Bph dr mnr
•Transferir como PPT, PDF•
10 gostaram•1,332 visualizações

This document provides information on benign prostatic hyperplasia (BPH): - It describes the anatomy and zones of the prostate gland and discusses theories on the causes of BPH related to hormone levels and aging. - The pathology, clinical features, investigations, management options including medications, minimally invasive procedures, and surgeries for BPH are summarized. Surgical options include transurethral resection of the prostate (TURP) and newer laser procedures. - Complications of treatments like TURP are noted. Indications for medical versus surgical management are provided.

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Bph dr mnr
Semelhante a Bph dr mnr (20)
Mais de SREE GOKULAM MEDICAL COLLEGE AND RESEARCH FOUNDATION
Mais de SREE GOKULAM MEDICAL COLLEGE AND RESEARCH FOUNDATION (11)
Último
Último (20)
Bph dr mnr
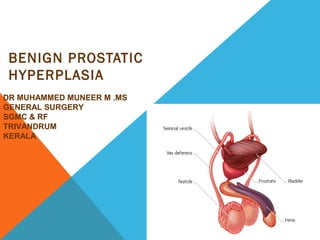
- 1. BENIGN PROSTATIC HYPERPLASIA DR MUHAMMED MUNEER M .MS GENERAL SURGERY SGMC & RF TRIVANDRUM KERALA
- 2. Sagittal View of the Prostate Rectum Seminal vesicle Denonvillier's fascia Deep transverse perineal muscle Puboprostatic ligament Plexus of Santorini Anterior lobe Posterior lobe Middle lobe Pubic bone Penis and Urethra Base of prostate Apex of prostate
- 3. SAGITAL SECTION OF THE PROSTATE GLANDSAGITAL SECTION OF THE PROSTATE GLAND Seminal Vesicle Central Zone Bladder Peri-urethral zone Anterior Zone Fibro-muscular Peripheral Zone Transition Zone Urethra
- 6. THEORIES • It is an involuntary hyperplasia due to disturbance of ratio of circulating androgen and estrogen. Hypothalamus-pulsatile release of LHRH---- release of LH from anterior pituitary stimulate leydig cells of testis -release testosterone - reaches prostate- releases 5 alpha reductase of prostate - convert TS to DHT for its effect. DHT is 5 times more potent than TS. 90% of TS from testis ,10% TS from adrenal cortex With age TS level drops slowly. But fall of oestrogen level is not equal . So enlarges through intermediate peptide growth factor.
- 7. BPH • BPH arises from submucosal glands of periurethral transitional zone with stromal proliferation and adenosis. It eventually compresses the peripheral zone and enlarges as lateral lobe. • BPH arising from subcervical glands of central zone enlarges as middle lobe projecting up into the bladder with in the internal spincter • Most common benign internal neoplasm of the adult male. • BPH due to hyperplasia and hypertrophy with increased glandular and stromal elements of the prostate in varying amounts
- 8. PATHOLOGY • BPH involves adenomatous zone of prostate, ie submucosal glands .(TZ) • Median lobe enlarges in to the bladder • Lateral lobe narrow the urethra causing obstuction • Urethra above the verumontanum gets elongated and narrowed • Bladder initially takes the pressure burden causing trabeculations, sacculations and later diverticula formation.
- 11. • Enlarged prostate compress the prostatic venous plexus causing congestion ,called as vesical piles leading to hematuria. • Back pressure causes hydroureter and hydronephrosis • Secondary ascending infection can cause acute or chronic pyelonephritis. • It can even cause severe obstruction can lead to obstructive uropathy with renal failure
- 12. CLINICAL FEATURES • The enlarged gland contribute to the overall lower urinary tract symptoms (LUTS) complex via two routes: • (1) direct bladder outlet obstruction (BOO) from enlarged tissue (static component) • (2) from increased smooth muscle tone and resistance within the enlarged gland (dynamic component). • Voiding symptoms have often been attributed to the physical presence of BOO. • Detrusor overactivity is thought to be a contributor to the storage symptoms seen in LUTS
- 13. LUTS SYMPTOMS OF VOIDING • Hesitancy • Poor flow not improving by straining • Dribbling even after micturition • Intermittent stream- stops and starts • Sensation of poor bladder emptying • Episodes of near retention SYMPTOMS OF STORAGE • Frequency • Nocturia • Urgency • Urge incontinence • Nocturnal incontinence
- 14. CONSEQUENCES OF BPH • No symptoms , no BOO • No symptoms ,but urodynamic evidence of BOO • LUTS, no e/o BOO • LUTS and BOO • Others (a/c , c/c retention, hematuria,UTI,, stone formation.) • LUTS assessed by means of scoring systems,which give a semi objective measure of severity. • The AUA-SI and the International Prostate Symptom Score (I- PSS) are nearly identical, short questionnaires are used to assess the severity of:- • 3 storage symptoms (frequency, nocturia, urgency) and • 4voiding symptoms- (feeling of incomplete emptying, intermittency, straining, and a weak stream).
- 15. IPSS SCORE • Mild- IPSS <7 FLOW RATE >15 RV < 100 • MODERATE -IPSS 7-20 FLOW RATE <I5 ml rv <200 • Sever IIPSS >20 FLOW RATE < 10 RV > 20O ml
- 16. • The term "benign prostatic hyperplasia" is reserved for the histological pattern it describes. • Benign prostatic enlargement is used when there is gland enlargement and is usually a presumptive diagnosis based on the size of the prostate. • Benign prostatic obstruction (BPO) is used when obstruction has been proven by pressure flow studies, or is highly suspected from flow rates and if the gland is enlarged. • Bladder outlet obstruction (BOO) is the generic term for all forms of obstruction to the bladder outlet (e.g., urethral stricture) including BPO.
- 17. BOO • BLADDER OUTLOW OBSTRUCTiON • This is a urodynamic concept based on combination of law of flow rates in presence of high voiding pressure. • Urodynamically proven BOO • BPH • Bladder neck stenosis • Bladder neck hypertropy • Prostrate cancer • Urethral strictures • Functional obstruction due to neuropathic condition(DM,Parkinson’s disease, disseminated sclerosis,Alzheimer’s , Stroke)
- 18. ∙ Little correlation with volume and degree of symptomatology Degree of BOO does not necessarily correlate to the severity of LUTS Long term effect of BOO Bladder may decompensate so that detrusor contraction become progressively less efficient and residual urine develops. Bladder may become more irritable during filling with decrease in functional capacity, partly by detrusor over activity.
- 19. INVESTIGATIONS • Urine Microsopy and C/S • Blood urea serum creatine, serum electrolytes • Cystoscopy • Prostate specific antigen • Acid phosphatase • USG - Look for residual urine, volume • Urodynamics Urine Flow rate > 15ml / sec is normal 10-15ml is equivocal < 10 ml is low Voiding pressure < 60 cm of water is normal 60-80 ml is equivocal > 80 is high Normal peak urine flow rate is > 15 ml/sec., for a voided volume more than 200ml. In obstruction it is < 10 ml/ sec
- 20. • No symptoms specific for early prostatic cancer • Presenting symptoms are therefore those of BPH • BX of prostate should be performed in those with abnl DRE or PSA ABOVE Age specific reference range.
- 21. • Trans-rectal US (TRUS) is useful to find out nodules/ possibility of carcinoma prostate. It is not done routinely. • IVU- to see kidney function
- 22. PSA • Prostate specific antigen • Single chain glycoprotein of 240 AA residue and 4 CHO side chain • Physiological roole in lysis of seminal coagulam • prostate specific, but not cancer specific • In addition to ca pro , it can elevated in • increasing age, • A/c urinary retention • CathetArisation • After TURP, • PROSTATE BX • PROSTATITIS
- 23. PROBLEM WITH PSA • Men with prostate cancer may have a normal PSA • Men with BPH or other benign condition may have a raised psa • Age specific PSA • 40- 49YR OLD -- <2.5 ng/ml • 50- 59 yr - < 3.5 • 60- 69 <4.5 • 70- 79 < 6.5 ng/ml • Free : total PSA ratio ( < 0.15 strongly suggests posssibility of carcinoma prostate)
- 24. MANAGEMENT • Basic management of BPH/LUTS classifies diagnostic tests as either recommended or optional. • A "recommended test" should be performed on every patient during the initial evaluation whereas an "optional test" is a test of proven value in the evaluation of select patients. • If the initial evaluation demonstrates the presence of LUTS associated with results of a digital rectal exam (DRE) suggesting prostate cancer, hematuria, abnormal prostate-specific antigen (PSA) levels, recurrent infection, palpable bladder, history/risk of urethral stricture, and/or a neurological disease raising the likelihood of a primary bladder disorder, the patient should be referred to a urologist for appropriate evaluation before advising treatment
- 25. CONTD • presence of LUTS ,with or without some degree of nonsuspicious prostate enlargement, if the symptoms are not significant or if the patient does not want treatment, no further evaluation is recommended. • In patients with significant symptoms, it is now recognized that LUTS has a number of causes that may occur singly or in combination. Among the most important are BPO, overactive bladder, and nocturnal polyuria. • Discuss the benefits and risks • Treatment Options: watchful waiting, medical, surgical, minimally invasive surgical treatments.
- 26. MEDICAL MANAGEMENT • In drug therapy, if there are coexisting BOO and overactive bladder symptoms –combination of alpha-blocker and anticholinergic therapy. • If BOO symptoms predominate, alpha-adrenergic blocking agents are the first treatment of choice for LUTS due to BPH. • when the prostate is enlarged as assessed by PSA levels, transrectal ultrasound (TRUS) or on DRE, alpha-blockers alone, 5-ARIs alone, and/or combination alpha-blocker and 5-ARI therapy have shown the most efficacy,
- 27. • storage symptoms predominate in an overactive bladder due to idiopathic detrusor overactivity. • The treatment options of lifestyle intervention (fluid intake alteration), behavioral modification and pharmacotherapy (anticholinergic drugs) should be discussed with the patient.
- 28. DRUGS USED IN BPH • Medical Therapies Alpha-Blockers - Alfuzosin, Doxazosin, Tamsulosin, Terazosin, Silodosin* • Inhibits smooth muscle contraction of prostate, they reduce bladder neck resistance so as to improve the urine flow • 5- Alpha-reductase inhibitors (5-ARIs) - Dutasteride, Finasteride • Inhibits conversion of TS to DHT, effective in palpable enlarged prostate . Decrease actual volume of prostate with maximal efect seen by 6 months • This class of drugs also alter serum PSA level(reduce to 50%),must be kept in mind with regard s to prostate cancer screening • Combination Therapy - Alpha blocker and 5-alpha-reductase inhibitor - Alpha blocker and anticholinergics • Anticholinergic Agents
- 29. INDICATION FOR SURGERY Severe obstruction based on urodynamic data .. <10 ml/sec recurrent hematuria Recurrent infection , urinary tract anatomic deterioration from obstruction Chronic retention of urine with residual urine more than 100-250 ml Accute retention with no other cause for retention, accounts for 25% of prostatectomy. Complication of BOO- stones in diverticula
- 30. SURGERY • Minimally Invasive Therapies - Transurethral needle ablation (TUNA) - Transurethral microwave thermotherapy (TUMT) • Surgical Therapies - Transurethral resection of the prostate (TURP) - Open prostatectomy retropubic ((millin) transvesical perineal prostatectomy(young) - Transurethral holmium laser ablation of the prostate (HoLAP) - Transurethral holmium laser enucleation of the prostate (HoLEP) - Holmium laser resection of the prostate (HoLRP) - Photoselective vaporization of the prostate (PVP) - Transurethral incision of the prostate (TUIP) - Transurethral vaporization of the prostate (TUVP)
- 31. PROSTATE RESECTOSCOPE AND TURP
- 32. TURP • Using cystoscope with fluid like 1.5% isotonic glycine irrigating continuously, enlarged prostate is identified and resected using a loop with hand control • Resection is done using high frequency diathermy current, above the level of verumontanum. • After surgery continuous bladder irrigation using three way foley’s catheter • Antibiotic should be given and catheter is removed within 72 hours.
- 33. COMPLICATIONS OF TURP • Water intoxication with CCF- TURP syndrome • Hyponatraemia • Haemorrahage / hematuria(3%) • Infection (15-20%) • Incontinence • Perferation of bladder/ Prostatic capsule • Stricture urethra • Retrograde ejaculation(65%) • Recurrence(15% after 8-10yr) • Erectile dysfunction(5%)
- 34. BENEFITS OF TURP • No suprapubic incision • Most common and popular method • Done using resectoscope • Faster recovery and early discharge.
- 35. HISTOLOGY OF BENIGN PROSTATIC HYPERPLASIA
- 36. CYSTOGRAPHY OF BLADDER BASE ELEVATION INDICATING BPH
- 40. TRANSURETHRAL DILATATION OF PROSTATE
- 41. • a large variety of MITs exist for bph who fails drug therapy , but for most patients the gold standard surgical proceedure remains TURP
- 42. THANK YOU
- 43. TUNA-INDICATIONS • BPH/BOO • Lateral lobe enlargement • Prostate volume <60gms • Median lobe not ideal, but can be Rx • Bladder neck hypertrophy not ideal candidate
- 44. TUMT- METHOD OF ACTION • Apoptosis induced by moderate thermal energy for longer period of time • Hemorrhagic necrosis induced by higher thermal energy over shorter time
Notas do Editor
- This is a sagittal view of the prostate. It is located beneath the bladder. The prostate is separated from the rectum and the bladder by Denonvillier’s fascia, a membranous band of fibrous tissue. Perineal muscle is located directly underneath the prostate. The urethra travels from the bladder through the prostate into the penis.