❤️Amritsar Escorts Service☎️9815674956☎️ Call Girl service in Amritsar☎️ Amri...
Cardio 2
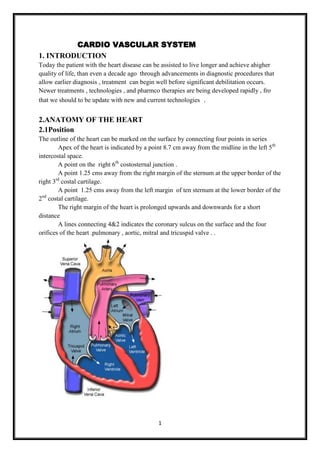
1. CARDIO VASCULAR SYSTEM
1. INTRODUCTION
Today the patient with the heart disease can be assisted to live longer and achieve ahigher
quality of life, than even a decade ago through advancements in diagnostic procedures that
allow earlier diagnosis , treatment can begin well before significant debilitation occurs.
Newer treatments , technologies , and pharmco therapies are being developed rapidly , fro
that we should to be update with new and current technologies .
2.ANATOMY OF THE HEART
2.1Position
The outline of the heart can be marked on the surface by connecting four points in series
Apex of the heart is indicated by a point 8.7 cm away from the midline in the left 5th
intercostal space.
A point on the right 6th costosternal junction .
A point 1.25 cms away from the right margin of the sternum at the upper border of the
rd
right 3 costal cartilage.
A point 1.25 cms away from the left margin of ten sternum at the lower border of the
nd
2 costal cartilage.
The right margin of the heart is prolonged upwards and downwards for a short
distance
A lines connecting 4&2 indicates the coronary sulcus on the surface and the four
orifices of the heart .pulmonary , aortic, mitral and tricuspid valve . .
1
2. The heart is composed of three layers .
The inner layer or endocardium ,consists of endothelial tissue and lines the inside of the
heart and valves.
The middle layer or myocardium is made of muscle fibers and is responsible for the
pumping action .
The exterior layer of the heart is called the epicardium The heart is encased in a thin
,fibrous muscle called the pericardium which is composed of two layers . Adhering to
the epicardium is the visceral pericardium .enveloping the visceral pericardium is the
parietal pericardium .,a tough fibrous tissue that attaches to the great vessels ,diaphragm
, sternum ,and vertebral column and supports the heart in the mediastinum
The space between these two layers (pericardial space) is filled with about 30 ml of fluid
which lubricates the surface of the heart and reduce friction during systole .
2.2 Heart chambers
The four chamber of the heart constitute the right and left sided pumping systems . the
right side of the heart ,made up of the right atrium and right ventricle , distributes venous
blood to the lung via pulmonary for oxygenation . the right atrium receives blood returning
from the superior vena cava ,inferior vena cava and coronary sinus . ..the left side of the heart
composed of left atrium and left ventricle ,distributes oxygenated blood to the aorta . the left
atrium receives oxygenated blood from the pulmonary circulation via the pulmonary veins .
The atria are thin walled because blood returning to these chambers generates low
pressure . in contrast , the ventricular walls are thicker because they generate greater pressure
during systole . the right ventricle contracts against low pulmonary vascular pressure and has
thinner walls than the left ventricle .
Because the heart lies in a rotated position within the chest cavity , the right ventricle
lies anteriorly and the left ventricle is situated posteriorly .the let ventricle si responsible for
the apex beat or the point of maximum impulse PMI,which is normally palpable in the left
mid clavicular line of the chest wall at the 5th intercostals space.
2.3Heart valves
The four valves in the heart permit blood to flow only in one direction . the valves are
composed of thin leaflets of fibrous tissue , open and close in response to the movement of
blood and pressure chambers within the chambers . there are two types of valves
Atrioventricular &Semilunar valves
2.4Atrioventricular valves
The valves separate the atria from the ventricle are termed as Atrioventricular valves .the
tricuspid valve has three cusps or leaflets , separates the right atria from the right ventricle .
the mitral or bicuspid valve has two cusps this lies between the left atria and the left ventricle
Normally when the ventricles contract , ventricle posture rises , closing the atrio ventricular
valve leaf lets. Two additionally structures , the papillary muscle and chordate tendinae
maintain valve closure . the papillary muscles located on the sides of the ventricular walls
are connected to the valve leaf lets by thin fibrous bands called chordate tendinae .
During systole contractioin of the papillary muscles causes the chordate tendinae to be come
taut , keeping the valve leaflets approximated and closed.
2
3. 2.5Semilunar valve
The two semilunar valves are composed of three half –moon –like leaflets . the valve
between the right ventricle and the pulmonary artery is called the pulmoinc valve . the valve
between the left ventricle and the aorta is called the aortic valve .
2.6Coronary arteries
The left and right coronary arteries and their branches supply arterial blood to the
heart . these arteries originate from the aorta just above the aortic valve leaflets . the heart has
large metabolic requirements , extracting approximately 70to 80% of the oxygen delivered.
The left coronary arteries has three branches . the artery from the point of origin to the first
major branch is called the left main coronary artery . two bifurcations arise off the left main
coronary artery these are the left anterior descending artery , which courses down the
anterior wall of the heart and the circumflex artery , which circles around to the lateral left
wall of the heart
3
4. The right side of the heart is supplied by the right coronary artery ., which progress
around to the bottom or the inferior wall of the heart . the posterior wall of the heart receives
its blood supply by an additional branch from the right coronary artery called the posterior
descending artery .
Superficial to the coronary arteries are the coronary veins . venous blood from these
veins returns to the heart primarily through the coronary sinus which is located posteriorly
in the right atrium .
2.7Cardiac muscle
The myocardium is composed of specialised muscle tissue . microscopically it resembles
striated muscle tissue which is conscious under control . functionally it resembles smooth
muscle because its contraction is involuntary. Therese fibers are arranged in an
interconnected manner that allows fro coordinated myocardial contraction and relaxation
Function of the heart conducting system
The specialised heart cells of the cardiac conducting system methodologically generate and
coordinate the transmission of electrical impulses to the myocardial cells .the result is
sequential atrioventricular contractioin which provides for the most effective flow of blood ,
thereby optimizing cardiac output . three physiologic characteristics of the cardiac
conduction cells account for this co-ordination
Automaticity : ability to initiate an electrical impulse
Excitability : ability to respond to an electrical impulse
Conductivity : ability to transmit an electrical impulse from one cell to another .
The sinoatrial node SA node referred to as the primary maker of the heart is located at
the junction of the superior vena cava and the right atrium . the SA node in a normal heart
resting heart has an inherent firing rate of 60 to 100 impulses per minute , but the rate can
change in response to the metabolic demands of the body .
The electrical impulses initiated by the SA node are conducted along the myocardial
cells Of the atria via specialized tracts called inter nodal pathways . .the impulse cause
electrical stimulation and subsequent contraction of the atria .the impulses are then
4
5. conducted to the atrio ventricular node the AV consists of another group of specialised
muscle cells similar to those of SA node
The AV node coordinates the incoming electrical impulses from the atria and after a
slight delay , relays the impulse to the ventricles . the impulse is the conducted through a
bundle of his that travel in the septum separating the left and right ventricles . the bundle of
his divides into the left and right bundle branch . to transmit impulses to the largest chamber
of the heart the left bundle branch bifurcates into the left anterior and left posterior bundle
branches . impulse travel through the bundle branches to reach the terminal point in the
conduction system called purkinje fibers . .this is the point at which the myocardial fiber are
stimulated causing ventricular contraction ;
The heart rate is determined by the myocardial cells within the fastest inherent firing
rate under normal circumstances the SA node has the highest inherent rate , the AV node
has the second inherent rate and the ventricular rates has the lowest inherent rate
3 PHYSIOLOGY OF THE HEART
3.1Physiology of cardiac contraction
Cardiac electrical activity is the result of the movement of ions across the cell
membrane . the electrical changes recorded within a single cell result what is known as
cardiac action potential In the resting state , cardiac muscle cells are polarized , which means
an electrical difference exists between the negatively charged inside and the positively
charged outside of the cell membrane . as soon as an electrical impulse is initiated , cell
membrane permeability changes and sodium moves rapidly into the cell , while potassium
cells exists the cell. The ionic exchange begins depolarization . contraction of the
myocardium follows depolarization.
The interaction between changes in membrane voltage and muscle contraction is
called electro mechanical coupling . as one cardiac muscle cell is depolarized , it act as a
stimulus to its neighbouring cells causing it to depolarize . sufficient depolarization of a
single specialzed conduction system cells results in depolarization and contraction of the
entire myocardium . Repolarisation return of cells to its resting stage occurs as the cell
returns to its baseline or resting state this corresponds to the relaxation of myocardial fibers
.
3.2Cardiac cycle
Beginning with systole , the pressure inside the ventricles rises rapidly forcing the
atrioventricular valves to close . as a result blood cease to flow from the right atria into the
5
6. ventricles and regurgitation of blood into the atria is prevented . the rapid rise of pressure
inside the right and left ventricles forces the pulmonic and aortic valves to open and blood is
ejected into the pulmonary artery and aorta , respectively . the exist of blood is at first rapid
then as the pressure in each ventricle and its corresponding artery equalizes , the flow of
blood gradually decreases.
At the end of the systole , pressure within the right and left ventricles rapidly decrease ,this
lowers pulmonary and aortic pressure causing closure of the semilunar valves .
During the diastole when the ventricles are relaxed the atrio ventricular valves are open ,
blood returning from the veins flow into the atria and then into ventricles .
3.3Cardiac output
It is the amount of blood pumped by each ventricle during a given period . the cardiac
output in arresting adult is about 5l per minute but varies depending on the metabolic needs
of the body . it is computed by stroke volume heart rate .
Stoke volume is the amount of blood ejected per heart beat . the average resting stroke
volume is about 70ml and the heart rate is 60 to 80 bpm
Electrical Activity of the Heart
When vertebrate muscles are excited, an electrical signal (called an "action potential") is
produced and spreads to the rest of the muscle cell, causing an increase in the level of
calcium ions inside the cell. The calcium ions bind and interact with molecules associated
with the cell's contractile machinery, the end result being a mechanical contraction. Even
though the heart is a specialized muscle, this fundamental principle still applies.
One thing that distinguishes the heart from other muscles is that the heart muscle is a
"syncytium," meaning a meshwork of muscle cells interconnected by contiguous cytoplasmic
bridges. Thus, an electrical excitation occurring in one cell can spread to neighboring cells.
Another defining characteristic is the presence of pacemaker cells. These are specialized
muscle cells that can generate action potentials rhythmically.
Under normal circumstances, a wave of electrical excitation originates in the pacemaker cells
in the sinoatrial (S-A) node, located on top of the right atrium. Specialized muscle fibers
transmit this excitation throughout the atria and initiate a coordinated contraction of the atrial
walls. Meanwhile, some of these fibers excite a group of cells located at the border of the left
atrium and ventricle known as the atrioventricular (A-V) node. The A-V node is responsible
for spreading the excitation throughout the two ventricles and causing a coordinated
ventricular contraction.
ASSESSMENT
The assessment of the acutely ill cardiac patient will be different from that of a patient with
a stable or chronic conditions
4 History collection
The nurse obtain the health history from the patient about the onset and severity of
chest discomfort , associated symptoms current medications and allergies
The nurse observes the general appearance and evaluates hemodynamic status
6
7. With a table patients , a complete health history is obtained during the initial contact
It is helpful to have the patient’s spouse or family members available during history
Initially demographic information regarding age , gender and ethnic origin is obtained
The family history including genetic abnormalities should be obtained .
Height , weight should be obtained
During the interview the nurse conveys the sensitivity to the cultural background and
religious practices of the patient this removes barrier to communication .
The baseline information derived from the history assists in identifying patient
condition and educational , self care needs . once the problem has been clearly
identified a plan of care is started . during subsequent contacts or visits with the
patient , a more focused health history is performed to determine whether goals have
been met whether the plan needs to be modified and whether new problems have
arised .
When a patient has chest discomfort ,questions should focus on differentiating a
serious life threatening condition such as MI from conditions that are less serious or
that would be treated differently
The following points should be remembered when assessing patients with cardiac
symptom
Women are likely to present with atypical symptoms of MI than men
There is little coordination between the severity of the chest and the
gravity of its cause
Elderly and people and those with diabetes may not have pain with angina
or MI because of neuropathies . fatigue and shortness of breath may be the
predominant symptom in these patients
There is poor correlation between the location of chest discomfort and its
source .
History of present health concern
COLDPSA
Character – describe the sign or symptom . how does it feel , look ,, sound, smell and so
forth?
Onset – when did it begin
Location – where is it ? d oes it radiate ?
Duration – how long does it last? Does it recur?
Severity – how bad is it ?
Pattern – what makes it better ? what makes it worse ?
Associated factors- what other symptoms occur with it ?
Chest pain: Chest pain can be cardiac , pulmonary ,
Do you experience chest pain ? muscular , gatroin testinal in origin angina is
When did it start? usually described as a sensation of squeezing
7
8. Describe the type of pain , location , radiation , around the heart . a steady severe pain ‘and a
duration and how often you experience the pain . sense of pressure . it may radiate to the left
does activity make the pain worse ? shoulder and down the left arm or to the jaw .
Did you have perspiration with the chest pain ? diaphoresis and pain worsened by activity
usually related to cardiac chest pain
Palpitations It may occur with the abnormalities of the
.do you experience palpitations . heart’s attempt to increase cardiac output by
increasing the heart rate it cause the patient
to feel anxious
Qther symptoms Faitgue may result from compromise cardiac
Do you tired easily ? output fatigue related to decreased cardiac
Do you experience fatigue? output is worse in the evening or as the day
Describe when the fatigue is started . was it progresses
sudden or gradual ?
Do you notice it at any particular time of day
Do you have difficulty in breathing Dyspnea may result from CCF , pulmonary
disorder , CAD, MI,..dyspnea may occur at
rest , during sleep or with mild , moderate ,
or extreme exertion
Do you wake up at night to urinate? Increased renal perfusion during periods of
How many times a day ? rest or recumbence may cause nocturia .
decreased frequency may be related to
decreased CO
Do you experience dizziness It may indicate decreased blood flow to the
brain due to myocardial damage . , however,
there are several other causes fro dizziness
such as inner ear syndromes , decreased
cerebral blood flow , and hypertension .
Do you experience swelling in your feet , ankles It may occur as a result of heart failure
,or legs
Do you have frequent heart burn ? Cardiac pain may be overlooked or mis
When does it /occur ? interpretated as gastro intestinal problems
What relieves it ?
How often you experience it
Past health history Congenital or acquired defects affect the
heart’s ability to pump, decreasing the
Have you been diagnosed with a heart defect or oxygen supply to the tissues.
a murmur?
Have you ever had rheumatic fever It results in inflammation of the all layers
of the heart
have you ever had an ECG It helps to identify any myocardial changes
Have you ever had a blood test outside? Elevated cholesterol level indicates the risk
for developing atherosclerosis
Do you take medications for heart disease? To know any adverse effects sometimes
clients may skip diuretics because of
frequent urination
Do you monitor your own blood pressure or Self monitoring is necessary for the person
heart rate? who is on cardiotonic or anti hypertensive
medications
8
9. Family history A genetic pre disposition prone for
Is there a history of hypertension ,MI, CAD developing heart disease .
,DM,in your family
Lifestyle and health practices It increase the risk for heart disease
Do you smoke ? how many cigarettes per day ?
and for how many years?
What tyoe of stress do you have in your life
style ?
Describe what you usually eat in a 24 – hour
period ?
How much alcohol you consume ?
Do you exercise /
Describe your daily activities ?
Has your heart disease affects your sexual
activity ?
How many pillows do you use to sleep at night ? If heart function is compromised , cardiac
Do you feel rested in the morning ? output to the kidneys is reduced during
Do you get up to urinate in the morning ? episodes of activity
5 PHYSICAL EXAMINATION
A physical examination is performed to confirm the data obtained in the health history . in
addition to observing the patient’s general appearance , a cardiac physical examination
should include an evaluation of the following
Effectiveness of the heart as a pump
Filling volumes and pressures.
Cardiac output
Compensatory mechanism.
The examination which proceeds logically from head to toe can be performed in ten minutes
with practice and covers the following
Preparing the client
Explaining the procedure to the patient
Provide privacy in case of assessing female patients in addition the client will be asked to
assume a left lateral position , sitting up and leaning forward so that the examiner can
ascultate for the presence of any abnormal heart sounds ..
Equipment
Sthetscope .
Small pillow .
Examination light
Watch with second
Centimeter ruler .
Physical examination
Assessment Normal findings Abnormal findings
Inspection The apical impulse may or Pulsation , which may also
9
10. Inspect pulsations not be visible if apparent ,it be called heaves or lifts ,
With the client in supine would be in the mitral area other than apical pulsation or
position with the head of the left midclavicular line 4th , 5th considered abnormal should
bed elevated between the 30 intercostals space . the apical be evaluated .
and 45 degrees , stand on the impulse is the result of the
client’s right side and look left ventricle moving towards
for the apical impulse and during systole.
any abnormal pulsations .
Palpation The
Palpate the apical impulse
remain on the client’s right
side and ask the client to
remain supine . use the
palmar surfaces your hand to
palpate the apical impulse in
the mitral area 4th , 5th
intercostals space at the mid
clacvicular line
Palpation :
Making sure that your hands are warm and with the patient rsupine, feel the
precordium .
Use the proximal halves of the four finger held gently together , or the whole hand
Touch gently and let the cardiac movements rise to your hand because sensation will
decrease as you increase pressure.
Begin at the apex , move to the left sterna border and then move to the base , going
down to the right sterna border and into the epigastrium or axillae .
Feel for the apical impulse and identify its location by the intercostals space and the
distance from the mid sterna line
Determine the width of the area in which is felt . usually it is palpable . within a small
radius
Not more than 1 cm . the impulse is usually gentle and brief . if it is vigorous
characterize it as heave or lift . in many adults it may not be able to feel because of
the thickness of the chest wall .
An apical impulse that is more forceful and widely distributed fills systole or is
displaced laterally downwards may indicate increased cardiac output or left
ventricular hypertrophy .
A lift along the left sternal border may caused by right ventricular hypertrophy .
A loss of thrust may be related to overlying fluid or air or to displacement beneath
the sternum .
Displacement to the right without a loss organ in thrust suggests dextro cardia ,
diaphragmatic hernia , distended stomach , or a pulmonary abnormality the point at
which the apical impulse is most readily see or felt should be described as the point
of maximal impulse PMI.
10
11. Feel for a thrill : a fine palpable , rushing vibration , s palpable murmur , often but not
always , over the base of the heart in the area of the right or left 2nd intercostals space
.. it grnerally indicates a disruption of of the expected blood fllow related to some
defect in the closure of one of the semilunar valves , pulmonary hypertension , or
atrial septal defect .
While palpate the precordium , use your other hand to palpate the carotid artery so
that you can describe the carotid pulse in relation to the cardiac cycle .
Percussion
It is limited in defining the eborderrs of the heart or determining its size , because the
shape of the chest is relatively rigid and can make more malleable heart conform .
Left ventricular size is determined by the location of the apial impulse .
The right ventricular tends to enlarge in the antero posterior diameter rather than
laterally thus determining the value of percussion of the right heart border.a chest x-
ray is more useful in determining the heart borders
Characteristics of pain
Types Character and Duration Precipitating Relieving
location and events measures
radiation
Substernal or 5-15 mt Usually related Rest , NTG,
retrostenal pain to exertion , oxygen
spreading across emotion , eating
chest, may cold
radiate to inside
of arm , , neck
or jaw
Substernal pain More than 15 mt Occurs Morhine
or pain over spontaneously sulphate ,
precordium but may be successful
may spread sequelae to reperfusion of
widely unstable angina blocked
throughout chest coronary Artery
. pain in hands
and shoulders
may be present
Sharp severe Intermittent Sudden onset , it Sitting upright ,
substernal pain increases with analgesia, anti
or pain to the swallowing , inflammatory
left of sternum coughing , and medications
,may be felt in rotation of
epigastrium and trunk
may be referred
to neck ,arms,
and back
Pleuritic pain Pain arises from 30+min Often occurs Rest time ,
inferior portion spontaneously treatment of
of pleura , may pain occurs or underlying
11
12. be referred to increases with cause,
costal margins inspiration bronchodilators
or upper
abdomen ,
patient may be
able to localise
pain
Esophageal pain Substernal pain 5-60 min Recumbency , Food , antacid,
may be cold liquids, NTG relieves
projected exercise pain
around chest to
shoulders
Anxiety Pain over chest 2-3 min Stress, Removal of
may be variable, emotional , stimulus ,
does not radiate tachhypnea, relaxation
, patient may
complaints of
numbness and
tingling of hands
and mouth
General appearance
Cognition
Skin
BP
Arterial pressures
Jugular venous pulsations and pressures
Heart
Extremities.
Lungs .
Abdomen .
Inspection
The room should be quiet because subtle , low pitched sounds are hard to hear
Stand to the patient’s right , a thorough examination of the heart requires the patient to
assume a variety of position s sitting erect, and leaning forward, lying supine , and
being in the left lateral recumbent position ‘in most adults the apical impulse should be
visible at the midclavicular line in the 5th intercostals space , but it is easily obscured
by obesity , large breasts, or muscularity . in some patient s it may be visible in the 4th
left inter costal space. The apical impulse may become visible only when the patient
sits up and the heart is brought closer to the anterior wall
A readily visible and palpable impulse when the is supine suggests an intensity that
may be the result of a problem and also important to assess the inspection of skin .
Palpation
Making sure that your hands are warm and with the patient supine , feel the
precordium . use the proximal halves of the four fingers held gently together or the
12
13. whole hand . touch gently and let the cardiac movements rise to your hand , because
sensation will decrease as you increase pressure .
Start at the apex, move to the left sterna border and then to the base , going down to
the right sterna order and into the epigastrium .
Feel fro the apical impulse and identify its location , by the intercostals space and the
distance from the mid sternal line .the impulse is generally gentle and brief .
Feel fro a trill , a fine palpable, rushing vibration , a palpable murmur , often , but not
always over the base of the heart in the area of the right or left 2nd intercostals space .
it generally indicates disruption of the expected blood flow related to some effect in
closure of the semilunar valve
While palpating the precordium , use your other hand to palpate the carotid artery .
it is located just medial to the and below the angle of the jaw.
Percussion
Percussion is of limited value in defining the borders of the heart or determining its
size , because the shape of the chest is relatively rigid and can make the more
malleable heart conform ‘left ventricular heart size is better judged by the location of
the apical impulse .
The right ventricular tends to enlarge in the antero posterior diameter , rather than
laterally .thus diminishing the value of percussion of the right heart border . a chest x-
ray is far more useful in defining the heart borders .
Begin tapping at the anterior axillary line, moving medially along the inter costal
spaces toward the sternal border . the change from a resonant to a dull sound marks
the cardiac border .
Note theses points with pencil and the outline of the heart is visually defined .
On the left the loss of resonance will generally be close to the point of maximal
impulse at the apex of the heart . measure this point from the mid sterna line at each
inter costal spaces.
Auscultation
Always place a comfortable warm stethoscope on the naked chest .
Comfort is important make the patient is warm and relaxed before beginning. Instruct
the patient when to breathe comfortably and when to hold the breath in expiration
and inspiration .
Listen carefully for each sound , isolating each component of the cardiac cycle ,
especially while the respirations are momentarily suspended . the following sequence
is suggested .
o Patient sitting up and leaning slightly forward and preferably in expiration : this is
the best position to hear relatively high –pitched murmurs with the stethoscope
diaphragm .
o Patient supine : listen in all five areas .
o Patient left lateral recumbent : listen in all five areas . this is the best position to
hear the low pitched filling sounds in diastole with the stethoscope bell
o Other positions depend on your findings
13
14. o Patient right lateral recumbent: this is the best position for evaluating right
rotated heart of dextro cardia . listen in all five areas
As you examine each of the five auscultatory areas , , remember to inch along . a full
evaluation cannot be obtained by jumping from one isolated area to the next . at each site
pause and listen selectively for each component of the cardiac cycle . let your stethoscope
follows the sounds wherever they lead
o Assess the rate and rhythm of the heart , noting the auscultatory area in which you
are listening each time .
o Instruct the patient to breathe normally and then hole the breath in expiration
o Concentrate on systole, listening for any extras sounds or murmurs. S1 marks the
beginning of systole .
o Concentrate on diastole , which is a longer interval than systole , listening for any
extra sounds or murmurs .
o Inhale the patient to inhale deeply ,listening closely for s2 to become two
components during inspiration . split s2 is best heard in the pulmonic auscultatory
area .
o Basic heart sounds are characterized in much the same way as respiratory and
other body sounds by pitch , intensity , duration , and timing in the cardiac cycle .
5.1 General appearance and cognition
The nurse observes the patient’s level of distress , level of consciousness and thought
process as an indication of the heart’s ability to propel oxygen to the brain
The nurse observes for evidence of anxiety along with any emotional factors .
5.2 Inspection of the skin
It includes assessing the skin color , temperature , and texture .
Pallor – decrease in color of the skin is caused by lack of oxyhemoglobin it is
observed in the finger, nails, lips and oral mucosa . in patient ‘s with dark skin , the
nurse observes in the palm of the hands and soles of the feet
Peripheral circulations –it occurs due to decreased flow rate of blood to a particular
area which allows more time for the hemoglobin molecule to become desaturated .
Central cyanosis – a bluish tinge observed in the tongue and buccal mucosa denotes
serious cardiac disorders .
Xanthelasma – yellowish slightly raised plaques in the skin , may be observed along
the nasal portion of one or both eyelids and may indicate elevated cholesterol levels.
Reduced skin turgors with dehydration and aging
Temperature and moisteness .
Ecchymosis – patients who are receiving anti coagulant therapy should be observed
for unexplained ecchymosis.
Wounds ,scars and tissue should be examined
5.3 Blood pressure
BP can be measured with the use of invasive arterial monitoring systems by a
sphygmomanometer and stethoscope
14
15. Assess for pulse pressures and postural blood pressure changes.
5.4 Arterial pressures
Assess the pulse rate which varies from patient to patient
Asses the pulse rhythm. For the initial cardiac examination or if the pulse rhythm is
irregular , the heart rate should be counted by auscultating the apical pulse for a full
minute while simultaneously palpting the radial pulse .
Assess the pulse quality , it should be assessed bilaterally ,scales can be used to
assess the strength of the pulse such as
Pulse not palpable or absent
o +1 weak , thread pulse difficult to palpate
o +2 diminished pulse cannot be obliterated
o +3 easy to palpate
o +4 strong bounding pulse may be abnormal
Assess for pulse configuration . the true configuration of the pulse is best appreciated
by palpating over the carotid artery rather than the distal radial artery .
5.5 Jugular venous pulsations
This provides a mean of estimating central venous pressures which reflects right
ventricular end diastolic pressure
Assess for jugular venous pulsations and distension
5.6 Heart inspection and palpation
Aortic area to determine the correct intercostals space at the angle of Louis by
locating the bony ridge near the sternum , at the junction of the body and manubrium .
from this angle locate the 2nd intercostals space by sliding one finger to the left or
right of the sternum
Pulmonic areas -2nd intercostals space to the left of the sternum
Erb’s point -3rd intercostals space to the left of the sternum
Right ventricular or tricuspid area -4th an 5th intercostals spaces to the left of the
sternum
Left ventricular or apical area – the PMI, location on the chest where heart
contractions can be palpated
Epigastric area – below the xiphoid process.
5.7 Percussion
Normally only left border of the heart can be detected by percussion . it extends from
the sternum to the mid clavicular line in the 3rd to 5th intercostals spaces
Unless the nurse detects a displaced apical impulse and suspects cardiac enlargement ,
percussion is omitted
5.8 Cardiac auscultation
Auscultate the heart sounds and be in a position to differentiate from the abnormal
sounds
During auscultation the patient remain supine position , using the diaphragm of the
stethoscope , the examiner starts at the apical area and progress upward along the left
15
16. sternal border to the pulmonic and aortic valve , the auscultatory findings ,
particularly murmurs should be documented by
o Location on chest wal
o Timing of sound either during systole or diastole .
o Intensity of the sound
o Quality and location of the sound
5.9 Inspection of the extremities
The hands , arms , legs and feet are observed for skin and vascular changes
o Decreased capillary refill
o Vascular changes such as quality of pulse , numbness, paraesthesia , decrease
in temperature , pallor , and loss of movement.
o Haemotoma
o Peripheral edema
o Clubbimg of fingers
o Lower extremity ulcers
5.10 Other Systems
Lungs
Tachypnea
Cheyne stroke respiration
Hemotypsis
Cough
Crackles
Wheezes
Abdomen
Hepato jugular reflex
Bladder distension
6. DIAGNOSTIC EVALUATION
Diagnostic studies and procedures are used to confirm the data obtained by the history and
physical examination . some test are easy used to interpreted by expert clinicians . all tests
should be explained to the patient .
6.1 Laboratory tests
It may be performed for the following reasons
o To assist in diagnosing an acute MI
o To identify abnormalities of the blood
o To assess the degree of inflammation
o To monitor serum level of medications
o To screen generally for abnormalities
16
17. Blood chemistry
Lipid profile
Cholesterol, triglycerides, and lipoproteins should be measure to evaluate person risk for
atherosclerosis
Cholesterol levels
it is a lipid required for hormone synthesis and cell membrane formation elevated cholesterol
level are known to increase the risk for CAD disease.
Normal level cholesterol=200mg/dl
HDL =35-65mg/dl
Triglyceride =40-150mg/dl
Serum electrolyte level
Sodium , potassium and calcium ions are vital to cellular dpolarization and repolarization the
effect of an elevated potassium leads t o myocardial depression and ventricular irritability ,
both hypo and hyperkalemia leads to ventricular fibrillation or caridac stand still
Magnesium is integral to the absorption of calcium and the maintenance of potassium stores
Blood urea nitrogen level
BUN is an end product of protein metabolism and is excreted by the kidneys .
In the patient with cardiac disease , an elevated BUN level may reflect reduced renal
perfusion
Serum glucose level
It should be monitored because cardiac patient may also have diabetes .
Coagulation studies
PTT &aPTT are used to obtain the activity of the intrinsic pathway
PT measures the extrinsic pathway and also used to monitor the effects of therapeutic anti-
coagulation with warfarin
INR International Standardized Ratio provides a standard method for reporting PT levels . it
is maintained between 2.0 &3.0 fro patient with deep vein thrombosis , pulmonary embolism
, valvular heart disease , and between 2.5 &3.5 for patients with mechanical prosthetic heart
valve replacements.
Hematologic studies
Complete blood count
6.2Chest x-ray and fluoroscopy
A chest x-ray reveals size, contour , position of the heart . it reveals cardiac and pericardial
calcifications of the pulmonary circulation
17
18. Fluoroscopy allows visualization of the heart on a x- ray screen . it shows cardiac and
vascular pulsations and unusual cardiac contours
6.3 Electrocardiography
It is a diagnostic tool in assessing the cardio vascular system . it is a graphic recording of the
electrical activity of the heart , an ECG can be recorded with 12,15, or 18 leads , showing the
activity from the different reference points . it is obtained by placing disposable electrodes in
a standard positions on the skin , chest wall , and extremities . the heart electrical activity are
recorded in a graph paper.
6.4 Cardiac stress testing
It is a non invasive procedures to evaluate the effectiveness of cardiovascular system
response to stress. It helps to determine the followings
CAD
Cause of chest pain
Functional capacity of the heart after an MI or heart surgery
Effectiveness of antiarrthymic or antianginal medications
Dysrhythmias.
6.5 Echocardiography
It is anon invasive ultrasound test that is used to examine the size, shape , and motion of
cardiac structures .
It is apaticularly useful tool in diagnosing pericardial effusion determining the etiological
factors for heart murmurs, evaluating the function fo prosthetic heart valves , determining the
chamber size , and evaluating the ventricular wall motion ,
It involves transmission of high frequency sound waves into the heart through the chest wall
and recording the return signals . the ultrasound is generated by the hand held tranducer
applied to the front of the chest . an ECG is recorded simultaneously to assist with
interpreting the echo cardiogram
6.6 Radio nuclide imaging .
It involves the use of radio isotopes to evaluate coronary artery perfusion noninvasively to
detect MI and to assess left ventricular function . thallium 201 and technetium 99m are two of
the most common radio isotopes used in cardiac nuclear studies . as they decay they give off
small amounts of energy in the form of gamma rays , when they are injected intravenously
18
19. into the blood stream the energy emitted by the radioisotope can be detected by a gamma
scintillation camera positioned over the body
6.7Computed tomography
CT scanning or electron beam CT , uses x-ray to provide cross sectional images of the chest ,
including the heart and great vessels . these techniques used to evaluate cardiac massages and
disease of the aorta and pericardium .
Nursing role
Patient preparation is the primary role in of the nurse for these tests
The procedure is non invasive an painless
To obtain adequate images , the patient must lie perfectly still during the scanning
process.
An intravenous line is necessary if contrast enhancement is to be used
6.8Positron emission tomography
It is anon invasive scanning method that was used in the past primarily to study
neurologic function . more recently it has been used to diagnose cardiac dysfunction .
it provides specific information about myocardial perfusion
During a PET scan , radioisotopes are administered by injection , one compound is
used to determine blood flow in the myocardium and another shows the metabolic
function
Nursing interventions
Instruct the patient to refrain from using tobacco or ingesting caffeine for 4 hours
before the procedure
Reassure the patient
6.9Magnetic resonance imaging
It is a noninvasive painless technique that is used to examine both the anatomic and
physiologic properties of the heart ..
It is valuable in diagnosing the diseases of the aorta, heart muscle , pericardium , as well as
congenital heart lesion s
6.10Cardiac catheterization
19
20. It is an invasive procedure in which radio opaque arterial and venous catheters are introduced
into selected blood vessels of the right and left side of the heart . most commonly the
catheters are inserted percutaneously through the blood vessels or via cut down procedure if
the patient ha spoor vascular access. During catheterization , the patient has an IV line in
place for the administration of sedatives , fluids , heparin , and other medications .radio
opaque isotopes are used to visualize the coronary arteries , some contrast against iodine
.diagnostic catheterization are commonly preferred for an out patient basis and require 2 to 6
hours of bed rest.
Patients hospitalized for angina or acute MI may also rquire cardiac catheterization , . after
the procedure , these patient usually return to the hospital rooms for recovery.
6.11Angiography
Cardizc catheterization , is usually performed with angiography , a technique of injecting a
contrast agent into the vascular system to outline the heart and blood vessesls. When a
particular heart chamber or blood vessels is singled out for study the procedure is known as
selective angiography. . common sietesare the aorta, coronary arteies, and the right and left
sides of the heart .
6.12 Aortography
An aortogram is a form of angiography that outlines the lumen of the aorta and the major
arteries arising from it . the catheter may be introduce into the aorta using the translumbar or
retrograde brachial or femoral artery approach .
Right heart catheterization ,
It usually precedes with left heart catheterization , it involves the passage of catheter from an
antecubital or femoral vein into the right atrium right ventricle , pulmonary artery
,pulmonary arterioles.
Left heart catheterization ,
It is performed to evaluate the patency of the coronary artery and the function of the left
ventricles & the mitral and aortic valves. . after the procedure , the catheter is withdrawn and
arterial hemostasis is achieved using manual pressure or other techniques.
Nursing interventions
Before catheterization ,
Instruct the patient to usually fast fro 8-12 hours before the procedure
Prepare the [patient .
Reassure the patient with mild sedatives.
Encourage the patient to experience certain fears and anxieties .
After catheterization ,
Observe the catheter access
20
21. Evaluate temperature, color of the site .
Monitor for dys rhythmias.
Instruct the patient to report any chest pain and bleeding or discomfort .
Encourage fluids to increase urinary output and flush out the dye
6.13 Hemodynamic monitoring
Critically ill patient require continuous assessment of their cardiovascular system to diagnose
and manage their complex medical conditions. This is mostly achieves by central venous
pressure monitoring , CVP, pulmonary artery pressure monitoring , intra arterial BP
monitoring
To perform invasive monitoring specialized equipment is necessary which includes
A CVP , pulmonary or arterial catheter .
A flushed system composed of intravenous solution , tubing’s stopcocks, .
A pressure bag placed around the flush solution that is maintained at 300 mm of hg
A transducer to convert the pressure coming from the artery or heart chamber into an
electrical signal.
An amplifier or monitor which increase size of the electrical signal for display .
Central venous pressure monitoring
It is used to assess the right ventricular function and venous blood return to the heart this
can be measured by connecting either a catheter positioned in the vena cava or the proximal
part of a pulmonary monitoring system . before insertion of CVP , the site is prepared by
shaving , a local anesthetic may be used
The physician threads a single lumen multilumen catheter through the external jugular ,
cubital or femoral vein into the vena cava just above or within the right atrium .
Nursing interventions
Once the CVP catheters is secured and a dry sterile dressing is applied .
It is confirmed by chest x-ray and the site is inspected daily for infection
Dressing should be changed under aseptic techniques.
To measure the CVP the transducer or the zero mark on the manometer must be used at a
standard reference point called the phlebostatic axis . after locating this position , the nurse
may make an ink mark on the patient’s chest to indicate the location it can be measured
correctly with the patient at supine position up to a 45 degree
The range for normal CVP is 0- 8 mm H g
Pulmonary artery pressure monitoring
It is used for assessing the left ventricular function ‘it is achieved by using a pulmonary artery
catheter and pressure monitoring system .the catheter is inserted into a large vein , the
catheter is inserted into the vena cava and right atrium . in the right atrium the balloon is
inflated and the catheter is carried rapidly by the flow of blood through the tricuspid valve
into the right ventricle through the pulmonic valve and into a branch of pulmonary artery
21
22. Normal pulmonary pressure is 25/9 mmHg with a man pressure 15 mmHg
Intra arterial blood pressure monitoring
It is used to ontain direct and continuous BP measurements in critically ill patients who have
severe hypertension or hypotension
Once an arterial site is selected ,collateral circulation to the area must be confirm before the
catheter is placed
With the Allen test the nurse compresses the radial and ulnar arteries simultaneously and
asks the patient to make a fist causing the hand to blanch . .
After the patient opens the fist the nurse releases the pressure on the ulnar artery while
maintaining pressure on the radial artery .the patient’s hand will turn pink if the ulnar artery
is present .
Nursing intervention s
Proper aseptic methods should be followed
A transducer is attached , pressures are measure in millimeters
7. CONCLUSION
So far we discussed about the cardio vascular assessment , throughout the continuum of
care , whether in a home , hospital , or rehabilitation setting , all patients with cardio vascular
disease require similar assessments .an accurate and timely assessment provides the data
necessary to identify diagnoses, formulate a plan of care and evaluate the respose of the
patient to the care needed.
22
23. 8. BIBLIOGRAPHY
1. 1. Fuller (2000) ,J, Health Assessment , A Nursing Approach , 3rd edn , Philadelphia :
Lippincott Williams and Wilkins publishers , Pp
2. Weber , J , (2007 ) Health Assessment In Nursing , 3rd edn , Philadelphia : Lippincott
Williams and Wilkins publishers , Pp:
3. Seidel , H.M (1999) Physical Examination , 5th edn Missouri : Mosby Publishers Pp
4. Smeltzer .C. Suzzane , Hinkle .I . Janice et al , Textbook Of Medical – Surgical Nursing
11th edn , Philadelphia : Lippincott Williams and Wilkins publishers , Pp:
23
24. SEMINAR ON
HEALTH ASSESSMENT OF
CARDIO VASCULAR SYSTEM
SUBMITTED TO SUBMITTED BY
MRS. FELICIA CHITRA MS.G.MUTHAMIZ SELVI
READE IN NURSING M.SCNURSING 1ST YEAR
MTPG&RIHS MTPG&RIHS
24
25. Submitted date on 22-2-11
INDEX
S.NO CONTENT PAGE NO
1 Introduction
2 Anatomy Of The Heart
2.1position
2.2 Heart Chambers
2.3heart Valves
2.4atrioventricular Valves
2.5semilunar Valve
2.6coronary Arteries
2.7cardiac Muscle
3
Physiology Of The Heart
3.1physiology Of Cardiac Contraction
3.2cardiac Cycle
3.3cardiac Output
4 History Collection
4.1 Health Perception And Management
4.2 Nutrition And Metabolism
4 .3 Elimination
4.4 Activity And Exercise
4.5 Sleep And Rest
4.6 Cognition And Perception
5 Physical Examination
5.1 General Appearance Band Cognition
5.2 Inspection Of The Skin
5.3 Blood Pressure
5.4 Arterial Pressures
25