
Recomendados
Mais conteúdo relacionado
Semelhante a PERICARDIAL TEMPONADE drmousa.pptx
Semelhante a PERICARDIAL TEMPONADE drmousa.pptx (20)
Mais de mousaderhem1
Mais de mousaderhem1 (20)
Último
Último (20)
PERICARDIAL TEMPONADE drmousa.pptx
- 2. ● Overview about topic ○ Definition ○ Pathophysiology ○ Signs and symptoms ○ Treatment ● Patient and Problem ○ History ○ Nursing Physical Assessment ○ Related Treatments ○ Nursing care plan ● References. Outline
- 3. The pericardium is composed of two layers: Visceral pericardium and The parietal layer Normally the pericardial space or sac contains up to 50 ml of serous fluid Pericardium 3
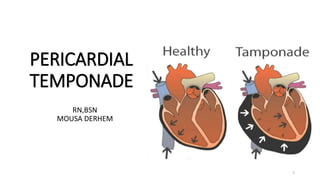
- 4. Cardiac tamponade is a serious medical condition in which blood or fluids fill the space between the sac that encases the heart and the heart muscle. This places extreme pressure on your heart. The pressure prevents the heart’s ventricles from expanding fully and keeps your heart from functioning properly. So the heart can’t pump enough
- 5. • Cardiac tamponade is the accumulation of blood or other fluid in the pericardial sac puts pressure on the heart, which may Prevent it from pumping effectively..
- 6. Pericardial tamponade can develop suddenly as a result • Trauma : both stabbing and blunt • Rupture of the aorta Aortic dissection • Rupture of the ventricle after a heart attack • Post myocardial infarction • complications of Heart surgery (open heart surgery, CABG) • Drugs and medications ( antihypertensives e.g. minoxidil, hydralazine , procainamide) Causes
- 7. Pleural effusion due to various causes exert pressure in heart walls Impairs relaxation and filling of the ventricles Chambers do not fill properly Less cardiac output (too little oxygen reaches the tissues) Increase venous pressure Hypotension, shock , Reflex tachycardia ↑JVP hepatomegaly ascites peripheral edema Rales Systemic Congestion Pulmonary congestion
- 8. • Chest discomfort • Pleuritic pain • Tachypnea and dyspnea on exertion that progresses to air hunger at rest are the key symptoms • Convulsions, unconscious • Most patients are weak and faint at presentation and can have vague symptoms such as anorexia, dysphagia, and cough • The initial symptom may also be one of the complications of tamponade, such as renal failure
- 9. • Elevated venous pressure , Distended neck veins • Kussmaul’s sign{distended neck veins} • Hypotension • Narrow pulse pressure • Dyspnoea • Cyanosis of lips and nails • Restlessness and anxiety • Pain in the right upper abdomen, Upset stomach • Fever, for any infection
- 10. • Beck's triad (cardiology) • Hypotension • Muffled heart sounds • jugular venous distension • Other • Pulsus paradoxus
- 11. • History Collection :- Collect history regarding the etiological factors and symptoms • Physical Examination :-Beck's triad, Pulsus paradoxus (a drop of at least 10 mmHg in arterial blood pressure on inspiration) ,There may also be general signs & symptoms of shock (such as tachycardia , more than 90 beats) per minute breathlessness and decreasing level of consciousness) , Can be bradycardia? (uremia and patients with hypothyroidism) ,Rub is a frequent finding in patients with inflammatory effusions
- 12. Electrocardiographic Findings :- May be associated with ST segment , low voltage QRS complexes , In some cases, electrical alternans will be present in which case the height of the QRS varies from beat to beat , Tachycardia will likely be present as well , Combined P and QRS alternation is virtually specific for tamponade
- 13. • Echocardiogram :-This scan provides a detailed image of the heart, which may help to detect the fluid in the pericardial sac or a collapsed ventricle. • Chest X-ray:- An X-ray of the chest shows if the heart is abnormally large or an unusual shape due to fluid build up..
- 14. • Computerized tomography (CT) scan:- A CT scan of the chest can confirm the presence of extra fluid in the pericardium. • Magnetic resonance angiogram (MRA):- An MRA uses a magnetic field and radio waves to detect any abnormalities in how the blood flows through the blood vessels of the heart.
- 16. The main aim of client with cardiac Tamponade is : 1. Save the patient life 2. improve the heart functions 3. Relive from symptoms Treatment that are administered for cardiac tamponade include: 1. IV fluids to maintain normal BP 2. Antibiotics 3. Supplemental oxygen to reduce work load on the heart
- 17. 4.Bed rest and leg elevation • 5. Inotropic drugs ( Dobutamine) • Mechanical ventilation with positive airway pressure should be avoided in patients with tamponade, because this further decreases cardiac output
- 18. PERICARDIOCENTESIS • Pericardiocentesis, also called a pericardial tap, is a surgical invasive procedure ( use both diagnostic and therapeutic purpose) in which abnormal or excessive fluid is removed from the pericardium sac the sac around your heart. Or Pericardiocentesis is the removal by needle of pericardial fluid from the sac surrounding the heart for diagnostic or therapeutic purposes.
- 19. • Monitor strictly vital signs, especiallyrespiratoryfrequency. • Give the semi-Fowlerposition if not contraindicated. • Give oxygen as indicated • Monitor urine output hourly; a drop in urine output may indicate decreased renal perfusion as a result of decreased stroke volume secondaryto cardiac compression. • Continuously monitor ECG for dysrhythmia formation, which may result of myocardial ischemia secondary to epicardialcoronary artery compression.
- 20. 20 •Case study
- 21. • Monitorthe BP every 5 to 15 minutesduringthe acute phase. • Auscultation of breath soundsand heart sounds.Listen to the murmur. • Maintainbed rest in a comfortableposition duringthe acute period. • Educatethe patientabout the disease conditionand treatment • Educatethe patient about the pericardiocentesis • Encouragethe patient to ask questions
- 22. Patient history A 59-year-old Saudi male referred from the office of cardiologist to our hospital complaining of worsening shortness of breath, weight gain of 6 pounds, leg swelling, and low blood pressures (BP) down to 80/60mmHg for a few weeks. Medical history was significant for hypertension, coronary artery disease, diabetes, and a recent tamponade diagnosed 4 months prior to this hospitalization. Dizziness was his initial complaint in March.
- 23. Physical examination Cardiovascular: tachycardic, regular rhythm, JVD+, Decreased heart sounds, variation in pulse of 12 mmhg during inspiration Pulmonary: Tachypneic, crackles B/L, SOB when lying flat Abdominal: Soft , non-tender to palpation, BS+ Vitals: HR: 130 RR: 22 BP:85/65 Temp: 101.4 F SPO2: 92%
- 24. Diagnosis
- 25. Emergent Treatment 25 1. Oxygen toreduceworkload on the heart 2. Hypotension Medications to help increase blood pressure to normal levels A . IVF cautiously and Dobutamine Vasopressors 3. Cardiac Tamponade A . Pericardiocentesis
- 27. Pulsus paradoxus > 10 mm Hg (hallmark) Narrowed pulse pressure (<30 mm Hg) Hypotension Neurologic Anxiety Confusion Obtunded if decompression is advanced Nursing assessment 27
- 28. ● Ineffective Breathing Pattern related to: hyperventilation that evidenced by shortness of breathing and change vital signs Nursing diagnosis 28 Nursing planning To maintain Patterns breath effectivelyas evidenced by no tachypnea, vital signs are within normal ranges NURSING INTERVENTIONS- 1. Monitorstrictlyvital signs, especiallyrespiratory frequency. 2. Monitorthecontents breathing, chestexpansion, regularity of breathing, mouth breathing and muscleusea respirator 3. Givethesemi-Fowlerposition if notcontraindicated. Rationale: Facilitates lung expansion 4. Teachclientsadeep breath. Rationale: With thedeep breathing exercisecan increase oxygen intake. 5. Giveoxygen as indicated. Rationale: Oxygenadequate toavoid the riskof tissuedamage. 6. Give medicationas indicated. Rationale: Medications thatcan affect therespiratoryventilation.
- 29. NURSING INTERVENTIONS 29 1. Monitorstrictlyvital signs, especiallyrespiratory frequency. 2. Monitor thecontents breathing, chestexpansion, regularity of breathing, mouth breathing and muscle usea respirator 3. Give thesemi-Fowler position if not contraindicated. Rationale: Facilitates lung expansion 4. Teachclientsadeep breath. Rationale: With thedeep breathing exercisecan increase oxygen intake. 5. Giveoxygen as indicated. Rationale: Oxygen adequate toavoid the risk of tissuedamage. 6. Give medication as indicated. Rationale: Medications thatcan affect the respiratoryventilation. NURSING EVALUATION After nursing diagnosis patient partially goal met, patient maintained breathing patterns no tachypnea
- 30. Decreased cardiac output related to reduced ventricular filling secondary to increased intrapericardial pressure. GOALS- To maintain cardiac output of the patient as evidenced by client HR,BP,Pulse pressure NURSING INTERVENTIONS 1. Continuously monitor ECG for dysrhythmia formation 2. Monitor the BP every 5 to 15 minutes during the acute phase. 3. Note the color, presence / quality of the pulse. 4. Auscultation of breath sounds and heart sounds. Listen to the murmur. 5. Maintain bedrest in a comfortable position during the acute period. 6. Provide adequate rest periods / adequate. Assess the form of self-care activities, if indicated. Nursing diagnosis 2 30 NURSING EVALUATION After nursing diagnosis patient is maintained cardiac output
- 31. Educate the patient about the disease condition Educate the patient about the treatment Educate the patient about the pericardiocentesis Encourage the patient to ask questions Health education 31
- 32. 1. Doenges, M. E., Moorhouse, M. F., & Murr, A. C. (2019). Nursing care plans: Guidelines for individualizing client care across the life span. FA Davis. 2. Hinkle, J. L., & Cheever, K. H. (2022). Brunner and Suddarth’s textbook of medical-surgical nursing. Wolters kluwer india Pvt Ltd. 3. Emergency Nurses Association. (2019). Sheehy's Emergency Nursing: Principles and Practice. Elsevier Health Sciences. 4. https://www.ncbi.nlm.nih.gov/books/NBK568727/ References 32