinic
visit to ensure that barriers to successful diabetes care are
minimized.
Question
Which of the following does the American Diabetes Association
recommend to minimize the risk of cardiovascular disease in
patients
with diabetes? Select all that apply.
TEACHING POINTTEACHING POINT
http://care.diabetesjournals.org/content/41/Supplement_1
The best options are indicated below. Your selections are
indicated by
the shaded boxes.
A. Smoking cessation
B. Daily aspirin therapy
5. C. Blood pressure less than 140/90 mmHg (if it can be
achieved without increased treatment burden, a systolic target
of < 130
is appropriate in younger, healthier patients)
D. If > 40 years old, regardless of other atherosclerotic
cardiovascular disease risk factors, statin therapy
SUBMITSUBMIT
Answer Comment
> The correct answers are A, B, C, D> The correct answers are
A, B, C, D
ADA Recommendations to Minimize the Risk of
Cardiovascular Disease in Patients with Diabetes
Smoking cessationSmoking cessation, daily aspirindaily aspirin,
blood pressure controlblood pressure control and
lipid controllipid control are all recommended to reduce the risk
of
cardiovascular disease.
Please note that as of 2018, ADA recommendations were
published
with the older definition of hypertension (140/90). It always
takes time
before multiple different organizations agree on the same
thresholds.
Daily low dose aspirin is recommended for primary prevention
of
cardiovascular disease in diabetic patients with a 10-year risk of
atherosclerotic cardiovascular disease of >10%. It is also
6. recommended for secondary prevention of all diabetic patients
with a
history of atherosclerotic disease.
Reduction of cardiovascular risk is achieved with a goal of
optimal
glycemic control, as well as control of many other health factors
that
raise cardiovascular risk, such as tobacco use, obesity, poorly
controlled hypertension, and hypercholesterolemia.
TEACHING POINTTEACHING POINT
References
Economic Costs of Diabetes in the U.S. in 2012. American
Diabetes Association. Diabetes Care. April
2013; 36(4):1033-1046.
http://care.diabetesjournals.org/content/36/4/1033. Accessed
May 11, 2018.
PATIENT HISTORY HISTORY
Mr. Morales tells you about his heart attack.Mr. Morales tells
you about his heart attack.
!
You enter the exam room and introduce yourself to Mr.
Morales.
"What brought you to the oRce today?"
"I had a heart attack about a month ago and had to have open-
heart surgery.
The heart doctors told me that my heart is weak now. My
7. cardiologist told me
that I have to get my blood sugar under control so I don't have
another heart
attack. I am here to get down to work."
"Tell me more about that."
"I didn't come back to see Dr. Clay because my job at the
furniture factory
wouldn't give me time off for clinic appointments, and I
couldn't risk losing
" DEEP DIVEDEEP DIVE
http://care.diabetesjournals.org/content/36/4/1033
The best option is indicated below. Your selections are
indicated by the
shaded boxes.
my job. I wasn't checking my blood sugar before my heart
attack because the
testing strips are so expensive and my supervisor wouldn't let
me off the line
to check anyway. Since my surgery, I haven't gone back to
work, and I've
been checking my sugar before each meal and before bed. The
hospital
social worker got me two months' worth of testing strips and
lancets before I
went home, but I'm going to run out in a couple of weeks. I'm
worried that I
won't be able to check anymore."
He also tells you that while he was in the hospital, they had to
use insulin through
8. his vein to keep his blood sugar controlled, and that was very
upsetting to him.
Question
True or False: In a critically ill medical patients, tight blood
sugar control
with intravenous insulin therapy, with a goal blood sugar of 80-
110
mg/dL, is associated with lower mortality than less tight blood
sugar
control (e.g. 140-180 mg/dL).
A. True
B. False
SUBMITSUBMIT
Answer Comment
> The correct answer is B> The correct answer is B
EUectiveness of Intravenous Insulin for Blood Glucose
Control
Blood sugar control in critically ill patients has been the subject
of
considerable investigation. Previous research suggested that
tight
control (80-120 mg/dL) was desirable, but more recent research
shows
that aggressive blood sugar control can be associated with
higher
mortality.
Hypoglycemia (serum glucose concentration <70 mg/dL), with
rates as
high as 40% in some studies, is associated with tight glycemic
9. control.
TEACHING POINTTEACHING POINT
A meta-analysis of 29 controlled trials involving more than
8,000 adult
ICU patients showed no difference in in-hospital mortality
between the
group assigned to tight glucose control versus usual care.
The current recommended blood glucose target for mostThe
current recommended blood glucose target for most
hospitalized patients is 140 to 180 mg/dL.hospitalized patients
is 140 to 180 mg/dL.
References
Wiener RS, Wiener DC, Larson RJ. Benefits and risks of tight
glucose control in critically ill adults: a
meta-analysis. JAMA. 2008;300(8):933.
MEDICATION REVIEW HISTORY
You review Mr. Morales' medications with him:
MedicationsMedications
metformin 1000 mg twice daily
pioglitazone 15 mg daily
glipizide 5 mg daily
aspirin 81 mg daily
clopidogrel 75 mg daily
long-acting metoprolol 100 mg daily
furosemide 80 mg twice daily
lisinopril 20 mg daily
amlodipine 10 mg daily
10. ranitidine 150 mg twice daily
gabapentin 300 mg twice daily
potassium chloride 10 mEq twice daily
atorvastatin 80 mg daily
Mr. Morales says, "The hospital doctors sent me home on an
insulin shot - 40 units
in my belly every night before I go to bed. I don't like giving
myself the shot, so
sometimes I just don't, but I take all the rest of my medicines
like they told me to."
He takes out the vial of insulin, and you see that it is insulin
glargine.
Question
The best option is indicated below. Your selections are
indicated by the
shaded boxes.
Which of the following medications should you consider
discontinuing in
this patient based on your knowledge of his reduced ejection
fraction?
Choose the single best answer.
A. Pioglitazone
B. Atorvastatin
C. Aspirin
D. Glipizide
11. SUBMITSUBMIT
Answer Comment
> The correct answer is A> The correct answer is A
Thiazolidinediones
Pioglitazone (A),Pioglitazone (A), a member of the class of
drugs known as
thiazolidinediones (TZD), is not recommended for use in
patients who
have newly developed heart failure and in those with known
NYHA
Class III and IV heart failure. The same is true for
rosiglitazone, another
TZD that has been associated with an increased risk of
cardiovascular
disease.
Mechanism of action:Mechanism of action: TZDs are
peroxisome proliferator-activated
receptor-gamma (PPARgamma) agonists.
Effects:Effects: TZDs decrease insulin resistance, increase
glucose uptake in
peripheral tissue, decrease hepatic glucose production, decrease
vascular inflammation, redistribute visceral adipose tissue
peripherally, and preserve beta cell function. Overall, they
cause the
A1c to decrease by 1% to 1.5%. Hypoglycemia is not associated
with
this medication class. TZDs have differing effects on lipids.
Pioglitazone slightly reduces LDL levels and raises HDL.
Rosiglitazone
can increase LDL levels.
12. Side effects:Side effects: The receptors that TZDs activate are
ubiquitous and are
TEACHING POINTTEACHING POINT
abundant in the cells within the renal collecting tubules. Hence,
TZDs
increase sodium reabsorption, leading to increased water
retention.
Compared to placebo, all TZDs are associated with a
statistically
significant increase in edema and weight.
Warnings:Warnings: Care should be used with these agents in
patients with
liver disease. Serum transaminases greater than 2.5 times the
upper
limit of normal is a contraindication to initiation of these
agents, and a
rise to greater than three times the upper limit of normal should
lead
to their discontinuation. Liver tests should be measured at
baseline
and periodically while the patient is on this class of medication.
Contraindications:Contraindications: The FDA has added a
warning to the label of
pioglitazone noting an increased risk of bladder cancer after
more
than one year of treatment. Pioglitazone is now contraindicated
in
patients with a history of bladder cancer or active bladder
cancer.
Patients should be counseled to tell their physician if they
13. notice blood
in their urine or a red tint to their urine.
No precautions are needed when using aspirin, glipizide, or
simvastatin
in patients with a reduced ejection fraction.
BLOOD GLUCOSE MONITORING HISTORY
" DEEP DIVEDEEP DIVE
!
You continue your interview with Mr. Morales and ask him:
"Have you brought your blood sugar log with you today?"
He hands you his blood sugar log proudly. Over the last four
weeks, you see
that his morning fasting readings are ranging 130-169 mg/dL,
including
before-lunch readings of 151-247 mg/dL, before-supper
readings of 184-211
mg/dL, and before-bed readings of 158-305 mg/dL. There are no
recorded
readings under 70 mg/dL (3.9 mmol/L).
"Some days you have many readings over 200 mg/dL. Is there
anything
diUerent going on on those days that you can think of such as
eating larger meals?"
"Oh, those are the days after I didn't take my insulin shot. The
readings are
always higher on those days."
14. "Have you had any low blood sugars?"
"I feel like I have low blood sugar several times a week, and I
eat a Snickers
bar because I'm afraid of passing out and going into a coma. I
feel like I'm
going to die -- shaky, sweaty, jittery! I don't check when I feel
this way, I just
eat as fast as I can - I can tell when my sugar is low."
See the associated reference ranges in conventional and SI
units.
https://www.meduapp.com/resources/laboratory_reference_valu
es
The best option is indicated below. Your selections are
indicated by the
shaded boxes.
Hypoglycemia
It is important at each visit to ask diabetic patients if they have
experienced any
hypoglycemic symptoms or events that required the assistance
of another
person.
Often times, when a patient is hypoglycemic, he does not write
it down because
he is preoccupied treating the hypoglycemia.
When to Refer Patients with Diabetes to an Endocrinologist
If a patient is having recurrent or severe hypoglycemia (seizure,
coma, or
impairment that requires the aid of another person), an
endocrinologist should
15. be consulted. Hypoglycemia is defined as a blood glucose <70
mg/dL.
Primary care physicians' threshold for referral varies across
providers. Other
conditions that would warrant referral are when a patient's A1c
is 8% more than
twice in a 12-month period, despite intensive treatment; for
initiation of a
complex multiple daily injection insulin regimen; or for
initiation of continuous
infusion insulin pump therapy.
Question
Can patients accurately detect hypoglycemia by symptoms
alone?
A. Yes
B. No
SUBMITSUBMIT
Answer Comment
> The correct answer is B> The correct answer is B
Self-Monitoring Glucose: Indications & EUectiveness
TEACHING POINTTEACHING POINT
TEACHING POINTTEACHING POINT
TEACHING POINTTEACHING POINT
16. Self-Monitoring Glucose: Indications & EUectiveness
Effectiveness of Self-Monitoring Blood GlucoseEffectiveness of
Self-Monitoring Blood Glucose
Patients should be advised to check their blood sugar if they
feel "low"
because it is well recognized that people are not able topeople
are not able to
accurately detect hypoglycemia (blood glucose of < 70
mg/dL)accurately detect hypoglycemia (blood glucose of < 70
mg/dL)
by symptoms aloneby symptoms alone. Eating high
carbohydrate food to treat
perceived hypoglycemia rather than actual hypoglycemia leads
to
worsened overall glycemic control.
Clinical studies have shown that self-monitoring of blood
glucose
(SMBG) may improve glycemic control, although for some
patients
self-monitoring increases depression and anxiety. It is important
to
evaluate patients' abilities to use SMBG techniques to ensure
they are
using accurate data to evaluate their response to therapy and
their
degree of success in reaching blood-glucose targets. After
receiving
education, patients can use SMBG data to adjust their activity
level,
food intake and choice, as well as drug therapy to achieve
optimal
glycemic control.
When to Self-Monitor Blood GlucoseWhen to Self-Monitor
17. Blood Glucose
In patients on less frequent insulin injections, SMBG may be
useful in
achieving glycemic goals.
Patients on an insulin pump and those using multiple daily
insulin
injections should self-monitor blood glucose at the following
times:
before each meal
at bedtime
when they have symptoms of hyper- or hypoglycemia
after treating hypoglycemia to ensure return of euglycemia
before exercise
before critical activities, such as driving
Blood Glucose Goals
HealthyHealthy *Medically*Medically
**Very**Very
MedicallyMedically
TEACHING POINTTEACHING POINT
AdultsAdults ComplexComplex
AdultsAdults
ComplexComplex
AdultsAdults
fasting andfasting and
beforebefore
18. mealsmeals
80-130
mg/dL (3.9-
7.2 mmol/L)
90-150
mg/dL
100-180 md/dL
one to twoone to two
hours afterhours after
a meala meal
< 180 mg/dL
(10.0
mmol/L)
before bedbefore bed
100-130
mg/dL (5.6-
7.2 mmol/L)
100-180
mg/dL
110-200 mg/dL
*Medically complex adults have multiple co-existing chronic
illnesses,
two or more ADL impairments, or mild to moderate cognitive
impairment.
**Very medically complex adults or adults in poor health have
long
19. term care or end-stage chronic illnesses, moderate to severe
cognitive
impairment, or two or more ADL dependencies.
See the associated reference ranges in conventional and SI
units.
DIET HISTORY HISTORY
You ask Mr. Morales about diet and physical activity.
"Can you tell me what you typically eat in a day?"
"I usually eat breakfast and lunch at McDonald's or Denny's.
For breakfast, I
usually have a bacon egg and cheese biscuit with hash browns
and black
coffee. For lunch, I have a sandwich, fries, and soda. If I'm
really hungry, I get
the "value" size of the fries and soda."
" DEEP DIVEDEEP DIVE
https://www.meduapp.com/resources/laboratory_reference_valu
es
The best options are indicated below. Your selections are
indicated by
the shaded boxes.
"What drinks and snacks do you typically eat during the day?"
"I drink Coke with lunch, whole milk with supper, and usually
have a big bowl
of fudge ripple ice cream before I go to bed. If I'm hungry in
the afternoon, I'll
grab a pack of cookies from a vending machine."
20. "And what do you have for dinner?"
"My wife and I eat supper at home. We share the cooking.
Usually, we have
fried or stewed meat with gravy, rice, or pasta along with rolls.
Sometimes we
have vegetables cooked with side meat."
"Are you able to do any exercise during the week?"
"Except for moving around at work, I didn't get much exercise
before. Since
my heart surgery, I feel short of breath just walking to the
mailbox at the end
of the driveway!"
"Do you have any chest pain or sweating?"
"Not really."
SCREENING FOR COMPLICATIONS HISTORY
You now decide to focus your history on screening for
complications of diabetes:
"Are you having any trouble with your vision?"
"How about numbness or tingling in your hands or feet?"
Question
Which of the following are types of neuropathies a patient with
diabetes
might develop? Select all that apply.
A. Distal symmetric polyneuropathy
B. Postural hypotension
21. C. Gastroparesis
D. Erectile dysfunction
E. Resting tachycardia
SUBMITSUBMIT
Answer Comment
> The correct answers are A, B, C, D, E> The correct answers
are A, B, C, D, E
Diabetic Neuropathies
It is estimated that 50% of patients with diabetes will eventually
struggle with one or more neuropathies related to their diabetes.
Axonal loss and atrophy are responsible for the majority of
clinical
symptoms and loss of function in patients with neuropathy.
There can
also be evidence of demyelination and remyelination, with the
actual
number of large nerve fibers being reduced, while small nerve
fibers
increase.
Distal polyneuropathyDistal polyneuropathy
Distal polyneuropathy is the most common type of diabetic
neuropathy. It is the progressive loss of sensation in the classic
stocking/glove distribution. Diabetic foot ulcer incidence is
greatly
increased in patients with distal polyneuropathy.
Autonomic neuropathyAutonomic neuropathy
22. Autonomic neuropathy can take many forms and affect one or
many
organs. Specific types include:
cardiovascular (orthostatic hypotension, resting sinus
tachycardia,
postprandial hypotension)
gastrointestinal (gastroparesis, chronic constipation, esophageal
motility disorders)
genitourinary (sexual dysfunction, neurogenic bladder)
TEACHING POINTTEACHING POINT
abnormal pupillary responses and disorders of hidrosis
OBESITY MANAGEMENT MANAGEMENT
You leave the room so that Mr. Morales can disrobe for your
exam. Dr. Clay asks
what you have learned so far.
You present the history to Dr. Clay and tell her that you are
particularly concerned
about Mr. Morales' diet. You and Dr. Clay look at the triage
sheet and see that Mr.
Morales' height is 176.5 cm (69.5 inches) and his weight is 123
kg (272 lbs). You
calculate his BMI: it is 39.6 kg/m .2
Body Weight Management in Patients with Diabetes
ClassificationClassification BMI in kg/mBMI in kg/m22
23. Normal 19-24
Overweight 25-29
Obese 30-39
Morbidly obese 40+
Maintenance of a healthy body weight is essential in the
management of
patients with diabetes. However, for some patients, attainment
of an ideal body
weight is too large a goal, especially if they are morbidly obese.
Studies have
shown that a modest weight loss of approximately 5-10%modest
weight loss of approximately 5-10% of the current
weight can lead to significant improvement in glycemic control,
blood pressure
control, and lipid parameters.
Question
" DEEP DIVEDEEP DIVE
TEACHING POINTTEACHING POINT
The best options are indicated below. Your selections are
indicated by
the shaded boxes.
Which of the following are appropriate approaches to
addressing Mr.
Morales' obesity and diet? Select all that apply.
24. A. Referral to a registered nutritionist for medical nutrition
therapy.
B. Office-based, brief dietary counseling.
C. Referral to an accredited diabetes care center for diabetes
management self education.
D. Patient materials about diet and exercise.
SUBMITSUBMIT
Answer Comment
> The correct answers are A, B, C, D> The correct answers are
A, B, C, D
Mulitdisciplinary Approach to Diabetes Care
The care of the patient with diabetes is a team endeavor.
Through a
multidisciplinary approach, patients can be offered the very best
chance of optimizing their blood glucose control and reducing
their
risks of morbidity and mortality.
Refer to a registered nutritionist for medical nutrition therapy
regarding daily food choices and portion sizes.
Refer to an accredited diabetes care center for diabetes
management self-education, both in group and one-on-one
settings.
Numerous studies have shown that diabetes management self-
education is effective in improving patients' self-care behaviors,
lowering their A1c, improving their knowledge of diabetes and
enhancing their quality of life.
25. Office-based counseling of basic ADA recommendations for
diet and
exercise can be reviewed with the patient. For example, patients
can
be taught how to monitor his carbohydrate intake through
carbohydrate counting, food exchanges, or self-reflection.
Thirty
minutes of moderately intense exercise, more days than not,
may be a
good recommendation for many patients. Less than 10% of daily
TEACHING POINTTEACHING POINT
calories should be from fat.
Patient education materials are a useful adjunct to office-based
counseling, and can be found at the ADA website section on
diet/exercise.
BLOOD PRESSURE MANAGEMENT MANAGEMENT
You recheck Mr. Morales' blood pressure manually.You recheck
Mr. Morales' blood pressure manually.
!
You look at the rest of Mr. Morales' vital signs:
Vital signs:Vital signs:
Temperature:Temperature: 36.3 C (97.9 F)
Pulse:Pulse: 74 beats/minute
Respiratory rate:Respiratory rate: 12 breaths/minute
26. Blood pressure:Blood pressure: 152/86 mmHg today (148/92
mmHg at the cardiologist's office
two weeks ago)
Fingerstick blood glucose:Fingerstick blood glucose: 158 mg/dL
(8.8 mmol/L)
You retake his blood pressure manually and read 150/90 mmHg.
See the associated reference ranges in conventional and SI
units.
http://www.diabetes.org/food-and-
fitness/?utm_source=WWW&utm_medium=GlobalNavFF&utm_
campaign=CON
https://www.meduapp.com/resources/laboratory_reference_valu
es
The best option is indicated below. Your selections are
indicated by the
shaded boxes.
Question
Is this patient's blood pressure at goal?
A. Yes
B. No
SUBMITSUBMIT
Answer Comment
> The correct answer is B> The correct answer is B
Blood Pressure Goal for Patients with Diabetes
27. There is ample, well-validated evidence that blood pressure
control is
one way of lowering a diabetic patient's cardiovascular risk.
According
to the ADA, the optimal blood pressure goal in patients with
diabetes
is less than 140/90 mmHg. Younger, healthier patients who can
be
treated without increasing the treatment burden may have a
lower
systolic target, such as less than 130. It is important to
remember that
an individual patient's blood pressure goal may be higher or
lower
based on his/her response to therapy and personal
characteristics.
Note: Other organizations recommend different blood pressure
goals
for patients with diabetes, such as the ACC/AHA, which
recommends
treatment in people with diabetes who have blood pressure
greater
than or equal to 130/80 mmHg, with a goal blood pressure of
less than
130/80 mmHg.
The ACC/AHA guidelines on hypertension published in late
2017
suggested lower numbers for a definition of HTN; now anything
over
130/80 is considered hypertension per ACC/AHA. Other
organizations -
like ADA - have not yet updated their guidelines to reflect this
change.
Pharmaceutical managementPharmaceutical management
28. Most diabetic patients require multiple agents to reach and
maintain
their individual blood pressure goal. ACE inhibitor and ARB
therapy
TEACHING POINTTEACHING POINT
are first-line treatment options because they also delay the onset
and
decrease the progression of diabetic nephropathy. Diuretics and
calcium channel blockers can be used to attain blood pressure
goals.
Reasons for uncontrolled blood pressureReasons for
uncontrolled blood pressure
There are multiple reasons why a patient may have uncontrolled
blood pressure. Blood pressure may be uncontrolled in patients
needing increased dosages of their medications or additional
agents.
It may be elevated secondary to medications (e.g. NSAIDs) or
alcohol.
Or patients may not be taking their medications regularly, may
not
have taken their medications on the day of the office visit, or
may have
run out of their medication prior to the visit.
Before adding another medication or increasing the dose of
existing
medication, it is critical that nonadherence be explored first as a
possible cause of uncontrolled hypertension.
29. When asked about his adherence to his current regimen, Mr.
Morales
says he took all of his medications this morning and did not
miss any
doses of his medications in the past week.
PHYSICAL EXAM 1 PHYSICAL EXAM
You examine Mr. Morales' eyes.You examine Mr. Morales'
eyes.
!
You proceed with Mr. Morales' exam, paying special attention
to the fundoscopic
exam.
Physical ExamPhysical Exam
GeneralGeneral: Obese, older male in no apparent distress.
HEENTHEENT: Normocephalic, atraumatic. Oropharynx clear
and moist. Dentition and
dental hygeine good. Pupils equal and reactive to light and
accommodation.
Extraocular movements intact. No icterus.
Fundoscopic examFundoscopic exam: Several microaneurysms
bilaterally and hard exudates on
the left.
NeckNeck: Supple and thick. No increased JVD. No carotid
bruits. Carotid pulses 2+
bilaterally with normal upstroke. No thyromegaly or masses.
30. LungsLungs: Clear to auscultation bilaterally. No wheeze, rales,
or rhonchi.
CardiacCardiac: PMI diffuse and laterally displaced. Regular
rate and rhythm. Normal S1,
S2, no S3, no S4, no murmurs.
AbdomenAbdomen: Soft, nontender, nondistended, no
hepatosplenomegaly.
The best options are indicated below. Your selections are
indicated by
the shaded boxes.
Question
Which of the following are recommendations for the prevention
and
decreased progression of diabetic retinopathy? Select all that
apply.
A. Optimal blood pressure control
B. Optimal glucose control
C. Smoking cessation
D. Optimal LDL control
SUBMITSUBMIT
Answer Comment
> The correct answers are A, B, C> The correct answers are A,
B, C
31. Diabetic Retinopathy
Diabetic retinopathy, a microvascular diabetic complication, is
the
leading cause of preventable blindness in the developed world.
PreventionPrevention
Two large prospective trials (DCCT with Type 1 diabetics and
UKPDS
with Type 2 diabetics) revealed that intensive glucose
management
resulted in prevention or delayed onset and progression of
diabetic
retinopathy.
Co-existing hypertension, nephropathy, and tobacco abuse also
contribute to retinopathy onset and progression.
Two types of diabetic retinopathyTwo types of diabetic
retinopathy
1. Non-proliferative diabetic retinopathyNon-proliferative
diabetic retinopathy
Involves cotton wool spots, hard exudates, microaneurysms, and
retinal hemorrhages.
TEACHING POINTTEACHING POINT
https://medu-relier-
production.s3.amazonaws.com/files/SIMPLE-08-
c2HsB1o7coAFhzTur-
Z5A2MUkASComz6CQVw5pWjneKqY6ACxrW/compressed/im
ages/251192.jpg
32. Vision loss usually results from severe macular edema, a
thickening of
the retina with resultant edema of the macula.
2. Proliferative diabetic retinopathyProliferative diabetic
retinopathy
Involves neovascularization of the retinal vessels or optic disc,
retinal
hemorrhage (dot-blot, flame), retinal fibrosis with traction
detachment, and vitreous hemorrhage. Macular edema can occur
as
well.
Image of proliferative retinopathy with neovascularizationImage
of proliferative retinopathy with neovascularization
!
OnsetOnset
Development of diabetic retinopathy is directly related to
disease
duration and is generally not seen in patients who have had
diabetes
less than five years. The exception is Type 2 diabetic patients
who
were likely hyperglycemic more than five years prior to their
diabetes
diagnosis.
ScreeningScreening
Annual dilated eye exams by an ophthalmologist are
recommended
33. for all Type 1 diabetic patients within five years of diagnosis
and
shortly after diagnosis in patients with Type 2 diabetes. Patients
with
progressive retinopathy are often seen quarterly or biannually.
Panretinal TreatmentPanretinal Treatment
Panretinal laser photocoagulation is the treatment of choice for
proliferative diabetic retinopathy and severe cases of non-
proliferative
retinopathy. Screening is done aggressively due to the well-
documented efficacy of laser photocoagulation in the prevention
of
vision loss. Ranibizumab, an anti-vascular endothelial growth
factor,
injected into the vitreous showed noninferiority to laser therapy
and
can also be used.
PHYSICAL EXAM 2 PHYSICAL EXAM
You perform a diabetic foot exam on Mr. Morales.You perform
a diabetic foot exam on Mr. Morales.
!
You are glad you will have the opportunity to practice the
diabetic foot exam you
reviewed last night.
" DEEP DIVEDEEP DIVE
34. You proceed with Mr. Morales' exam:
Physical ExamPhysical Exam
Extremities:Extremities: Full range of motion without clubbing
or cyanosis. No peripheral
edema.
Diabetic foot exam:Diabetic foot exam: 1+ dorsal pedis and
posterior tibialis pulses bilaterally
with decreased sensation to monofilament and vibration to the
mid-shin. No
ulcers. + diffuse onychomycosis.
Neurologic:Neurologic: Awake, alert and oriented times four.
Cranial nerves II-XII are
grossly intact. Muscle strength is 5/5 throughout with normal
tone and bulk. Deep
tendon reflexes are trace throughout. Gait normal. No tremor.
When to Perform the Diabetic Foot Exam
It is important to do a thorough foot exam in a diabetic patient
on an annual
basis for low-risk patients and more often in patients at high
risk for foot ulcer
formation.
Patients at High Risk for foot Ulcer FormationPatients at High
Risk for foot Ulcer Formation
Patients with known diabetic polyneuropathy, sensory or
vascular deficits,
patients who smoke, and patients with a prior history of diabetic
foot ulcer or
35. amputation.
Foot Exam in Patients with Diabetes
Visually inspect the feet for callus formation, ulceration, nail
infections, and
bony deformities.
Assess skin integrity, especially between toes and under
metatarsal heads.
Palpate the dorsalis pedis and posterior tibialis pulses to screen
for peripheral
vascular disease and look for signs of peripheral vascular
disease, such as hair
loss.
Check sensation using a 128 Hz tuning fork (vibration) and a
cool metal object,
potentially the same tuning fork (temperature).
Check pressure sensation using a 10-g monofilament:
TEACHING POINTTEACHING POINT
TEACHING POINTTEACHING POINT
Show the monofilatment to the patient and try it on their hand
to show them
it will not hurt.
Ask the patient to close their eyes or look at the ceiling and tell
you each time
they feel the monofilament touch their foot.
36. Randomly place the end of the monofilament on the 9 different
areas of the
foot (see image to the right) with enough pressure to bend the
monofilament.
If the patient does not say "yes" at a particular site, continue to
the next site
and re-test that site at the end.
Check achilles reflexes.
Question
List some of the preventive measures will you recommend to
Mr.
Morales regarding foot care.
The suggested answer is shown below.
Letter Count: 0/1000
SUBMITSUBMIT
Answer Comment
Foot Care for Patients with Diabetes
It is important to review and provide information about foot
self-care
TEACHING POINTTEACHING POINT
http://diabetes.niddk.nih.gov/dm/pubs/complications_feet
with diabetic patients.
Patients should be instructed to check the dorsal and plantar
37. surfaces of their feet everyday for cuts, sores, redness, and
swelling.
If the patient is unable to view his entire foot by himself, then a
caregiver should be asked to do it for him.
Feet should be washed daily and dried well.
Remind patients to use their forearm to check water temperature
to
prevent burns.
Patients should keep the skin of their feet smooth and soft with
lotion.
Toenails should be trimmed weekly or as needed.
Patients should be encouraged to wear white socks, as these will
show any drainage from a previously unknown sore, and well-
fitting,
comfortable shoes.
Shoes and socks should be worn at all times.
There is no robust evidence to warrant the recommendation that
all
patients with diabetes be fitted with special shoes to prevent
diabetic
foot ulcers.
High-risk patients should be referred to a podiatrist for
comprehensive foot care.
DIABETES LAB EVALUATION TESTING
" DEEP DIVEDEEP DIVE
38. The best options are indicated below. Your selections are
indicated by
the shaded boxes.
You discuss the next steps for Mr. Morales with Dr. Clay.You
discuss the next steps for Mr. Morales with Dr. Clay.
!
You tell Mr. Morales that you are finished with your exam and
explain that after
you talk with Dr. Clay, you'll both be back. You step out and
present the findings
from your physical exam to Dr. Clay. The two of you start to
discuss the next steps
for Mr. Morales.
Question
Which of the following laboratory studies are appropriate to
order for
Mr. Morales today? Select all that apply.
A. Hemoglobin A1c
B. Fasting lipid profile
C. Liver function profile
D. Basic metabolic profile
E. Spot urine albumin/creatinine ratio
SUBMITSUBMIT
39. Answer Comment
Answer Comment
> The correct answers are A, B, C, D, E> The correct answers
are A, B, C, D, E
All tests listed are appropriate because Mr. Morales has not had
these
tests in the last year. A reasonable A1c goal for a patient such
as Mr.
Morales with prevalent coronary artery disease would likely be
7-8%.
Chronic Diabetes Evaluation
Hemoglobin A1cHemoglobin A1c
Hemoglobin A1c should be ordered every six months in patients
who are meeting their individualized treatment goals, and every
three
months if they are not or if therapy is changing.
A HbA1c goal of < 7% is generally a reasonable goal for a
nonpregnant, otherwise healthy adult patient. More stringent
A1c
goals (< 6.5%) may be appropriate in some patients, with
shorter
disease duration, long life expectancy, and no significant
cardiovascular disease, if it can be attained without significant
hypoglycemia.
The ADA Standards of Medical Care in Diabetes state, "less
stringent
A1c goals (such as < 8%) may be appropriate for patients with
history
40. of severe hypoglycemia, limited life expectancy, advanced
microvascular or macrovascular complications, extensive
comorbid
conditions, and those with longstanding diabetes in whom a
stringent
goal is difficult to attain." For patients who have limited
resources and
a poor support system, and/or are unable to prioritize self-care
due to
social, economic or psychological stressors, a less stringent A1c
goal
may also be appropriate.
Remember that HbA1c levels are unreliable in patients with
hemoglobin variants, such as sickle cell disease; with end-stage
kidney
failure/on dialysis, and who have recently had blood
transfusions or
large blood loss.
Individuated Hemoglobin A1c Goals
Healthy Nonpregnant Adults, without severe recurrent
hypoglycemia/hypoglycemic unawareness
< 7%
Medically Complex Adults, with history of severe
TEACHING POINTTEACHING POINT
hypoglycemia and/or longstanding diabetes < 8%
Medically Complex Adults/Adults in Poor Health, with
41. severe recurrent hypoglycemia/hypoglycemic
unawareness
<
8.5%
Fasting lipid profileFasting lipid profile
The ADA and the AHA/ACC are overall in agreement regarding
lipid
management in diabetic patients.
The AHA/ACC guidelines are:The AHA/ACC guidelines are:
Lifestyle modification (weight loss, increased physical activity,
reduced fat intake) should be recommended for all patients with
diabetes, where appropriate.
All patients with diabetes and cardiovascular disease, regardless
of
age, should be on a high intensity statin.
All patients aged 40 to 75 with diabetes should be on a
moderate-
intensity statin. If ASCVD risk is >7.5%, they should be on a
high-
intensity statin.
For patients aged <40 or >70 with diabetes, consider statin
therapy
depending on risks/benefits and patient preferences.
The ACC/AHA does not recommend lipid goals at this point.
See the requiredrequired Aquifer Cholesterol Guidelines module
for more
42. information about this.
Liver function profileLiver function profile
Indicated if the patient takes a TZD. When patients take this
class of
medication, liver tests should be monitored periodically.
Basic metabolic profileBasic metabolic profile
Indicated to monitor renal function if the patient takes
metformin
and in patients with diabetes in general.
Spot urine albumin/creatinine ratioSpot urine
albumin/creatinine ratio
Indicated annually in patients with Type 2 diabetes without
evidence
of increased urinary albumin excretion (<30 mcg albumin/mg
creatinine) and more often to assess for progression and effect
of
DIAGNOSES
FINDINGS
NOTES
MENUMENU
https://southu-nur.meduapp.com/documents/796
https://southu-nur.meduapp.com/
https://southu-
nur.meduapp.com/document_set_document_relations/90965#
43. therapy in patients with established increased urinary albumin
excretion (30 mcg albumin/mg creatinine or greater). A
diagnosis of
increased urinary albumin excretion is made when two of three
specimens collected within a 3- to 6-month period are 30
mcg/mg
creatinine or greater. Remember that vigorous exercise within
the last
24 hours, menstruation, illness, fever, markedly elevated blood
pressure, CHF exacerbation, and acute hyperglycemia can cause
false-
positive results.
Urine dipstick measurements are not used to diagnose or follow
increased urinary albumin excretion because of the insensitivity
of the
method for detecting the initial small increases in protein
excretion.
Protein excretion must exceed 300 mcg per day to turn the
dipstick
positive.
Estimated GFR based on the serum creatinine should also be
used to
assess for chronic kidney disease, at least annually, looking at
declining GFR as another marker of kidney disease progression.
See the associated reference ranges in conventional and SI
units.
CONCLUDING THE VISIT CARE DISCUSSION
" DEEP DIVEDEEP DIVE
BOOKMARKS
44. https://www.meduapp.com/resources/laboratory_reference_valu
es
The best options are indicated below. Your selections are
indicated by
the shaded boxes.
Mr. Morales explains his frustration with quitting smoking.Mr.
Morales explains his frustration with quitting smoking.
!
You and Dr. Clay return to speak with Mr. Morales. Dr. Clay
spends time catching
up with him, clarifying some parts of the history and performing
her own physical
exam.
She then asks, "How's the smoking going?"
He responds, "I know I need to stop smoking, Dr. Clay. I've cut
down to less than
half a pack a day, but I just can't quite seem to do it."
She encourages him, "We'll help you come up with a plan for
stopping completely.
We know that you can do it!"
Dr. Clay asks Mr. Morales to get redressed and go to the lab to
have some blood
drawn. She directs him to return to the exam room when he is
finished so you can
discuss the next steps for his care together.
45. Question
Which of the following recommendations should be given to
Mr. Morales
today? Select all that apply.
A. Discontinue metformin.
B. Attempt smoking cessation (with help in putting a plan in
place).
C. Increase lisinopril to 40 mg daily, and return to the lab for a
potassium and creatinine measurement in one week.
D. See a dentist every other year.
E. Pneumococcal vaccination.
F. Influenza vaccination.
G. Return to clinic in six months.
SUBMITSUBMIT
Answer Comment
> The correct answers are A, B, C, E, F> The correct answers
are A, B, C, E, F
Smoking Cessation in the Setting of Diabetes
Complete smoking cessation is the goal in all patients, and
smoking
cessation counseling should be part of every clinic visit. Merely
asking
46. if the patient is considering smoking cessation increases the
chance
that the patient will quit. Patients who have already cut down
should
be congratulated on accomplishing that hard task, then they
should be
encouraged to build on this success and quit completely.
Studies have shown that diabetic smokers suffer far more
cardiovascular comorbidity than patients without diabetes who
smoke
and that smoking cessation leads to decreased progression of
retinopathy and nephropathy.
Vaccinations for Patients with Diabetes
Diabetic patients should receive a pneumococcal vaccination
and
should be immunized for influenza annually. They should also
receive
the Hepatitis B vaccine series if they are between 19 and 59
years old.
TEACHING POINTTEACHING POINT
TEACHING POINTTEACHING POINT
Dental Care for Patients with Diabetes
Diabetic patients should be seen by a dentist regularly; the
recommendation is twice a year.
Metformin Contraindications
Metformin is not recommended for patients with reduced
ejection
fraction requiring pharmacologic therapy, in particular patients
47. with
unstable or acute heart failure. It is likely safe in patients with
well-
compensated, stable CHF. It is prudent to stop a patient's
metformin
in the setting of a recent heart failure diagnosis but it may also
be
reasonable to restart it in the future should their symptoms
stabilize.
Metformin is also contraindicated in patients with a GFR of <
30
mL/min/1.73m . In addition, it shouldn't be started in patients
with a
GFR of 30 to 45 mL/min/1.73m though can be continued at a
reduced
dose with a GFR in this range in patients started on the
medication
when kidney function was normal. It is also contraindicated in
patients
with alcohol abuse or marked liver disease. These
contraindications
exist due to the increased risk of lactic acidosis in these
patients.
Metformin should be routinely discontinued when patients are
hospitalized due to the increased risk of dehydration and
opportunity
for IV contrast dye use, which could reduce renal function.
2
2
Increase lisinopril to 40 mg daily (C)Increase lisinopril to 40
mg daily (C): Mr. Morales' blood pressure is
above goal, so increasing his ACE inhibitor will hopefully
48. lower his blood
pressure while affording renal protection and decreasing urinary
albumin excretion. It is prudent to evaluate for hyperkalemia
and a
further increase in creatinine in one week, given that both are
known
side effects of ACE inhibitor therapy.
Mr. Morales' A1c is likely not at goal of 7% to 8%, and today
you are
discontinuing his metformin and pioglitazone. He is likely
going to need
additional hypoglycemic agents to lower his blood glucose,
perhaps
prandial insulin. Waiting six months to see him again (G) puts
him at
great risk of incurring additional co-morbidity from poorly
controlled
Type 2 diabetes. He should be seen in two to four weeks to
ensure that
TEACHING POINTTEACHING POINT
TEACHING POINTTEACHING POINT
additional agents are added in a timely manner if necessary.
See the associated reference ranges in conventional and SI
units.
MEDICATIONS TO TREAT DIABETES TEACHING
Dr. Clay uses this as an opportunity to teach you a little bit
about oral and
injectable medications that are used in the management of the
49. Type 2 diabetic
patient.
Injectable Medications for Type 2 Diabetes
InsulinInsulin
Different types of insulin are used to manage diabetes.
The ADA Standards of Medical Care in Diabetes state,
"consider initiating insulin
therapy (with or without additional agents) in patients with
newly diagnosed
Type 2 diabetes who are symptomatic and/or have A1c 10% or
greater and/or
blood glucose levels 300 mg/dL or greater."
Evidence is accumulating that earlier use of insulin in the
treatment of patients
with uncontrolled Type 2 diabetes results in better long-term
glycemic control.
In a patient with an A1c value 9% or greater, oral hypoglycemic
and non-insulin
injectable medications as monotherapy are unlikely to bring the
patient's A1c to
goal, and dual therapy is recommended.
When insulin is used, typically a basal insulin, such as glargine
or detemir, is
initiated first, with continuation of one or more oral
medications (usually
metformin, unless there is a contraindication). The regimen is
then escalated
every three to six months until the A1c goal is attained.
In patients on a single oral agent whose A1c is within one
percentage point of
50. goal, adding another oral agent or non-insulin injectable should
be considered.
A well-known meta-analysis found that for each non-insulin
agent added from a
different class, the A1c could be expected to decrease 0.9-1.1%.
For a comprehensive list of available insulins refer to table 8.2:
Pharmacology of
available glucose-lowering agents in the U.S. for the treatment
of type 2
TEACHING POINTTEACHING POINT
https://www.meduapp.com/resources/laboratory_reference_valu
es
https://medu-relier-
production.s3.amazonaws.com/files/SIMPLE-08-
c2HsB1o7coAFhzTur-
Z5A2MUkASComz6CQVw5pWjneKqY6ACxrW/compressed/im
ages/251224.jpg
http://care.diabetesjournals.org/content/41/Supplement_1/S73.fi
gures-only
diabetes
Glucagon-like peptide-1 receptor agonistsGlucagon-like
peptide-1 receptor agonists
Mechanism of action:Mechanism of action: There are several
GLP-1 receptor agonists available,
commonly prescribed agents include exenatide and liraglutide.
These agents
increase insulin secretion in a blood glucose dependent manner.
They also
decrease post prandial glucagon secretion, slow gastric
51. emptying, centrally
increase satiety, and decrease appetite. *
Administration:Administration: These agents are all delivery by
subcutaneous injection.
There are monthly, weekly, daily and twice daily formulations.
They can be used
in combination with most oral medications and with basal
insulin. *
Side effects:Side effects: The most common side effect is
nausea, which can be
significant, accompanied by emesis. *
Effects:Effects: A1c decreases of approximately 1% and
statistically significant
weight loss are associated with use.
Contraindications:Contraindications: There have been post
marketing reports of exenatide-
induced pancreatitis, so its use in patients with a history of
pancreatitis should
be avoided. Tumors of the C-cells have been reported.
References
American Diabetes Association Standards Of Medical Care In
Diabetes-2018. Diabetes Care. 2018 Jan;
41 (Supplement 1): S1-S2.
http://care.diabetesjournals.org/content/41/Supplement_1.
Accessed May
4, 2018.
American Diabetes Association Standards Of Medical Care In
Diabetes-2016. The Journal of Applied
Research and Education. January 2016, Volume 39, Supplement
1.
52. http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Su
pplement_1.DC2/2016-Standards-of-
Care.pdf.. Accessed May 4, 2018.
CONCLUDING THE VISIT CARE DISCUSSION
You and Dr. Clay return to the exam room to talk to Mr.
Morales about your
recommendations for his diabetic care.
Dr. Clay starts, "We'd like you to stop taking the metformin and
pioglitazone
because those medications are not the best or safest in patients
who have heart
failure like you do."
"But won't that make my blood sugars go up with two less
medicines everyday? I
thought we were going to get my blood sugars lower," Mr.
Morales wants to know.
http://care.diabetesjournals.org/content/41/Supplement_1/S73.fi
gures-only
http://care.diabetesjournals.org/content/41/Supplement_1
http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Su
pplement_1.DC2/2016-Standards-of-Care.pdf
"You're right, Mr. Morales. Without those two medicines, your
readings will likely
increase, so we'd like to increase your glipizide to 10 mg daily
to help. Taking
glipizide with glargine insulin every day will also help. We'd
like to have you call the
office in a few days with your readings so we can see how it's
going. We will be
working closely in the coming weeks and months to keep your
53. glucose well
controlled, and we'd like you to see a diabetes educator and a
nutritionist for help
with your food choices and portions."
You tell him that you'd like to better control his blood pressure,
and he agrees to
take the increased lisinopril dose.
"The good thing, Mr. Morales, is that getting your glucose and
blood pressure
under control will help your kidneys function better. And
stopping smoking will
help too. Have you thought about whether you are ready to quit
now? Would you
consider setting a quit date?"
He responds, "Maybe we can talk about that when I come back
the next time."
You remind him to check his blood sugar with his glucose meter
when he feels
"low" so that he doesn't eat when he doesn't need to. You
reiterate the proper
treatment of blood glucose to achieve a reading of >70 mg/dL
(>3.9 mmol/L).
You make him an appointment for a dilated eye exam and advise
him to check his
feet daily.
You are able to give him two more weeks of testing strips and
the toll-free number
to the patient assistance line for glargine insulin so that he can
request samples.
You ask him to see the clinic's social worker for further help
54. with patient
assistance and hand him a note for work explaining his need to
be allowed off the
line to check his blood sugar regularly, as well as his need to be
seen in close
follow up with Dr. Clay.
As he leaves, Mr. Morales says, "I'll see you in two weeks, and
thank you for taking
the time to really talk to me and find out how to help. I feel like
I am really going to
be able to take care of myself this time, and I'll have my
tobacco quit date when I
see you again!"
See the associated reference ranges in conventional and SI
units.
LAB RESULTS AND DIABETIC
NEPHROPATHY
MANAGEMENT
https://www.meduapp.com/resources/laboratory_reference_valu
es
It is two weeks later and Mr. Morales is back in Dr. Clay's
diabetes clinic.
You take a look at the electronic medical record, and the lab
results from Mr.
Morales' initial clinic visit reveal:
Lab Values: Conventional: SI:
55. Potassium 4.8 mEq/L 4.8 mmol/L
BUN 29 mg/dL 10.4 mmol/L
Creatinine 1.8 mg/dL 159 μmol/L
Hemoglobin A1c 8.3%
Total cholesterol 213 mg/dL 5.52 mmol/L
Triglycerides 385 mg/dL 4.35 mmol/L
HDL 38 mg/dL 0.98 mmol/L
LDL 117 mg/dL 3.03 mmol/L
Liver function panel: normal
Spot urine albumin to creatinine ratio: 120 mcg/mg creatinine
You realize that the spot urine albumin to creatinine ratio
confirms Mr. Morales'
prior history of increased urinary albumin excretion. Prior to
seeing Mr. Morales,
you decide to look up some information about diabetic
nephropathy.
You are glad that you increased Mr. Morales' lisinopril dose
during the last visit
since it will hopefully slow progression of his diabetic
nephropathy.
You highlight that his A1c is above goal, but you tell Dr. Clay
that it may not be
necessary to make adjustments to his diabetic regimen since that
was done at the
56. last visit.
See the associated reference ranges in conventional and SI
units.
Diabetic Nephropathy
TEACHING POINTTEACHING POINT
https://www.meduapp.com/resources/laboratory_reference_valu
es
Diabetic Nephropathy
EpidemiologyEpidemiology
Diabetic nephropathy occurs in 20% to 40% of diabetic patients
and is the most
common etiology of end-stage renal disease in the U.S.
Risk factors associated with the progression of diabetic
nephropathy include:
obesity, increasing age, African American race, and tobacco
abuse.
PathogenesisPathogenesis
Kidney insult appears to originate with glomerular hypertension
and
hyperfiltration. Chronic hyperglycemia leads to mesangial
expansion,
deposition of matrix, increased amount of VEG-F and other
cytokines, local
inflammation, and activation of protein kinase C.
Prevention / TreatmentPrevention / Treatment
57. Two large prospective trials (DCCT with type 1 diabetics and
UKPDS with Type 2
diabetics) revealed that intensive glucose management resulted
in prevention
or delayed onset and progression of diabetic nephropathy.
Aggressive blood pressure lowering is critical for treatment of
increased urinary
albumin excretion. In patients with hypertension with increased
urinary
albumin excretion, an ACE inhibitor or ARB therapy is
recommended to delay
the onset and decrease progression of diabetic nephropathy.
ReferralReferral
Referral to nephrology is appropriate if the the cause of kidney
disease is not
certain, and or there are challenging management issues present,
such as
resistant hypertension or electrolyte derangement. The threshold
for referral to
nephrology varies across providers; however, nephrology should
be consulted if
Stage 4 or greater chronic kidney disease (GFR < 30 ml/min per
1.73 m )
develops since this has been found to reduce cost, improve
quality of care, and
keep people off dialysis longer.
2
FOLLOW-UP VISIT CARE DISCUSSION
58. You and Dr. Clay congratulate Mr. Morales on his weight loss
before tellingYou and Dr. Clay congratulate Mr. Morales on his
weight loss before telling
him to return for a follow-up visit.him to return for a follow-up
visit.
!
You and Dr. Clay review Mr. Morales' vitals. His weight is
down two pounds and his
blood pressure is 129/72 mmHg.
Mr. Morales greets you, "You are going to love these blood
sugars! That ADA Web
site has great information and the social worker has gotten it
worked out so that I
receive patient assistance for most of my medications and
supplies. I've learned so
much from the nutritionist and diabetes educator. I've
completely changed the
way I eat and I'm taking a walk around the block every evening
before supper.
There is one thing, though. My wife does most of the grocery
shopping and she
doesn't speak English very well. Are there any resources
available in Spanish?"
"Certainly, Mr. Morales - I'll make sure that you have that
information before you
leave."
You both review Mr. Morales' blood sugar log and find that by
taking his glargine
insulin daily, his fasting readings have come into goal nicely
and his prandial
59. readings are within goal >75% of the time.
"Congratulations on all your hard work, Mr. Morales! These
readings look
wonderful and your weight and blood pressure are coming down
nicely. I don't
think I'll make any changes to your diabetes regimen today, but
keep calling every
week with your readings so that we can stay on top of your
sugar control. You
know, if you keep losing weight, you may be able to come off
the insulin."
"Thanks, Dr. Clay. I've been working hard, and I sure would
like to stop giving
myself that shot, so I'm going to keep on losing. And I've
decided to quit smoking
next Monday."
"That's great, Mr. Morales! We'll make sure that you get some
printed information,
as well as some website addresses, so you can maximize your
chances for success.
You review the remainder of Mr. Morales' labs, including his
HbA1c, renal function,
and the presence of microalbuminuria.
Dr. Clay tells Mr. Morales to return to the office in four weeks
for a follow-up visit
and reminds him to stop at the lab to check on his potassium
and kidney function
because of the higher ACE inhibitor dose.
60. "See you then, Dr. Clay. I'll be calling with my readings in a
week or two."
Diabetes Patient Resources in Spanish
The ADA website has excellent resources for Spanish-speaking
patients and
their families.
This is the final page of the case. We value your perspective on
the learning
experience. After completing three required feedback ratings
you can finish the
case and access the case summary.
CASE SUMMARY DOWNLOAD FINISH CASE
Well done! You have completed the case. Click to download the
case summary.
DOWNLOAD CASE SUMMARYDOWNLOAD CASE
SUMMARY
You may now continue to the optional self-assessment questions
for you to assess
what you have learned in this case.
RELEASE NOTES RELEASE NOTES
TEACHING POINTTEACHING POINT
http://www.diabetes.org/espanol/?utm_source=Homepage&utm_
medium=RedNav&utm_campaign=ESPANOL
LEARNING OBJECTIVES LEARNING OBJECTIVES
QUESTION 1 SAQ
61. QUESTION 2 SAQ
QUESTION 3 SAQ
QUESTION 4 SAQ
QUESTION 5 SAQ
Thank you for completing Internal Medicine 08: 55-year-old
male with
chronic disease management.
Name……………………………………………
Date………………………………………
Course: CSMT 345-Surveying and Layouts
Homework 1
Instructions:
Answer all the questions and submit your work in blackboard by
Sunday January 26, 2020 at
11:59pm. Observe the due date as any late submission will be
graded at 50% or may be rejected
by the instructor. Answers must be complete. Credit may be
given for submissions 2 days earlier.
Questions (Total = 20 points)
62. 1. Your supervisor has asked you to prepare a list of equipment
that your crew will use for
construction survey and layout for a building project.
a. List six of such equipment (3 points)
b. Pick two from the list which are PPE and state their functions
(2 points)
2. Giving example, differentiate the field engineer from office
engineer with reference to
construction surveying and layout (2 points)
3. I. What is effective communication and why is it important in
construction survey
and layout? (2 points)
II. It is an important requirement for the field engineer to
communicate effectively to
the craftspeople during surveying work at the jobsite.
63. a. What are the three words to summarize the basic principles of
marking in
construction survey (1 point)
b. Describe each of the three words with reference to surveying
and layout (2 points)
4. Using examples, differentiate the following with reference to
survey and layout
a. Errors and mistakes (2 points)
b. Accuracy and precision and stating where you would use
require both (3 points)
64. 5. Describe the requirement for a sharp tool in surveying and
layout operation (3 points)
1/13/2020
1
Communication
CSMT 345
LECTURE 2
Communication
• The basics
• Communicating with signals
• Stakes and laths
• Marking Line and Grade
• Abbreviations and Symbols
1/13/2020
65. 2
The basics
• Field engineer avenues to being successful
– Technical competence and the high level ability to perform
surveying and layout
– Ability to communicate the results of the technical tasks
performed
– Areas of communication of field engineer
• Discussing layout with the craftspeople and be able to provide
lines and grades for their needs
• Communicating with superintendents the points that have been
laid out and the plans for the future layouts
• Communicate with the owner providing an overall description
of
where parts of the project are located and how the phases of
construction will occur
• Overall: must have both technical skills and communication
skills
Success Avenues
• Field engineer must be able to:
– Interact courteously and criticize effectively
– Gather information and make proper decisions
66. – Deal with conflicts
– Hold successful meetings and solve problems
• Understanding the principles of effective communication is
key to the success of the field engineer
• Be Honest
– Accept mistakes and strive to improve; no compromise of
integrity
• Good manners
– Build good rapport with workmates; have structured work
habits
• Think, talk and act like a business person
– Take actions quickly and in a professional manner
– Treat others with dignity and respect
• Always double check for accuracy (of layouts and
communication)
1/13/2020
3
Oral Communications
• Listening well is the key to oral communication
– Effective people master the art of listening well both in
business and at jobsite
67. • Strategies of effective listening
– Remove distractions and concentrate fully
– Be understanding and patient at all times
– Show that you are actively listening
– Watch your temper and the temptation to argue
– Criticize positively
• Discussions are where effective listening manifest
– Be clear and provide enough information
Oral Communications
• Telephone communication and good habits
– Precise information must be given and heard in the same
manner
– Be prepared and make sure you know your material
– Take notes including details of the caller
– Know what satisfactory answer will be
– Monitor your feelings, voice, and language
– Use words and examples familiar to the listener
– Speak slowly so that your words are not missed
• Radio Communication
68. – Refrain from yelling on the microphone
– Hold the radio 4-6 inches away from your chin
– Use word ‘’out’ to signal end of discussion
1/13/2020
4
Written Communications
• Unclear document with incorrect words, misspellings
and unclear paragraphs can give a reader an
impression that you are not a very serious or reliable
person to deal with in construction business
• Writing an effective letter
– May be to persuade someone to agree or take an action
– Must be concise, be easy to notice important items, make
sense and contain all important information
– Attention to crowding, punctuation, repetition, and gender
– Structure it correctly following the format of introduction,
body, and conclusion
– Double check for errors; run spell check and read over
again or ask someone to look over the document for you
Meetings
69. • Preparation is key before meeting with foremen/women, rod
persons, supervisors or any other;
• Plan
– Identify the goal/reasons for the meeting and your
contributions
• Arrive well prepared
– Be punctual and prepare an up to date information for the
meeting
• Adopt good meeting habits
– Speak honestly and courteously and avoid interrupting others
– Listen carefully and avoid side conversations
– Learn from disagreements and above all…always be patient
• Actively participate
– Listen, collect feedback and make positive comments
– Deliver information in an interesting and simple manner
• Be considerate
– Maintain good eye contact, and monitor voice quality and
word choice
1/13/2020
5
Dealing with People
70. • As a field engineer, you will work with different people
– Learn to deal with different personalities
• Watch for non-verbal signals
– The way something is said is more important than what is
said, so watch your non verbal signals as well as for others
– Examples:
• Body and face movement
• Silences and tone of voice
• Eye contact (Americans vs the rest of the World)
• Learn about your audience
– Find what matters to your audience
• Make decisions
– Field engineers are leaders in construction and must
continuously make decisions
Giving and Receiving Criticism
• Criticize the behavior and not the person and try not to
criticize when angry
• Lay criticism in a positive manner and not negatively
– Instead of screaming YOU SHOULDN’T HAVE DONE THAT
consider saying ‘’this doesn’t seem to be working, lets
diversify a different view and approach’’
• Overall, control your temper when giving criticism
71. – set a pleasant tone, show understanding, offer support where
needed and above all, show confidence that the person will
improve to the required performance
• When you receive criticism
– Try to re-evaluate your views and your methods, learn from
others and avoid overly self defensive. Above all, try to grow
from criticisms
1/13/2020
6
Communication barriers
• Reasons a person will not understand or listen to you. It
is important that you overcome these barriers
– Poor listening abilities, e.g., short attention span
– Poor habits, e.g., chewing, tapping, arriving late
– Insufficient interest, e.g., overwhelming someone with
information
– Differing word definitions, e.g., same words may have
different
meanings
– Lack of basic knowledge
– Competing noise; always be in quiet zones when
communicating or
72. use hand signals where possible
– Different backgrounds and language; people from different
cultures
may have different meanings to different communication styles.
Try to
understand or be patient and accommodative when working with
people from diverse backgrounds
Communicating with signals
• Very useful when working with machines or equipment
producing high decibels (sound levels)
• Sometimes hand /arm signals are means of
communication for those who speak different
languages.
• It is the responsibility of the field engineer to learn hand and
arm signals in the construction site
• Examples;
– One-hand signals for numbers
• Hand and arm signals are effective communicating methods on
sites
– Field operation signals
• For safety reasons be able to communicate well with crane
operator
1/13/2020
7
73. Communicating with signals
Communicating with signals
1/13/2020
8
Stakes and Laths
• Stakes are first evidence that construction is
about to commence.
– Nothing is built accurately until the stakes are
located correctly and the information on the stakes
are conveyed clearly
– Field engineer communicates to the crafts through
stakes
Stakes and Laths cont..
• Principles of construction stakes
– Face stakes in the correct direction
• Every project is unique, so the field engineer should place
stakes that can be read by all personnel on the site
• For highways, center line stakes are placed so they can be
read from beginning of the project. For buildings, place
corner stakes so they can be read from the same direction
such as when the person is reading from the front of a
74. building
– Use proper stake size
• The size of the stake determines its use
• Three sizes are used by field engineer; hub, stake, and lath
1/13/2020
9
Stakes and Laths cont..
• Principles of construction stakes
– Always label them
• All lines or marks for use must be labeled clearly. Mistakes
occur because of unclear labelling of marks/lines
• Hub
– Paint their top as soon as they arrive so as to be ready for use
– 1-1/2’’ x 1-1/2’’ piece of wood in lengths of 6’’, 12’’, 18’’
– Generally used to mark a specific point such as center line
point,
control points, radius points, gutter lines, blue tops
• Stake
– ¾’’ x 1-1/2’’ piece of wood with length from 12-48’’
– Used for center lines, offset lines, slope lines and information
stakes next to hubs
75. • Lath
– ½’’ x 1-3/4’’ x 48’’. Used as guards for hubs and stakes
– Can also be used to indicate limits of clearing
Stakes and Laths cont..
• Principles of construction stakes
– Offset stakes for protection
• This prevents them from being destroyed by construction
(setting
of stakes away or ‘off’ of the point of need)
– Set stakes within tolerance (accuracy levels)
– Place solidly (not to fall due to wind force; hammer well)
– Place plumb
• Sloppy stakes (not plumb) usually indicate sloppy
measurements
– Place centered
• Should be driven so the exact point is close to the center of
the hub
and on line and distance
– Color code the flagging
• Color coding is to communicate the type of stake and type of
point
being located
76. • Red, white and blue color are used to communicate types of
points
1/13/2020
10
Stakes and Laths cont..
• Principles of construction stakes
– Color code flagging
Survey point Flagging Color(s)
1 Primary control Red/white/blue
2 Secondary control Red/white
3 Building control Red
4 Benchmark White/blue
5 Temporary benchmark white
6 Finished stake Blue
7 Slope Stake Red/blue
Stakes and Laths cont..
• Principles of communicating on stakes
– Ensure consistency on how you mark the stakes
77. – Print neatly
• Lettering style of the field book should be followed (all
uppercase lettering, slightly slanted and evenly spaced)
– Write legibly
• Avoid crowding the words and numbers
• Write from top to bottom of the stake every time
– Use understandable abbreviations
• Write full words if you can
• If abbreviations are used, discuss them with everyone
• E.g., Toe (Toe of Slope), Top (Top of Slope), P.I. (Point of
Intersection), P.C. (Point of Curvature), B.C. (Back of Curb),
T.B.M
(Top of Benchmark), B.M. (Benchmark).
1/13/2020
11
Stakes and Laths cont..
• Principles of
communicating on
stakes
– Use all sides
78. • Field engineer should use
all sides of the stake, but
primary identifying data
should be facing the
direction of use
– Typical order of
information
• Stake example
2+0
2
0
’ R
T
₵
|
|
C
u
t 5
@
1
:1
Stake Communication
79. Station number
offset
Alignment information
Centerline
Cut or fill data
Slope
Stakes and Laths cont..
• Setting stakes on the site
– Indicate information about site clearance
limit, rough grade, fine grade, slope,
gutter/curb, pipe, e.t.c.
– Cut and fill stakes
• Reference point on the stake that shows where cut or fill
starts is called a ‘’crow’s foot’’.
• Additionally, some use color-coded surveying flagging to
indicate cut or fill on stake. The importance of this practice
is to enable the project engineer to see stakes from far and
to know areas to be cut or fill. Example: red flagging is for a
cut stake, green flagging is for a fill stake. For stake on
grade, both red and green are used
• Flagging can be used to indicate how much cut or fill, e.g., 3
red strips of flagging imply a cut 3 ft from the crow’s foot, 2
stripes of green flagging imply a fill 2 ft from crow’s foot
81. • Set stakes within tolerance that includes the
vegetation that is not to be cut. Some stakes can
be put around plants/trees not to be cut
• Stakes must be visible before, during, and after
clearing/cutting
– Rough grade
• Tolerance (Horizontal: +/-0.1’; vertical: +/- 0.2’)
• Stakes will be set on offsets from the centerline at
locations determined by the contractor or plans
12+0
2
0
’ R
T
₵
|
|
C
u
t 5
@
1
:1
82. Stakes and Laths cont..
• Setting stakes on the site
– Fine grade
• Tolerance (Horizontal +/-0.1’;vertical +/- 0.01’
• May be set as offsets or as centerline where elevation
measurements will be taken off of the top of them. Cut and fill
will be noted on each stake. Intervals = 50’ or less
• Noted on the stake will be station number, elevation on top of
stake, alignment designation and cut and fill
– Slopes
• Tolerance (Horizontal +/-0.1’;vertical +/- 0.1’
• Are placed at 10’ min. because of the danger of being dug-out
• Never scale stakes from plans, but rather use calculations to
determine field locations and information written on them
• Slope stakes should have the following
– Offset distance, slope ratio, total distance to/from the offset
stake, and
station number
1/13/2020
13
Stakes and Laths cont..
83. • Setting stakes on the site
– Curb and gutter
• Tolerance (Horizontal +/-0.01’;vertical +/- 0.01’)
• Offset should be close to the centerline (<6’)
• Stakes should have the following labels
– Offset to back of curb, cut or fill to top of curb, gutter slope,
super elevation of pavement
– Pipe
• Tolerance (Horizontal +/-0.01’;vertical +/- 0.01’)
• Two kinds of pipe takes: hubs and laths.
– Hubs are used for alignment and grade while laths are for
writing information such as percent grade, offset distance,
station, type and size of pipe and cut or fill from hub to the
invert
– Pipe runs require a reference line (beginning of run and the
end)
Stakes and Laths cont..
• Setting stakes on the site
– Minor structures
• Tolerance (Horizontal +/-0.01’;vertical +/- 0.01’)
• Inlet culverts, junction boxes require reference lines with hubs
84. on either side
• Reference lines should refer to the center of the junction box,
the center of inlet
• Laths should contain;
– Station, offset distance, to the structure’s exact location,
elevation of
hub and cut or fill distance to the structure’s invert or even to
the
bottom of the structure
– Control
• Tolerance (Horizontal +/-0.01’;vertical +/- 0.01’)
• Hubs are sometimes used as control points. However, concrete
will be used as critical control points on construction sites
1/13/2020
14
Stakes and Laths cont..
Marking Line and Grade
• Stakes are the forms of communication of the field
engineer to craftpeople
• Marking standard for all can be used to avoid confusion
• Principles of marking
85. – Straight, label and plumb: make sure the labeling is clear
– Always label
• Label clearly the lines or marks used in layout
– Straight
• Lines used for reference in construction of floor should be ‘on
line’
– Level
• Horizontal lines placed on a wall to be used as reference for
elevation should be placed exactly horizontal, not sloping
– Plumb
• Vertical lines placed on a wall as a future target must be
plumb. They
should never slant to pose difficulty for future person using any
tool.
1/13/2020
15
Basic Principles of Chalking Lines
• Chalking can be very confusing if not done well
• Develop company color
– Develop a chalking scheme to avoid confusion; a standard that
is
86. known by all; i.e., color code the chalk line
• Enhance visibility
– Chalk lines should be highly visible from far
• Protect lines
– Chalk lines may become worn out from construction activities
– Spray them with clear varnish; spray several spots along the
chalk
line to preserve the line for future use if needed
Communicating the meaning of marks
– Line and grade marks are used for communicating to the
craftperson
– It is best to be clear when communicating the meaning of a
mark
– Too much information may be confusing and too few is not
good
– Experienced field engineer will know the right information to
put
– Well written stake communication are important. Example:
• OVERALL: Develop company-specific marks so everyone
on the job knows who made the marks
RIGHT WRONG
6’ above finished floor 6’ above floor (rough or finished)
87. 4’’ offset to south of ‘H’ line 4’’ off ‘H’ line (north, south, east
or west)
1/13/2020
16
Abbreviations and Symbols
– Abbreviations and
symbols are used on
stakes and in memos
– Use abbrev. to reduce
the size of writing on
stakes
– Examples
Word Abbreviation
Alignment align.
Above Mean Sea Level ABMSL
Approximate Approx.
Backsight BS
Backsight rod reading BS
Benchmark BM
88. Building Bldg.
Center line CL
Control point CP
Triangulation Tria.
Distance D
Finish Grade FG
Grade Gra.
Traverse Trav.
1/13/2020
1
Fieldwork Practices-Part 1
CSMT 345
LECTURE 3
1
Fieldwork Practices
• Safety
• Measurement Principles
89. 2
1/13/2020
2
Fieldwork Practices
3
Fieldwork Practices
4
1/13/2020
3
Fieldwork Practices
5
Safety
• Construction industry is a hazardous industry
(costing billion of dollars annually)and Safety is
often taken for granted
– Work related injuries including fatalities occur more often
• Developing a responsible attitude is key
– A field engineer is responsible for observing safe practices
90. amongst craft people on the site
• ideally everyone should be fully responsible
– Attitude is everything!
• Good, positive attitude about safety will get others more
concerned and is key to avoiding jobsite accidents
6
1/13/2020
4
Personal Protective Equipment (PPE)
• Hardhats
– Select hardhats that is adjustable, fit well, and wont interfere
with sighting through the instrument scope
• Eye protection (safety glasses with side shields )
• Hand protection (gloves)
• Fall protection
– Safety belts and harnesses at heights over 6’-especially when
surveying and marking points on high or sloping areas
• Safety vests
– Field engineers may be surveying hazardous areas (whether on
jobsites where heavy equipment is operating or next to highway
91. where cars are moving fast). They should wear highly visible
florescent safety vests at all time
– Vests with pockets to carry small surveying tools are
preferred 7
Personal Protective Equipment (PPE) cont..
• Ear protection
– Sites are usually noisy; field engineers should have some ear
protection at all times (e.g. ear muffs, plugs)
• Foot protection
– Slips, falls, and trips are common site accidents
– Select shoes that are sturdy and protect against compression,
slip and puncture.
– Boots should have ample room to avoid foot problems
– Steel toe safety shoes/boot is always preferred
– Note: When your feet hurt, you hurt all over
8
1/13/2020
5
Crew Protective Equipment
• Each crew is responsible for warning other workers and
92. public that they are working on a site and they need various
safety equipment
– Warning signs
• ‘Survey Crew ahead!’ sign can tell drivers to slow down
– Survey Cones
• Every survey vehicle has them
• Should be highly visible and reflective even in low light. The
bigger
(28’’ high) the cones, the more visible they are
– Flashers and barricades
• Used in extremely hazardous areas to prevent crew from harm
• Installation of concrete barriers around surveying control
points
usually provide the required degree of safety in hazardous areas
9
Crew Protective Equipment
10
1/13/2020
6
Crew Protective Equipment
93. 11
Crew Protective Equipment
• Dressing for the environment
– Must be concerned with more than physical hazards, e.g.,
summer heat or winter weather; skin cancer (using sun screen
in summer), drinking plenty of water; moisture control in cold
weather is key; avoid frost bites (hypothermia)
– Know the weather conditions and plan accordingly
12
1/13/2020
7
Hand tools hazards
• Crew should be trained on proper care, operation and
provided with proper safety equipment to work with in
surveying
• Common examples;
– Machete
• Make sure no one is close to you when working with it
– Chain saws
• Used for heavy clearing
94. • Wear proper PPE (hardhat, well fitting clothing, safety boots
with
protected ankles in the event of tool slip…steel toes will
prevent
injury from falling logs
• Always wear protective gear when using chain saws
• Note:
– remember that the safest cutting tool is the sharp one
13
Natural Hazards
• In addition to weather and equipment hazards, surveying in
the field may expose you to many dangers
– Plants (thorns, poisonous types)
– Wild animals (foxes, dogs)
– Snakes (poisonous snakes)
• Most poisonous snakes have triangular shaped heads.
• When beaten, be calm, identify if poisonous or not and seek
for
anti-venom treatment. Excitement makes the blood (with
venom)
speed to the heart and maybe dangerous
• Wear knee high boots or leggings for protection
– Insects
95. • Wasps, bees, spiders, scorpion
• More people die annually from bee stings than snake bites
• Proper PPE is needed, e.g., gloves, long sleeved shirts, etc.
14
1/13/2020
8
Highway hazards
• Consider man-made dangers when surveying on
public roads
• It is your responsibility as field engineer to see that
workers are in safe working conditions.
• Include signs, barriers, traffic cones, and orange vests
(florescent vests to make crews more visible to
average drivers)
• You should have a flag person in addition to signs if
need be
15
Construction hazards
16
96. 1/13/2020
9
Construction hazards
17
Construction hazards
• High voltage power lines
– Wooden rods are the safest compared to metallic rods
near powerlines
– Caution: never touch any powerline with any surveying rod
• Heavy equipment and trenches
– Proper shoring of trenches and cutting at proper angle of
repose
– Conducting survey work in trenches must be within
operator’s sight or line of view
• Falls
• Noise
• Note: it is the job of field engineer to observe good
safety practices on jobsites 18
1/13/2020
97. 10
Measurement Principles
• A field engineer must have knowledge to perform
standard surveying measurements on jobsites
• Standard surveying knowledge includes
– Measuring distances, angles, elevations; and
understanding mistakes and errors, proper notetaking and
care of equipment
• The field engineer must
– Reduce the size of errors in measurement
– Eliminate mistakes
– Understand rules/principles of measurement
19
Measurement Principles
• Total Honesty Needed
– Report what you measure, not what you have calculated
that you should measure, or what you think someone
wants to hear
– No cover-up of mistakes as they may be discovered
eventually and will cost more to correct
– Be a good communicator and listen to foremen/women
and craft people
98. – You should be able to advise everyone of the meaning of
information written on stakes or other survey marks so the
correct work is done
20
1/13/2020
11
Measurement Principles
• Mistakes vs Errors
– Errors can be managed but mistakes are bad in surveying
Mistakes (blunders):
– occur due to carelessness, lack of understanding of plans, lack
of
knowledge about measurement techniques or lack of
knowledge of measurement equipment
– Their effects are large
• Forgetting that a foot was cut when using a chain saw
• Setting an instrument a few degrees off
– Note: check and recheck your work to avoid mistakes
Errors
99. - Usually occur
– Can be because of instrument calibrations/imperfection
– Their effects are usually small
– Human error vs instrument errors
21
Measurement Principles
• Accuracy vs Precision
– In measurement, you can have accuracy without precision and
vice versa
– All measurements work must be accurate but try to achieve
precision depending on the surveying conditions, i.e., we must
work on the precision of the equipment and our measurement
to achieve the accuracy required in surveying layout
– Example:
• A building construction with accurate plans, built perfectly
with
everything straight, leveled and plumb. After completion for it
to
be discovered that it was incorrectly located on the site. In this
case, there was good precision and no accuracy
22
1/13/2020
100. 12
Measurement Principles
• Accuracy vs Precision cont..
– Accuracy
• Being able to obtain the true value with the measurements
taken,
i.e., 10 measurements taken should be close to the true value on
average.
• E,g., bull’s eye aimed but shots hit all around with some
hitting the
target
– Precision
• The closeness of the measurements to each other, i.e., all the
measurements will be nearly the same
• This closeness of the measurements does not mean accuracy
• E.g., bull’s eye aimed but all shots are at one place off the eye
– In construction layout, we want both accuracy and precision
• All shots to hit bull’s eye every time we measure (accurately
and
precise 23
1/19/2020
101. 1
Distance Measurement-Chaining
CSMT 345
LECTURE 5
1
Fieldwork Practices cont..
• Chaining equipment
• Basics of chaining
• Proper care for chains
• Chaining a distance
• Chaining a traverse
2
1/19/2020
2
Chaining Equipment
• Distance measurement can be simple with chains along a line
• But note that the process must be error free in reading
102. – Needs skills and good understanding of procedures involved
– A successful field engineer must be consistent in chaining
procedure
– Chaining and taping is sometimes used interchangeably
• Common equipment
– Field book
– Pencil-hard tipped (2h, 3h or 4h)
– Two range pole
– Hammer, two plumb bobs
– Steel tape
– Wood stakes
– Chaining pins 3
Chaining Basics
• Familiarity with the chain/tape measure used
– To avoid errors; examine chain closely before use to note
point ‘0’
• Know the difference in chains/tapes
– The metric chains vs engineering chains
• Use two people who communicate well with each other
103. – Two people communicating verbally, by signs; loudly and
clearly
– Good long term working relationships is key to success of
chaining
• Measure horizontally and maintain good alignment
• Breaking the chain
– Applied in measuring slopes for lengths shorter than full
chain length
• Apply proper tension; for precision
• Measure all distances twice; forward and back 4
1/19/2020
3
Care of Chains and Related Equipment
• Keeping the chains in reel when not in use
• Unwinding the loops/knots on chains
• Drying the chains when wet
• Cleaning off dirt and sand from the chain
• Wiping the chain with oily cloth
104. 5
Chaining a Distance
• Success at measuring distances accurately and precisely
requires
consistency in chaining procedure
• Procedure for measuring distance
– You would want the distances to be measured horizontally
– Take measurements by incorporating head chain and rare
chain
– The forward and back distances are averaged by adding them
together and diving by 2 to obtain a mean distance. A
discrepancy
ratio can be calculated for each line measured and compared to
a
standard to determine if the distance is acceptable or needs a
repeat
• Forward – back = discrepancy
Discrepancy ÷ mean = 1/x
Example:
A horizontal distance measurement using a steel chain/tape
recorded a forward
distance of 168.29’ and back distance of 168.25’. What is the
discrepancy ratio
(relative error)? (168.29-168.25)/168.27 = 1/4200
6
105. 1/19/2020
4
Chaining a Traverse
• Traverse chaining is a step to determine the location of
points
– The interior angles can also measured after chaining and thus
determine the precision of work
– Total Station (TS) distance measurement limit the use of
traverse chaining;
• Traverse chaining in used in absence of TS
– Traverse chaining starts at one point , goes around and
ends at the same point
– Always have the following
• Designated person for head chain and rear chain
• Necessary equipment for chaining
• Prepare sketches in the field book of the traverse to measure 7
Chaining Fundamentals
• Know your equipment ; its graduations/markings/scaling and
use
• Pull hard to ensure accuracy and precision
106. • Maintaining good alignment
• Chain horizontally
– Ensure horizontal distant measurement by using plumb bob.
Very sloppy
terrain may necessitate breaking chain
• Measure both ways
– Distances must be measured forward and back as a check
• Set solid points using stakes
• Protect points using laths with information describing the use
of points
• Maintain equipment by drying, cleaning, oiling regularly
• Record complete concise and properly arranged notes
• Maintain precision
– Forward and back readings to agree at 0.01 per 100 feet
measured
8
1/19/2020
5
Chaining Calculations
107. • Forward – Back = Discrepancy
Discrepancy/mean = 1/x
• Example
A traverse chaining field notes had the following data;
Forward distance =146.80’
Back distance = 146.84’
Calculate the mean distance (ft) , the discrepancy and the
relative error
9
Errors in Chaining
• Sources of errors
– Instrument error
• Resulting from manufacturer’s defect; Calibrating can reduce
it
– Natural error
• Effects of temperature, wind and weight of the tape
– Personal error
• Carelessness in reading the tape or in manipulating the
equipment
• Types of errors
108. – Systematic
• Occur over and over again and are predictable; can be
eliminated
• Every time a distance is measured 1’ is added to attain correct
distance
– Random
• Occur due to human limitations such as in reading; always
exist 10
1/13/2020
1
Fieldwork Practices-Part 2
CSMT 345
LECTURE 4
1
Fieldwork Practices cont..
• Tolerance for construction layout
• Notekeeping
• Instrument care
• Use and care of hand tools
109. • Leveling an instrument
• Instrument set up
2
1/13/2020
2
Tolerance for Construction Layout
• Tolerance is how far off from the design location something
can be built and still be accepted by the owner
• Tolerance controls the quality of work being performed
• Tight/small tolerance is better than large ones (precision)
• Always measure to one-half of what is coming behind you
• Tolerance vary from 0 to a foot
• Every project has designs with specific tolerance levels
3
Field Note-keeping Practices
• Basic Practices
– You must leave your work on the ground for others to
build or for reference purposes or defense (in courts)
110. – Record data exactly (honestly)..no undue erasings
– Keep field book safely
– Leave no room for interpretation
– Cite/make references (i.e., if copied from another
source)
– Use a hard pencil
4
1/13/2020
3
Field Note-keeping Practices cont..
• Layout of field book
– Title page
• Company’s name, address, telephone number, name of field
engineer and any other identifying information
– Table of content
• Following chronologically
– Legend
• Used symbols and abbreviations
111. – North arrow
• Useful for orientation of the layout
– Identification information
• Numbering each page/ or name of people performing work
– Provide date, time and weather data
– Use sketches freely 5
Field Note-keeping Practices cont...
• Guidelines
– Don’t crowd the data
– Do not erase
• Erased data will be thrown out in court; just cross
– Record everything
• Do it or record it if in doubt
• Leave nothing for interpretation
• Record in field book in away that anyone with little
knowledge in
surveying will understand
– Establish standard note forms; familiar to the company/crews
– Use standard lettering techniques
112. • All capital (upper case)letters be used for clarity and
consistency
• Hard pencil (2h/3h or 4h) be used
6
1/13/2020
4
General Instrument Care
• Surveying Instrument
– Levels, transits, theodolites, EDMs and total stations are
surveying
instruments which are used to measure angles, distances or
elevations.
• Although basic parts are the same, each has telescope lenses,
clamp,
leveling screws, delicate parts that must be cared for
– A surveying instrument will only work well if in good
working
condition, properly calibrated
• Must be used according to procedures recommended by
manufacturer
– Three areas instruments can get exposed to hazards
• Transportation
– Carry in protective case and avoid bouncing it
113. • Use
– Use according to manufacturers recommendations
• Storage
– Keep in case when not in use 7
General Instrument Care
• Care and use
– Attach instrument snugly to the tripod
– Grasp the instrument firmly
– Do not touch the lenses (only with clean hands)
– Try to keep the equipment dry
– Never leave the instrument unattended
– Establish a wide foundation
– Never force the instrument
– Return the instrument to its case
8
1/13/2020
5
Tripods
• Tripods provide a solid foundation for instrument setups
114. • Should always be well kept and cared for
• Two types
– Fixed leg-cannot be lengthened/shortened to assist in set of
instrument
– Adjustable legs: is flexible for setting instrument
• Tripod has a head for attaching the instrument, wooden or
metallic points with foot pads to help force the legs into the
ground
• Always ensure a solid set up, check all screws and bolts
• Do not mishandle the equipment
• Transport it carefully, not with other equipment that can
affect it
9
10
1/13/2020
6
11
Use and care of hand tools
• Plumb bob
115. – Used to create vertical line or a point for reference
– Keep it clean and never use it as a hammer or a scribe
• Sight level
– Used in taping to keep the tape horizontal; and in leveling to
keep
from setting the leveling instrument above or below the level
rod
– Wipe the lens with clean cloth and store in protective case
• Gammon reels; for storing plumb bob strings
– Keep strings clean and check for wear
• Chaining pins; for marking intermediate points on taping
– Clean pins regularly and repaint when paint fade for visibility
• Range poles
– for making points in surveying job more visible
– Store in protective case when not in use
12
1/13/2020
7
Use and care of hand tools cont..
• Prism poles
116. – Used with electronic instruments to measure distances and
make points
visible
– Are similar to range poles, except that they have hollow tube
to allow
graduated rods to telescope in and out allowing the rod person
to
establish the height of the prism quickly
– Keep the telescoping rod clean and store the prism pole in a
case
• Brush clearing equipment (axe, machete and chain saw)
– Wear appropriate PPE when in use
– Store in protective cases
• Hammers/chisels/chains/tapes
• Level rods
– Probably the most abused survey equipment after tripods
– Avoid touching the measurement face, don’t abuse and keep
clean
• Hand held computers
13
Use and care of hand tools cont..
• General guidelines
117. – Only use those equipment you know how to use
– Keep clean
– Store in protective cases
– Keep dry at all times
– Do not force if difficult to move
14
1/13/2020
8
Leveling an Instrument
• Ability to set up an instrument depends on
availability to level it
• Remember the principle of straight, level and plumb?
• GENERAL PRINCIPLES
– Instruments are differentiated into:
• One level vials, two level vials, three/four level vials
– Use the leveling screws to raise or lower the ends of the
vial until the level bubble is centered
15
Leveling an Instrument
118. 16
1/13/2020
9
Leveling an Instrument cont..
• GENERAL PRINCIPLES
– The head of the tripod should be horizontal
• a tripod that is not horizontal requires more movement of
the leveling screws which takes more time to complete the
leveling process. Adjust the tripod legs to ensure accuracy
– Level vial positioning
• Position the level vial over the leveling screws properly so
that the
manipulation of the leveling screws is effective
– Left thumb rule
• Most people use random method of leveling which takes
longer time.
• The rule is: both thumbs in, both thumbs out, the bubble
follows the left thumb
– As a check, always rotate 180 degrees
– Turn leveling screws equally 17
119. Instrument Setup
• This is a fundamental requirement of surveying
• Three types of equipment are used
– Plumb bob
• Works well except that it can be moved easily by wind thereby
introducing errors in the set-up over a point
– Optical plummet (optical plumb line)
• Has lenses and prism for quick set up
• Was introduced to reduce errors of plumb bob; wind does not
affect it
but it can get out of calibration and needs frequent check-up
– Laser plummets
• Lasers can be placed inside an instrument and be used for
instrument
setups over a point
• They are becoming part of the instruments and are expected to
become standard feature of instruments in future
– NOTE: Tool used to setup over a point should be quick and
precise18
1/13/2020
1
120. Construction Surveying
CSMT 345
LECTURE 1
Getting started and organized in surveying
• Becoming a construction surveyor (field engineer in
construction)
– Carpenter, college graduates, surveying firms
• Planning
– Most ideal in any construction venture
• Might require spending a lot of time on it to avoid future
problems
– Is done to avoid conflicts
– Success as a field engineer is highly dependent in your
planning ability
– Plan to plan and remember: your plan is dependent on plan of
others
– Plan on relevant equipment to use
• Field book
• Pencil/chalk/marking pen
• Plumb bob/ hammer
• Tape measure/calculator
121. • PPE (Safety belt and harness, safety vest, hard hat, e.t.c.)
1/13/2020
2
Getting started and organized in surveying
Dress appropriately
for the job
Getting started and organized for surveying
1/13/2020
3
Getting started and Organized cont..
• Equipment checklist
– Field engineer must evaluate and have good understanding of
the available surveying equipment needed at specific work
points
– Manufacturer’s sheets provide various specifications of the
available equipment
– Field engineer sources of information include various trade
magazines which annually publish items such as
122. • GPS units
• Levels
• Theodolites
• Total stations
Getting started and organized cont..
• Daily Scheduling
– Time management is the most difficult task for a field
engineer
– Take control of your time with proper planning
– Daily schedules will be used to communicate the plan to
others thus making your work easier and overally enjoyable
– Can take the form of simple bar charts with sequence of
activities
1/13/2020
4
Field engineering responsibilities
• Field engineering position introduces you to different
activities on a jobsite that will develop your understanding
of the construction process and company management
systems