
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Dr.r.subramaniyan, 09 3-17,Aqueous Humour Dynamics
Semelhante a Dr.r.subramaniyan, 09 3-17,Aqueous Humour Dynamics (20)
Mais de ophthalmgmcri
Mais de ophthalmgmcri (20)
Último
Último (20)
Dr.r.subramaniyan, 09 3-17,Aqueous Humour Dynamics
- 2. FUNCTIONS • Aqueous humor is a clear, colourless, watery solution continuously circulated from the posterior chamber throughout the anterior chamber. • Maintains the intraocular pressure. • Maintains the shape and the internal structural arrangement of the eye. • Cornea takes glucose and oxygen from the aqueous. • Lens uses glucose, oxygen and amino acids from the aqueous.
- 3. PHYSICOCHEMICAL PROPERTIES • VOLUME 0.31 ml • (o.25 ml in anterior chamber and 0.06 ml in posterior chamber) • Refractive index 1.336 • Density greater than water • Hyperosmotic ( compared to plasma) 3-5 mOsm/l • pH: acidic • Rate of formation: 2.3 µl/min. • Protein content less.
- 4. FACTORS AFFECTING COMPOSITION OF AQUEOUS HUMOUR • BLOOD AQUEOUS BARRIER • Protein and large molecular size substances are largely prevented from entering the cavities. This maintains the clarity of the media of the eye. • Formed by the tight junctions between the cells of epithelium of the ciliary body and endothelium of iris capillaries.
- 5. EFFECT OF BREAKDOWN OF BLOOD AQUEOUS BARRIER ON AQUEOUS HUMOUR COMPOSITION • Proteins and antibodies in aqueous equilibrate with those in plasma to form plasmoid aqueous (secondary aqueous). • Recognised clinically in slit lamp microscope as Tyndall Beam. • Fibrinogen appears in aqueous, which may allow the aqueous actually to clot. • Ionic composition of the aqueous approches same as plasma.
- 6. Aqueous humor production • Active secretion by double- layered ciliary epithelium. • Primarily derived from the plasma within the capillary network of the ciliary processes.
- 7. Aqueous humor • Secretion depends on: • Integrity of blood aqueous barrier • Blood flow to ciliary body • Neurohormonal regulation of blood and ciliary body • Adrenergic innervation
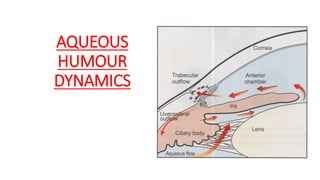
- 8. Aqueous humor outflow • Trabecular out flow (90%) • Uveoscleral out flow (10-20%)
- 9. Trabecular outflow channel Posterior chamber Anterior chamber Angle of anterior chamber ( Trabecular meshwork) Schlemm’s canal Collector channels Episcleral vein, aqueous vein
- 12. UVEA SCLERAL OUTFLOW • Pressure independent outflow • Responsible for 10-20 % of outflow Ciliary body Suprachoroidal space Venous circulation in the ciliary body, choroid, sclera
- 13. INTRAOCULAR PRESSURE • Refers to the pressure exerted by the intraocular contents on the coats of the eyeball. • IOP is maintained by the a dynamic equilibrium between the aqueous humour formation, aqueous humour outflow, and episcleral venous pressure. • Normal IOP is 10 – 21 mm Hg.
- 14. Factors affecting IOP • Rate of aqueous production • Resistance to aqueous outflow Pretrabecular , trabecular and post trabecular • Level of episcleral venous pressure.
- 15. Factors influencing IOP HEREDITARY • Age more than 40 • Time of the day: pressure highest in the morning, lowest in the evening Diurnal variation of More than 8 mm is considered pathognomonic of glaucoma. • Systemic venous pressure- external pressure of jugular veins, compression of superior vena cava by tumour, cavernous sinus thrombosis. • General anaesthesia decreases IOP (except nitrous oxide, ketamine) • Topical drugs • Blockage of the circulation of aqueous – angle of AC, pupillary block
- 17. VISUAL FIELD • Portion of space in which objects are simultaneously visible to the steadily fixating eye.
- 18. VISUAL FIELD EXAMINATION Screening tests • Confrontational visual field testing • Amsler grid (assesses the central 10° the visual field ) . Quantitative measurements using manual or automated perimetry
- 21. VISUAL FIELD DEFECTS • Relative paracentral scotoma • Roenne’s nasal step • Seidel scotoma • Arcuate scotoma • Double arcuate / ring scotoma • End stage / near total field defect
- 25. THANK YOU !!!