

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Ddd rem rai2
Semelhante a Ddd rem rai2 (20)
Mais de Rem Kulung
Ddd rem rai2
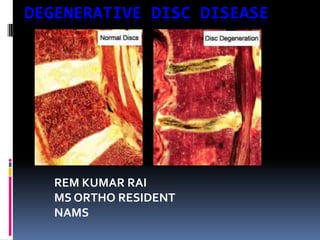
- 1. DEGENERATIVE DISC DISEASE REM KUMAR RAI MS ORTHO RESIDENT NAMS
- 2. DEFINITION Degenerative disc disease (DDD) has been used to describe a wide variety of morphologic and radiographic changes in the adult spine
- 3. DEFINITION: DISC DEGENERATION The North American Spine Society Consensus Committee on Nomenclature : Changes in a disc characterized by desiccation, fibrosis, or cleft formation in the nucleus; fissuring or mucinous degeneration of the annulus; defects and sclerosis of the endplates; and/or osteophytes at the vertebral apophysis.
- 4. DEFINITION: DDD Degenerative disc disease: as a clinical syndrome characterized by manifestations of disc degeneration and symptoms thought to be related to those changes
- 5. Intervertebral disc Total 23 Hydrostatic, load bearing , shock absorbing structure between the vertebral bodies Each disc unit has strong outer ring of fibers called the annulus fibrosus a soft , jelly like center called the nucleus pulposus 2 endplates (Campbell)
- 6. Intervertebral Disc Annulus Fibrosus Outer portion of the disc Annulus Fibrosus – Made up of lamellae fibrocartilage – Layers of collagen fibers Type I Arranged obliquely 30° Some radial fibers Thicker anteriorly >posteriolry Attached to end plates Great tensile, torsional & radial strength Lamellae
- 7. Intervertebral Disc Nucleus Pulposus – Inner structure – Notochord remnant – Type II collagen +Gelatinous GAG,H2O – High water content (7090%) – Resists axial forces Nucleus Pulposus
- 8. Vertebral End-Plate Cartilaginous & osseous component Nutritional support for the nucleus Passive diffusion
- 9. The intervertebral disc in the adult is avascular. blood vessels in the annulus until the age of 20 years and within the cartilage endplates until the age of 7 years. The cells within the disc are sustained by diffusion of nutrients into the disc through the porous central concavity of the vertebral endplate The discs vary in size and shape with their position in the spine. Discs also decrease in volume, resulting in a 16% to 21% loss in disc height after 6 hours of standing or sitting.
- 10. Anatomical Segment Components: Vertebral body Attached posterior elements Disc below Exiting and traversing Nerve root
- 11. Anatomical House with windows Window of opportunity to the disc space, interlaminar and intertransverse window
- 12. Spine Motion Segment The FUNCTIONAL UNIT of the spine Comprises of: 1.Two adjacent vertebrae 2.Intervertebral disc 3.Connecting ligaments: including the ligamentum flavum, interspinous, supraspinous, intertransverse ligament 4.Two facet joints and capsules
- 13. Natural History of Disc Disease Kirkaldy-Willis divided DDD into three separate stages with relatively distinct findings. There is recurrent episodes of pain followed by periods of significant or complete relief Dysfunction seen in those 15 to 45 years of age, characterized by circumferential and radial (micro )tears in the disc annulus and localized synovitis of the facet joints.
- 14. Instability found in 35- to 70-year-old patients, characterized by internal disruption of the disc, progressive disc resorption, degeneration of the facet joints with capsular laxity, subluxation, and joint erosion Stabilization present in patients older than 60 years, the progressive development of hypertrophic bone about the disc and facet joints leads to segmental stiffening or frank ankylosis
- 15. Each spinal segment degenerates at a different rate As one level is in the dysfunction stage, another may be entering the stabilization stage Disc herniationcomplication of disc degeneration in the dysfunction and instability stages Spinal stenosis from degenerative arthritis complication of bony overgrowth compromising neural tissue in the late instability and early stabilization stages
- 16. Pathoanatomy & pathogenesis Kirkaldy-Willis Three DYSFUNCTION phases of Degenerative process INSTABILITY STABILIZATION
- 17. Mechanism of DYSFUNCTION Episode of rotational or compressive trauma ( uncoordinated muscle contraction) Posterior joint strain ( also annular strain) Splinting Posterior joint Subluxation maintained Minor facet subluxation Synovitis( pain) Sustained segmental Hypertonicity of muscle Ischemia ( pain) Altered muscle metabolism
- 18. Symptom sign & radiological changes in dysfunction Symptom: Low back pain Often localised axial Sometimes referred /radicular Movement painful Sign: Local tenderness Muscle contracted: PSM spasm Hypomobility Extension painful Neurologically usually normal Radiograph: Loss of physiological curvatures Spinous process malalignment Irregular facet Early disc changes
- 19. Mechanism of unstable phase Severe dysfunction Continuing stress Trauma Increased dysfunction disc facets Degeneration of cartilage Coalescence of tears Loss of nucleus, internal disruption Attenuation of capsule Bulging of annulus Laxity of capsule Increased abnormal movement Unstable phase
- 20. INSTABILITY Symptom: Those of dysfunction Giving away of back, “catch” in back( on movement) Pain on coming to standing position after flexion Sign: Detection of abnormal movement( LOOK/FEEL) Observation of “catch” sway or shift when coming erect after flexion Radiograph: AP: Lateral shift Rotation Abnormal tilt Malaligned spinous process OBLIQUE: Opening facets LATERAL: Spondylolisthesis( in flexion) Retrolisthesis ( in extension) Narrowing foramen( in extension).Abnormal opening of disc Abrupt change in pedicle height.Traction spurs
- 21. Mechanism of stabilization Disc Facets Destruction of cartilage Loss of nucleus Fibrosis in joints Approximation of bodies Enlargement of facets Destruction of plates Locking facets Fibrosis in disc osteophytes Fibrosis arund joints Increased stiffness stabilization
- 22. STABILIZATION Symptom: Low back pain of decreasing severity Sign: Muscle tenderness Stiffness Reduced movement Scoliosis Radiograph: Enlarged facet Loss of disc height Osteophytes Small foramen Reduced movement Scoliosis
- 23. Diagnostic Studies ROENTGENOGRAPHY 1. AP and Lateral 2. Oblique views: useful in defining spondylolisthesis and spondylolysis 3. Lateral flexion and extension: X-ray may reveal segmental instability 4. Ferguson view (20-degree caudocephalic anteroposterior ): value in the diagnosis of the "far out syndrome," that is, L5 compression produced by a large transverse process of the fifth lumbar vertebra against the ala of the sacrum
- 24. MYELOGRAPHY Indicated if MRI is not available or for patient in whom MRI is contraindicated( cardiac pacemaker or brain aneurysm clip) valuable in a previously operated spine and in patients with marked bony degenerative change that may be underestimated on MRI improved by the use of postmyelography CT scanning
- 25. COMPUTED TOMOGRAPHY extremely useful diagnostic tool noninvasive, painless, outpatient procedure can supply more information about spinal disease Unfortunately, CT does not demonstrate intraspinal tumors or arachnoiditis and is unable to differentiate scar from recurrent disc herniation.
- 26. MAGNETIC RESONANCE IMAGING newest technological advance in spinal imaging The advantages : ability to demonstrate intraspinal tumors, examine the entire spine, and identify degenerative discs based on decreased H2O content costly and requires specially constructed facilities.
- 27. Modic Change Type I Signal intensity on low T1-weighted High T2-weighted replacement of the end-plate marrow with vascular fibrous tissue in response to chronic “injury.” Clinical: annular tear, fissure
- 28. MODIC CHANGE Type II signal intensity high T1-weighted and on FSE T2-weighted Low T2 represents replacement of the end-plate marrow with fatty tissue. Chronic marrow disuse Type II changes tend to remain stable with time.
- 29. Modic Change Type III signal intensity lowT1-weighted lowT2-weighted severely degenerated end plates only end plate change visible on CT scans or radiographssclerosis Part of the normal aging process and must not be confused with other pathologic processes, such as tumor and infection
- 30. Other diagnostic tests PET / SPECT- experimental & few centers have this facilities Electromyography/ NCVadvantage of electromyography is in the identification of peripheral neuropathy and diffuse neurological involvement indicative of higher or lower lesions. The SSEP is an extremely sensitive monitoring technique.
- 31. Bone scans positive findings usually are not indicative of intervertebral disc disease, but they can confirm neoplastic, traumatic, and arthritic problems in the spine. complete blood count, differential white cell count, biochemical profile, urinalysis, and sedimentation rate good screening procedures Rheumatoid screening studies such as rheumatoid arthritis latex, antinuclear antibody, lupus erythematosus cell preparation, and HLA-B27 also are useful when indicated by the clinical picture.
- 32. ZYGAPOPHYSEAL (FACET) JOINT INJECTIONS Cause of facet joint pain: Meniscoid entrapment and extrapment, synovial impingement, chondromalacia facetae, capsular and synovial inflammation, and mechanical injury to the joint capsule. Osteoarthritis No noninvasive pathognomonic findings distinguish facet joint–mediated pain from other sources of spine pain. Fluoroscopically guided facet joint injections therefore are commonly considered the gold standard for isolating or excluding the facet joint as a source of spine or extremity pain.
- 33. DISCOGRAPHY provocative testing for concordant pain to provide information regarding the clinical significance of the disc abnormality. Indications :surgical planning of spinal fusion, testing of the structural integrity of an adjacent disc to a known abnormality such as spondylolisthesis or fusion, identifying a painful disc among multiple degenerative discs, ruling out secondary internal disc disruption or suspected lateral or recurrent disc herniation, and determining the primary symptom-producing level when chemonucleolysis is being considered.
- 34. Lumbar spine in an oblique position with superior articular process (arrow) dividing disc space (d) in half Disc entry point is just anterior (arrow) to base of superior articular process (s) and just above superior endplate of vertebral body Curved procedure needle (c) passing through straight introducer needle (n
- 35. Lumbar Disc Disease Symptomatic LDH occurs during the lifetime of approx. 2% of the general population Factors associated with LDH: Male gender Age 30 -50 yrs Job requiring heavy lifting Lifting in a twisted or asymmetric posture Stressful occupation Lower income Cigarette smoking Exposure to prolonged vibration in the range of 4 to 5 Hz
- 36. Degenerative Disc Disease Pathophysiology: 1. Disc gradually dries out, loses height and volume. 2. NP changes from a turgid gelatinous bulb to brownish dessicated structure. 3. 4. 5. 6. 7. 8. 9. AF develops fissures parrallel to the vertebral end plates. Compressive loads transfer away from nucleus to margins Sclerosis of endplate reduces disc nutrition. Facet joints wear away cartilage, begin to override Motion segment becomes hypermobile Osteophytes develop to attempt to stabilize motion segment Osteophytes may encroach on neural structures.
- 37. Prolapse intervertebral disc Pathophysiology: 1. Acute disc prolapse is due to flexion +compression. 2. More at L4/5,L5/S1 (stress is more severe). 3. Disc rupture = stress + disturbances in the hydrophilic properties of the NP. 4. Disc rupture = fibrocartilaginous material extruded posteriorly and annulus bulges to one side. 5. Part of the nucleus may sequestrated freely. 6. Large central rupture may cause pressure of the cauda equina.
- 38. Boos et al. decrease in nutritional transport water content absolute number of viable cells proteoglycans pH increase in an increase keratin sulfate to chondroitin sulfate ratio lactate degradative enzyme activity
- 39. Pathophysiology: Pain= arises due to disruption of outermost layer of the annulus fibrosus, stretching or tearing of the posterior longitudanal ligament and pressure on the dura. symptoms worsened by coughing, valsalva, sneezing Sciatica= if disc protudes to oneside it may irritate the dural covering of the adjacent nerve root causing pain in the buttock, posterior thigh and calf. Pressure on the nerve root itself causes paraesthesia and/or numbness in the corresponding dermatome, as well as weakness and decreased reflexes in the muscles suppllied by that nerve root.
- 40. STAGES OF DDD Dessication Loss of fluid in nucleus pulposus. Disc bulge:- diffuse symmetrical outpouching of the annulus fibrosus caused by early disc degeneration& collapse Protrusion:- base wider than any diameter of the material displaced beyond disc space Extrusion:- displaced portion has a greater diameter than its connection with the parent disc at its base Sequestration:- when disc extrusion has lost all connection with the parent disc Migration:- an extruded disc, whether sequestrated or not, that has been displaced above or below the edge of the disc space
- 41. CLASSIFICATION DD Depending upon whether the displaced portion is completely enveloped by intact outer annulus or combination of annulus and PLL( s/t called capsule): Contained: Un contained: Subligamentous:- disc material contained beneath the PLL Transligamentous Submembranous:- disc material contained only by peridural menbrane
- 42. CLASSIFICATION Depending upon the relationship of the herniated material to the posterior annulus and PLL: Central( midline):- herniation along the posterior annulus Posterolateral:- along the weaker lateral expansion of PLL Foraminal( lateral ) Extraforaminal ( far lateral) In relation to nerve root: Shoulder herniation Axillary herniation According to the level of LDH: High LDH:- L1-L2, L2-L3, L3-L4 Low LDH:- L4-L5, L5-S1
- 43. SIGNS AND SYMPTOMS LDD Age:- 3rd or 4th decade in healthy adult Mostly relate to traumatic incident but Intermittent back pain of months or year Back or leg pain, radiating Aggravating :-heavy exertion, repetitive bending, twisting, or heavy lifting, relieved with rest in semi-Fowler position weakness and paresthesias, localized to the neurological level of involvement
- 44. Clinical examination Standing pt who declines to sit, with loss of normal lumbar lordosis & PVM spasm suggestive of PIVD List Limited spine ROM Point tenderness may be present over the spinous process at the level of the disc involved Atrophy of muscles – chronic cases
- 45. LSR testing During SLR maneuver , the L5 and S1 nerve root either moves or passively deforms approx. 2 to 6 mm at the level of foramen Maximum tension is realized in the sciatic nerve at 30* to 70* of elevation from the supine Crossed SLR is more specific of a disc herniation( pathognomonic of micromotion in affected side nerve roots while raising normal side leg) Large cenrtal or lateral recess herniation Free disc fragment Lasegue sign Bowstring sign
- 49. Management Goal: Prompt return to normal function and pain relief through the efficient and effective use of diagnostic tests and efficacious treatments Non operative: Reassurance, medications, and activity modification Bed rest in a semi Fowlers position for 1 to 2 days in acute cases Aerobic conditioning including abdominal and back strengthening exercises Application of heat, ice, TENS, USG massage, Traction Manipulative therapy Back school programme
- 50. EPIDURAL STEROIDS:- offer relatively prolonged pain relief without excessive narcotic intake if conservative care is elected. Methylprednisolone is the usual steroid injected. The dosage may vary from 80 to 120 mg. The anesthetics used may include lidocaine, bupivacaine, or procaine. current protocol is to inject the patient three times. These injections are made at 7- to 10-day intervals.
- 51. Indication of surgery Emergent/ absolute: Presence of cauda equina syndrome Progressive neurologic deficit Relative: Persistent radiculopathy despite an adequate trial of non surgical treatment( min of 6 wks) Recurrent episodes of incapacitating sciatica Significant motor deficit with persistent tension signs and pain Pseudoclaudication( activity related leg pain) caused by canal stenosis resulting from a disc herniation Goal of surgery: Alleviate the neural compression without further injury to the affected nerve root Minimal disruption of surrounding normal tissues and maintenance of spinal stability
- 52. Waddell’s Non-organic sign (DOReST) Finding Description 1. Tenderness a. superficial - pain with light touch to skin b. deep - nonanatomic widespread deep pain 2. Simulation a. pain with light axial compression on skull b. pain with light twisting of pelvis 3. Distraction No pain with distracted SLR 4. Regional a.nonanatomic or inconsistent motor findings during entire exam b. nonanatomic or inconsistent sensory findings during entire exam 5. Overreaction Overreaction noted at any time during exam
- 53. Surgical procedure Standard open lumbar disectomy Microlumbar disc excision Endoscopic disc excision Additional exposure Hemilaminectomy usually is required when identifying the root is a problem. This may occur with a conjoined root. Total laminectomy usually is reserved for patients with spinal stenoses that are central in nature, which occurs typically in cauda equina syndrome. Facetectomy usually is reserved for foraminal stenosis or severe lateral recess stenosis.
- 54. Thank you
Notas do Editor
- (C2-3 to L5- S1)
- degeneration involves: 1) declining disc nutrition, 2) loss of proteoglycan organization and concentration, 3) decrease in water content, 4) a decline in cell numerical density and synthetic activity, 5) increased degradative enzyme activity relative to matrix synthesis. An increased keratin sulfate to chondroitin sulfate ratio annulus fibrosis outer structure that encases the nucleus pulposuscomposed of type I collagen that is obliquely oriented, water, and proteoglycanscharacterized by high tensile strength and its ability to prevent intervertebral distractionremains flexible enough to allow for motionhigh collagen / low proteoglycan ratio (low % dry weight of proteoglycans) fibroblast-like cells responsible for producing type I collagen and proteoglycans
- nucleus pulposus central portion of the intervertebral disc that is surrounded by the annulus fibrosiscomposed of type II collagen, water, and proteoglycansapproximately 88% waterhydrophilic matrix is responsible for height of the intervertebral disccharacterized by compressibility a hydrated gel due to high polysacharide content and high water content (88%) proteoglycans interact with water and resist compressionviscoelastic matrix distributes the forces smoothly to the annulus and the end plates low collagen / high proteoglycan ratio (high % dry weight of proteoglycans) chondrocyte-like cells responsible for producing type II collagen and proteoglycanssurvive in hypoxic conditions
- With aging of the intervertebral disc there is an increase in the keratin sulfate to chondroitin sulfate ratioAt birth, the disc surface area is 50% nucleus pulposus (NP) and 50% annulus. The notochordal cells of the NP are gradually replaced by chondrocytes throughout the early teenage years. The demarcation betweenthe annulus and the nucleus becomes less distinct. The older NP has a higher collagen content with more structured fibers. In these fibers, the ratio of type II to type I collagen increases
- Stresses annulus fibrosushighest tensile stressesnucleus pulposushighest compressive stressintradiscal pressure is position dependent pressure is lowest when lying supinepressure is intermediate when standingpressure is highest when sitting and flexed forward with weights in the handswhen carrying weight, the closer the object is to the body the lower the pressure
- Epidemiology 95% involve L4/5 or L5/S1 levels L5/S1 most common levelpeak incidence is 4th and 5th decadesonly ~5% become symptomatic3:1 male:female ratio
- Disc Herniation herniated disks are associated with a spontaneous increase in the production of osteoprotegrin (OPG)interleukin-1 betareceptor activator of nuclear factor-kBligand (RANKL)parathyroid hormone (PTH)Disc aging leads to an overall loss of water content and conversion to fibrocartilage. Specifically there is a decrease in nutritional transport water contentabsolute number of viable cellsproteoglycanspHincrease inan increase keratin sulfate to chondroitin sulfate ratio lactatedegradative enzyme activityno change inabsolute quantity of collagen
- Containedbulge:circumferential symmetric disc extension upto the vertebral border within the annulus fibrosusContained protrusion: focal or asymmetrical extension of disc beyond the vertebral borderContained extrusion: extruded thru annulus but not thru PLLUncontained sequestration: disc material thru both annulus and PLL , not continuous with the parent disc materialMigration: Disc material displaced from the site of extrusion (either sequestrated or not)
- motor exam ankle dorsiflexion (L4 or L5) test by having patient walk on heelsEHL weakness (L5) manual testinghip abduction weakness (L5)have patient lie on side on exam table and abduct leg against resistanceankle plantar flexion (S1) have patient do 10 single leg toes stands
- Presence of 3 out of 5 of these sign correlated poor outcome with surgery even in the presence of true structural abnormalities.Waddell et al described and standardized these non-organic signs of low-back pain in 350 North American and British patients. They divided them into 5 categories (tenderness tests, simulation tests, distraction tests, regional disturbances, and overreaction), and found that when three or more categories were positive, the finding was considered clinically significant. This was also correlated with high scores for depression, hysteria and hypochondriasis on the Minnesota Multiphasic Personality Inventory (MMPI)