
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Oct
Semelhante a Oct (20)
Mais de Nikhil Rp
Último
Último (20)
Oct
- 1. OPTICAL COHERENCE TOMOGRAPHY Dr. Shaik Gohar Firdous Dr Nikhil R P
- 2. INTRODUCTION • OCT is a diagnostic technology,provides a cross sectional image of the anterior eye and retina in-vivo with a high resolution, similar to histological section. • OCT allows assessment of retinal disease, understanding of pathology and correlations between structure and function.
- 3. It allows detection and measurement of: • Morphological changes in retina • Retinal thickness • Retinal volume • Retinal nerve fiber layer thickness (RNFL) • Various parameters of the optic nerve head (ONH)
- 4. PRINCIPLE • Low coherence interferometry. Michelson Interferometer • A beam of light passes through semitransparent mirror that splits the beam into two. • These two beams are then thrown on two equidistant mirrors; reflected light from these mirrors is then picked up and summed up by a detector.
- 5. • The equidistant mirrors reflect the light wave in same phase; however, if one of the mirrors is moved by a distance less than the wavelength of the incident light, the reflected lights from the two mirrors will then possess a phase difference. • This phase difference then produces an interference pattern at the level of the detector.
- 8. • The resulting interference patterns are used to reconstruct an axial A-scan, which represents the scattering properties of the tissue along the beam path. • Moving the beam of light along the tissue in a line results in a compilation of A-scans with each A-scan having a different incidence point.
- 9. • From all these A-scans, a two-dimensional crosssectional image of the target tissue can be reconstructed and this is known as a B-scan. • OCT operates like a fundus camera but resolves like a USG machine. USG OCT • Source Sound waves Infrared light • Resolution 150 μ 10 μ • Patient contact Needed Non-invasive
- 10. TYPES OF OCT • Time Domain OCT • Spectral Domain OCT
- 11. • In TD OCT, image resolution and acquisition speed are inversely related. • Simultaneous increase in imaging speed and resolution can be brought about by spectral domain OCT (SD OCT).
- 12. DIFFERENCES TD-OCT • LIGHT SOURCE: 840nm • AXIAL RESOLUTION: 6-7µ • TRANSVERSE : 10µ • SCANNING SPEED : 28000 • SCAN DEPTH : 2mm • MAXIMUM ASCANS: 8000 SD-OCT • 820nm • 10µ • 20µ • 400 • 2mm • 512
- 13. Technique • In the presence of clear media and cooperative patients quality images can be taken even with a 3 mm pupil; otherwise dilatation is recommended. • The patient is seated comfortably in front of the OCT machine with chin positioned on the chin rest. He is asked to fixate on the fixation target. The internal fixation (green color light) target is the commonly used fixation target. Those patients who are unable to fixate with macula can focus with the opposite eye on an external target. After Fixation the operator selects the desired scan and aligns the instrument so that fundus image and scan beam is displayed on the screen.
- 14. Scanning protocols • The OCT software offers a variety of retinal scanning protocols including linear, circular, radial and parallel line scans • The duration of scan acquisition can be shortened by using fast scan protocols, which acquire three fast scans and averages them to give the final interpretation.
- 15. • The alignment algorithm reduces artifacts caused by axial movement of the eye during scan acquisition. • The normalization algorithm allows comparison of scans with varying signals. Apart from this the machine has Gaussian smoothing, proportional evaluation and profile algorithm scan for further refinement of the scan image • Application of gray scale image allows better sensitivity for detection of minute difference in the contrast. • A normative database is also available for comparison of peripapillary retinal nerve fiber layer as well as the macular thickness in the latest software.
- 16. Specific scanning protocols • Retina scanning protocols: Line scan, Raster lines, Cross hair, Radial lines, X-line and Circle. • Macular scanning protocols: Macular thickness scan, Fast macular thickness, Raster lines and Single line scan • RNFL scanning protocols: RNFL thickness protocol (3.4 mm), Fast RNFL thickness protocol (3.4 mm), Proportional circle, Concentric 3 rings, RNFL thickness (2.27Xdisc), RNFL map. • ONH scanning protocols: Optical disc scan and Fast Optical disc scan.
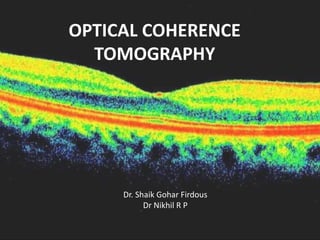
- 22. NORMAL RETINAL SCAN • Posterior hyaloid ,visible as very faint, fine and slightly reflective line. • Internal limiting membrane is clearly defined in the OCT scans due to contrast between the reflective retina and non-reflective vitreous. • The nerve fiber layer is highly reflective and more visible on the nasal side due to the density of papillomacular bundle.
- 23. • The fovea shows a characteristic depression on the macular scan. • The plexiform layers with reflectivity that is slightly greater than the reflectivity of the nuclear layers. • The outer retina is bounded by a highly reflective band (70 microns thick) that represents the retinal pigment epithelium.
- 24. • This band can be divided into three layers. • The first is thin and hyperreflective representing the junction of inner and outer photoreceptors. • The second of hyporeflective,outer segment • The third one is the thickest and most hyperreflective
- 25. • The Bruchs’ membrane and the choriocapillaris are seen as a single less reflective structure but in some scans the choriocapillaris may be visible separate from the RPE and the Bruchs’ membrane. • The larger retinal vessels are located indirectly by the shadow cone that they form on the posterior layers
- 26. • The OCT image can be displayed on a gray scale where more highly reflected light is brighter than less highly reflected light. • Alternatively, it can be displayed in color, colors correspond to different degrees of reflectivity. • Highly reflective:bright colors(red and yellow) • Low reflectivity:darker colors(black and blue). • Intermediate reflectivity -green.
- 29. • First generation OCT became available in 1996 as Humphrey Optical Coherence Tomography Scanner. • Infrared light source with wavelength of 850 nm,with a resolution of 10 to 17 μm.
- 30. • Commercial 3rd generation OCT (StratusOCT, Carl Zeiss Meditec, Dublin, CA) was introduced in 2002. Light source - super luminescent diode (SLD) Wavelength - 820 nm STRATUS OCT: Scanning speed - 400 A-scan/seconds (4х 1st gen). Axial resolution of 10 μm Transverse resolution of 20 μm.
- 31. Various newer OCT systems are: • Ultra-high resolution OCT • Combined OCT/SLO • Doppler-OCT • High Speed UHR-OCT • CAS OCT-Visante™ OCT • Polarization sensitive OCT • Combined FFA and en-face OCT • Intraoperative OCT
- 32. ULTRA HIGH RESOLUTION OCT • Axial resolution - 3 μm. • Transverse resolution - 15-20 μm. • Uses femto-second titanium sapphire laser that generates light with bandwidth of 125 nm centered at 815 nm. • Time for image acquisition is 4.3 sec(1.3 sec with Stratus OCT). • Hence, UHR OCT images need correction for axial motion.
- 33. • With OCT (Stratus OCT); GCL,ELM and photoreceptor details are not well visualized. • UHR OCT may be useful in evaluation of these retinal layers. 1.Showing photoreceptor integrity in patients with macular hole. Foveal photoreceptor degeneration is represented by outer hyporeflective disruptions of the junction between the inner and outer segments of the photoreceptors
- 34. 2.Detection of milder forms of ERM and vitreomacular traction. 3.Earlier detection of RNFL thinning and treatment of glaucoma patients. • UHR OCT can not only demonstrate focal RNFL changes before appearance of field defect but also detect progression of disease in an established case.
- 35. HIGH SPEED UHR OCT High Speed UHR-OCT uses SD OCT technology. • It allows simultaneous ultra-high speed and ultra-high resolution. • Imaging speed is 100 times faster than time domain UHR OCT. • 40 times faster than the standard- resolution OCT.
- 36. • It not only gives structural information but also functional retinal blood flow similar to Doppler ultrasound. • It may reduce the need for FFA.
- 37. • Raster scan to obtain 3-dimensional (3-D) images of ocular structure. • Quantitative mapping of retina layers, including measurements of the retinal thickness, RNFL photoreceptor layer and other intraretinal layers can be performed. • Its applications would be similar to that indicated for UHR-OCT.
- 40. COLOR DOPPLER OCT • CD OCT is the technique that combines laser Doppler velocimetry and OCT for imaging the depth, diameter, flow rate and retinal hemodynamic characteristics. • Color coded velocity data are superimposed on the conventional OCT image for CD OCT display. The direction and magnitude of blood flow are designated by red and blue color and intensity respectively.
- 41. • As it can measure blood flow profile in a few milliseconds it is able to show vascular autoregulation and response to changes in perfusion pressure, oxygen contents and following laser photocoagulation. • Presently only larger vessels near the optic disc have been mostly studied.
- 42. CORNEA ANTERIOR SEGMENT OCT • ASOCT with 1300 nm wavelength ASOCT was first reported by Radhakrishnan. • The CAS OCT image is a gray scale or false color two-dimensional representation of backscattered light intensity in a cross- sectional plane. • The scanning speed of the system is 4000 axial scans per second
- 43. • CAS OCT with a wavelength of 1.3-μm (present model) provides adequate resolution of both the cornea and the AC angle. • Detailed image of the cornea, iris root,angle recess, anterior ciliary body, scleral spur, and,in some eyes, the canal of Schlemm is possible.
- 44. ADVANTAGE OVER OTHERS • Being noncontact, the patient comfort, cooperation and safety is increased (pediatric) and there is no mechanical distortion of the tissue. • Provides more accurate biometry of anterior segment than Orbscan or Scheimpflug photography. • Though confocal scanning microscopy gives higher resolution than CAS OCT, it can scan only a small area of the eye at a time. • Unlike UBM, CAS OCT can perform measurements without any need of anesthesia or coupling medium. CAS OCT can also perform scanning of all 4 quadrants at a time.
- 45. OTHER USES • Measure corneal thickness, flap and residual posterior stromal bed following refractive surgery. • Important landmarks such as the scleral spur are more distinct in CAS OCT images. • Traumatic angle recession can be easily picked up. • Detecting gonioscopically occludable angle. • Also being used for imaging ocular surface and iris neoplasia.
- 46. LIMITATIONS • Speed and depth of penetration. • It cannot obtain clear images through opaque media. • Is obstructed by the eyelids making imaging of the superior and inferior angles difficult. • It provides limited visualization of the ciliary body.
- 47. INTERPRETATION EPIRETINAL MEMBRANE: • ERMs can be classified as idiopathic or secondary. • Idiopathic ERMs -fibroglial proliferation on the inner surface of the retina,secondary to a break in ILM,during posterior vitreous detachment. • Secondary ERMs result from an already-existing ocular pathology such as central or branch retinal vein occlusion, diabetic retinopathy, uveitis,and retinal breaks with or without detachment.
- 48. • ERMs are seen as a highly reflective layer on the inner retinal surface. • In most eyes, the membrane is globally adherent to the retina but,in some cases, it can be separated from the inner aspect of the retina, which enhances its visibility by OCT.
- 52. MACULAR HOLE • Macular hole is partial or full thickness dissolution of retinal tissue at the foveal region. • It may occur following blunt trauma, long- standing macular edema or as an idiopathic condition. • Pseudoholes are seen in dense sheet of ERM with a central defect that overlies the foveal center, giving the ophthalmoscopic appearance of a true macular hole.
- 53. OCT STAGING OF MACULAR HOLE • Stage 1 • Stage 1a: Foveolar detachment with yellow spot. OCT shows a cystoid space occupying the inner part of the foveal tissue. • Stage 1b: Foveolar detachment with yellow halo. OCT shows impending hole with extension of cystoid space posteriorly, disrupting the outer retinal layers. • Stage 2: Formation of minute eccentric holes. OCT shows eccentric opening of the roof of the hole with presence of an operculum (Figs 23.6 to 23.8).
- 54. • Stage 3: Full thickness macular hole with or without operculum. OCT shows a central full thickness macular hole with detached posterior vitreous. • Stage 4: Full thickness macular hole with posterior vitreous detachment. OCT shows a central full thickness macular hole with a cuff of subretinal fluid and completely detached posterior vitreous.
- 61. BERLINS EDEMA • Acute retinal opacification (macula or elsewhere) following closed globe injury. • Mild cases resolve spontaneously without any sequelae; severe cases result in permanent vision loss. • Histopathological features: • Disruption of photoreceptor outer segments • Phagocytosis of retinal pigment epithelial cells (RPE) • Intraretinal migration of RPE • Multilayered, disorganized RPE
- 62. • OCT findings depend on the severity and the duration of commotio retinae . • Photoreceptor disruption is seen as optically clear spaces in the area corresponding to the photoreceptors.
- 65. RETINAL ARTERY OCCLUSIONS • The clinical presentation depends on the type of vessel that is occluded. It may be asymptomatic or sudden rapid loss of vision or no PL. • The ophthalmoscopic include cotton wool exudates, opacification of retina and a cherry red spot.
- 66. OCT FINDINGS • Diffuse thickening of the neurosensory retina. • Increased reflectivity in the inner retinal layers, decreased reflectivity of the photoreceptor layers and the retinal pigment epithelium secondary to the shadowing effect. • Involvement of macula,of cystoid changes in the macular area with loss of the macular contour. • In old cases decrease in macular thickness.
- 68. RETINAL VENOUS OCCLUSIONS • Retinal thickening and cystoid macular edema (CME): Increase in retinal thickness is seen as loss of macular contour on OCT. In the area of retinal edema, presence of cystoid spaces with reduced reflectivity depicts CME. • Intraretinal and subretinal hemorrhages are seen as focal areas with bright and high reflectivity with back scattering. Area of shadowing appears as black spaces in the RPE and choriocapillaris layer
- 69. • Cotton wool spots are seen as highly reflective well demarcated areas with reduced reflectivity from outer retinal layers. • Optic disc edema is a common feature in CRVO. OCT can demonstrate disc edema and help in monitoring it in a quantitative manner.
- 71. AGE RELATED MACULAR DEGENERATION • Age related macular degeneration is the most common cause of blindness. • Early grades of the disease more frequent than the advanced grade. • Early stage – drusen • Advanced stage by geographic atrophy (non- exudative or dry form) choroidal neovascularization (exudative or wet form).
- 72. • Geographic atrophy - large area of irregular,well-defined chorioretinal atrophy involving the macula. • Exudative form-choroidal neovascular membrane and its sequlae like serous detachment, hemorrhagic detachment,exudation and distortion of the retinal photoreceptors.
- 73. • Drusen - hyper-reflective discrete protrusions within the RPE complex. • Active choroidal neovascular membrane - multi-layered, highly hyper-reflective fusiform or irregular mass with loss of retinal contour in the overlying region. • It may be located in the pre choriocapillaris region or in front of the pigment epithelial layer or in both these spaces.
- 77. CENTRAL SEROUS CHORIORETINOPATHY • Central serous chorioretinopathy is a noninflammatory, idiopathic serous detachment of the macula with or without associated RPE detachment. • Spontaneous resolution occurs - majority. Concurrent pigment epithelial detachments persist for a longer time despite resolution of the serous detachment.
- 78. • OCT to detect subtle serous detachments of the macula, either in the first episode, during recurrences or following treatment. • Serous detachment - hypo-reflective, shallow separation of the neurosensory retina from the RPE.
- 79. CSR
- 80. CSR with PED
- 81. CSR with PED
Notas do Editor
- A) Stage 1b macular hole and vitreofoveal traction; (B and C) Evolving into stage 2 macular hole (full thickness eccentric defect with operculum
- Stage 2 macular hole (full thickness eccentric defect with operculum
- full thickness defect with cystoid changes at the edge and pseudo-operculum
- nd yellow pigment deposit at the base of macular hol
- central area of retinal elevation and subneurosensory collection of moderate reflectivity material suggestive of fibrin along with retinal pigment epithelium detachment.