
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Generalrulesofabdomenalexamination 140413161534-phpapp02
Semelhante a Generalrulesofabdomenalexamination 140413161534-phpapp02 (20)
Mais de mostafa hegazy
Mais de mostafa hegazy (20)
Último
Último (20)
Generalrulesofabdomenalexamination 140413161534-phpapp02
- 1. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 1 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION
- 2. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 2 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION GENERAL RULES: • Wash hands / warm them. • Patient should be lying flat. • Keep the room as warm as possible and make sure that the lighting is adequate. • Proceed calmly / don’t make sudden moves. • Approach from right side of the patient. • Gather as much data as possible by observation first. • Arms at side (behind head tightens abdomen) & legs straight. • If the head is flexed, the abdominal musculature becomes tensed and the examination made more difficult • Bending knees may relax abdomen. • Abdomen should be fully exposed. Patient needs to be exposed from above the xiphoid process to the symphysis pubis. Exposure:--- 1. Ask the patientto lie on a level examinationtable that is at a comfortable height for both of you. At this point,the patient shouldbe dressedin a gown and, ifthey wish,underwear. 2. Take a spare bedsheetand drape it over their lowerbody such that it just covers the upper edge of theirunderwear (or so that it crosses the top of the pubic region). This will allow you to fullyexpose the abdomenwhile at the same time permittingthe patientto remain somewhat covered.The gown can then be withdrawn so that the area extendingfromjust belowthe breasts to the pelvicbrim is entirelyuncovered, rememberingthat the superior margin of the abdomenextendsbeneaththe rib cage. Order of Examination • Inspection • Auscultation • Percussion • Palpation
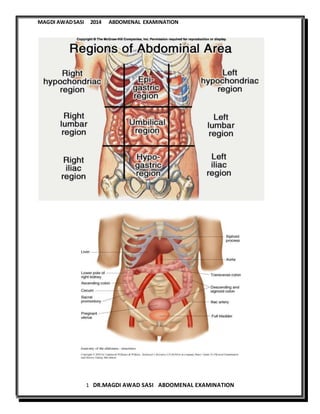
- 3. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 3 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION • Inspection : standing at the foot of the table and looking up towards the patient's head 1. Abdominal contour(Appearance of the abdomen )-Shape=contour: Is it flat? Distended? If enlarged, does this appear symmetric or are there distinct protrusions, perhaps linked to underlying organomegaly? The contours of the abdomen can be best appreciated by standing at the foot of the table and looking up towards the patient's head. Global abdominal enlargement is usually caused by air, fluid, or fat. It is frequently impossible to distinguish between these entities on the basis of observation alone, distended with full flanks. 5F are the causes of abdominal distentión— fat, feces ,flatus ,feotus , fluid. 2. Abdominal skin --Scars , striae (purple or silver), dilated veins around umbilicus in caput medusa veins radiating from the umbilicus & its direction of flow: from below upward or vise versa ((portal hypertension)) and veins in the lateral parts of abdomen (( inferiorvena cava obstruction)) ,rashes and lesions, Peristalsis (visible--Visible loops of bowel) ,Pulsations (Aorta). The abdomen is divided into 9 quadrants by two vertical midclavicular lines and two horizontal lines—one through transpylorus and the other through the anterior iliac spine. Common scars: 1. Right subcostal scar---- cholycestectomy scar 2. Mid –line long lapratomy scar---- acute abdomen of surgical unknown cause
- 4. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 4 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION 3. Right or Left lumbar scar---- kidney surgical intervention 4. Suprapubic scar---- Caesarean scar or prostate operation or pelvic operation. 5. Mid line supra umbilical scar—duodenal ulcers , pancreatic operations.
- 5. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 5 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION 3. Respiratory movement : Male --- abdomino-thoracic-- manner of breathing is abdominal respiration. Female –thoraco-abdominal-- the manner of breathing is thoracic respiration. 4. Umbilicus central or pushed down , inverted or flat or everted. The flat umbilicusisa clue to the ascitis or organomegallydue to increase intraabdominal presure. Look for discoloration over the umbilicus: 1. Cullen’s Sign: discoloration over the umbilicus. 2. Grey Turner’s Sign: discoloration over the flanks. These are both late signs suggesting intra-abdominal bleeding.
- 6. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 6 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION SUMMARY: INSPECTION Shape of the abdomen and flanks Skin –scar ,striae ,prominent veins ,umbilicus , visible peristalsis Movements of abdominal wall with respiration Ask the patient to cough and look for hernial orifices Hernia is derived from the Latin for "rupture" It is the protrusion of an organ or part of an organ through a defecte in the wall of the cavity ((peritoneal lining ))normally containing it. Types of herniae: Inguinal (( Indirect or indirect )) Inguinal hernias can be direct which is herniation through an area of muscle weakness, in the inguinal canal, and inguinal hernias indirect herniation through the inguinal ring. Indirect hernias, the more common form, can develop at any age but are especially prevalent in infants younger than age . This form is three times more common in males. Femoral Herniation through the femoral canal . Incisional Herniation ------- through an area weakened by a scar Umbilical Paraumbilical --------- Acquired defect above or below the umbilicus Epigastric --- in the midline of abdomen above the umbilicus caused by a defect in linea alba. If there is a visible mass or herniae , you have to asses the : Size Site Surface Shape Affect of cough
- 7. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 7 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION Palpation: Kneel down Ask about site of abdomenal pain First warm your hands by rubbing them together before placing them on the patient. The pads and tips (the most sensitive areas) of the index, middle, and ring fingers are the examining surfaces used to locate the edges of the liver and spleen as well as the deeper structures. You may use either your right hand alone or both hands, with the left resting on top of the right.put the palm of your right hand over abdomen and flexes your hand frequently at metacarpophalangeal and interphalangeal joints. Apply slow, steady pressure, avoiding any rapid/sharp movements that are likely to startle the patient or cause discomfort. Examine each quadrant separately, imagining what structures lie beneath your hands and what you might expect to feel. A. SUPERFICIAL PALPATION: Aim – to get confidence and assurance , to check temperature ,tenderness. Palpate the abdomen to detect: 1. Tenderness 2.Muscular rigidity or Rigidity 3.Superficial organs and masses Before you begin palpation, ask your patient if he has any pain or tenderness , and be away from the area of the pain . Palpate that area last, using gentle pressure. Start your palpation by the palm of the right hand from the right iliac fossa and go anti-clock wise . From RIF to suprapubic – left iliac fossa –left lumbar---- left hypochondrial --- epigastric -----right hypochondrial----right lumbar.. Press down around 1 cm Light palpation by moving your hand slowly and just lifting it off the skin. Watch for patient’s face for signs of discomfort. Abdominal pain upon light palpation suggests peritoneal irritation or inflammation
- 8. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 8 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION If rigidity or guarding while palpating, determine whether it is voluntary (patient anticipates the pain) or involuntary (peritoneal inflammation) Assess for rebound tenderness by pushing slowly and then releasing your hand quickly off the tender area. Watch for patient’s face for signs of discomfort. Identify any masses and note: Size,Location,Contour,Tenderness,Pulsations,Mobility DEEP PALPATION: For the organs and masses. A deeper exam is performed with the right hand or two hands, one on top of the other again flexing at the MCP & IPJ joints. You should still be looking at the patient’s face for them flinching due to pain. Again, examine all 9 named segments of the abdomen. Liver is located under right upper quadant and if the liver enlarged or pushed it descend toward the right iliac fossa along the mid calvicular line. In general, it is easier to detect abnormality if you start in an area that you're sure is normal by comparison. The right iliac fossa is the starting point for superficial and deep palpation. Directionof enlargementoforgans Liver: Enlargestowards right lowerquadrant Spleen:Diagonallytowards right lower quadrant Reactions that may indicate pathology include: Guarding,describingmuscle contraction as pressure isapplied. Rigidity,indicatingperitoneal inflammation.
- 9. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 9 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION Rebound,pain on release Hernial orificesifpositive coughimpulses. Start by kneelingdownto be on the same level ofpatientsabdomen. Start the deeppalpationby putting your right hand (palm) over the abdomenof the patient. start from right iliacfossa and ascend through mid clavicular line toward right hypochondrial area . keepyour palm in touch with the patientsabdomen. One way…..Gentlypushdown (posterior) and towards the patient's head with your hand oriented roughly parallel to the rectus muscle or lower right costal margin, allowingthe greatest numberof fingersto be involvedinthe exam as you try to feel the edge ofthe liver.Advance your hands a fewcm cepheladand repeat until ultimatelyyou are at the bottom margin of the ribs. Pushingup and inwhile the patient takes a deepbreath may make it easier to feel the liveredge as the downward movementof the diaphragm will bring the livertowards your hand. The tip of the xyphoidprocess, the bony structure at the bottom endof the sternum,may be directed outward or inward and can be mistaken for an abdominal mass. You shouldbe able to distinguishit by noting its locationrelative to the rib cage (i.e.in the mid-line where the right and leftsidesmeet). The two handed method may be used. Begin at the right lower quadrant and examine the entire abdomen gently by deep palpation. Lay one hand over the abdomen and push with the second concentrating on the feel of the bottom hand. Once again, known tender areas should be palpated last. 130-131: Palpation of Liver: Alternative Method It is acceptable during palpation of the liver to use both hands to palpate abdomen. You use the fingers of one hand to palpate and the other hand is used to apply pressure to the dorsum of the other hand. Thus the hand you are using to palpate does not need to be used to apply pressure.
- 10. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 10 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION Usual way----- 1.Start from right iliac fossa with your hand( palm ) parallel to the right costal margin 2.Ask the patient to take deep breath while keeping your hand in touch 3.Ask the patient to exhale , palpate deeply 4 cm in as the abdomen become relaxed 4.Preecedtoward the right costal margin through midclavicular line 5. During expiration, palpate deep. During inspiration, moves toward RT costal margin till you fell the liver margin where you have to ask the patient to take deep breath and go deeply with your hand 4cm depth. This is because the liver is intraperitoneal and moves down with inspiration. For spleen: The Palpation of the spleen is as for the liver but in the direction of the left hypochondrium. The edge of the spleen which may be felt if distended is more nodular than the liver. The normal spleen in not palpable. When enlarged, it tends to grow towards the pelvis and the umbilicus (i.e. both down and across) Another way to assess for splenomegaly is to ask the patient to lie on their right side. Support the rib cage with your left hand and again ask the patient to take deep breaths in moving your right hand up towards the left hypochondrium. Spleen (if not palpable, R lateral decubitus)--- The edge, when palpable, is soft, rounded, and rather superficial Palpation: Liver Stand on the pt’s right side. Place your left hand behind the patient’s R side under the 11th and 12th rib area. Press upward with the L hand. Place your R hand on the pt’s abdomen well below where you percussed the liver edge
- 11. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 11 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION To feel for the kidneys you should place one hand under the patientin the flank region((righthand at the inferior and lateral border of the ribs))and the other handon top. ---pushingdown as you push up from behind with your left hand.-----You should then try to ballot the kidney between the two hands. In the majority of people the kidneys are notpalpable, butthey may be in thin patients who have no renal pathology. Note: If the liverispalpable , it may be pusheddownor enlarged.Liverspan isthe nextstep to be done. If the spleenispalpable , it is enlarged. If the liverispalpable , it isimportant to detectthe tenderness--- hepatitis orcongestion, the size belowthe costal margin(cm) ,consistency—firmorhard, edge ,surface regularity---nodular / irregular inmalignancy or secondaries ,pulsatile – tricuspid regurgitation. You can also try to "hook" the edge of the liverwith your fingers. To utilize this technique,flexthe tipsof the fingersof your right hand (claw-like).Thenpushdown in the right upper quadrant and pull upwards (towards the patient'shead) as you try to rake-upon the edge of the liver.This isa nice way of confirmingthe presence ofa palpable liveredge feltduring conventional examination.
- 12. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 12 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION Causes of hepatomegally: 1. Infections--- hepatitis – HAV , HBV ,HCV, EBV, CMV , TB abscess , malaria ,alcohol 2. Inflammtion ---- autoimmune hepatitis 3. Ischemia----- bubb chiari syndrome , congested liver ,hepatic vein thrombosis 4. Tumour ---- hepaoma , lymphoma , leukemia 5. Tumour 2ry--- metastases 6. TB------ abscess 7. Fatty liver Causesof splenomegally( huge): 4 fingersbelow costal margin14cm 1. Malaria 2. Leishmaniasis 3. CML--- chronic myeloidleukemia 4. CLL----chroniclymphocyticleukemia 5. Portal hypertension---- livercirrhosisisthe commonest. 6. Myelofibrosis Causes of mildsplenomegally: 1. 1.Infection --- HAV ,glandularfever, EBV , CMV, infective endocarditis,malaria,leishmaniasis 2. Inflammation---- SLE,Rhemtaoidarthritis,sarcoidosis 3. Ischemia----- portal veinthrombosis 4. Tumour---- lymphoma,leukemia 5. Tuberculosis --- military 6. Portal hypertension How can you differentiate splenomegally from enlarged kidney on the left side of abdomen? For splenomegally , 1. Direction of enlargement ----- toward the right iliac fossa towardthe midline 2. Continuity of the dullness on percussion note 3. Movement with deep breathing as it is intraperitoneal 4. Splenic notch over the medial site 5. The examiner cant insert the fingers below the left costal margin For the kidney, 1. Ballottement is the pathognomic sign 2. Area of resonance over the mass PERCUSSION: Helps to identify the amount & distribution of gas and to identify possible masses that are solid or fluid filled. Percussing the abdomen produces different sounds based on the underlying tissues. Sounds help you detect excessive gas and solid or fluid-filled masses Also help you determine the size and position of solid organs such as the liver and spleen.
- 13. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 13 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION By Percussion , you are looking for areas of tympany and dullness Expect to hear tympany in most of the abdomen Expect dullness over the solid abdominal organs such as the liver and spleen Can be used to assess size of liver and spleen On the right, it is the liver dullness; on the left, dullness of the spleen, kidney ,colonic mass. The liver span is estimated by percussion. Remember that it is easier to hear the change from resonance to dullness – so proceed with percussion from areas of resonance to areas of dullness. 1.upper border from 2nd intercostal space through mid clavicular line, start percussing on the chest moving down towards the abdomen about ½ to 1 cm at a time. Note where the percussion notes change from resonate to dull which is the beginning of the liver border((upper)). 2.lower border from right iliac fossa though midclavicular line and ascend towardcostal margin till the dullness note start which is the beginning of the liver border(( lower)). Liver span is normally 6 to 12 cm in the midclavicular line which is the distance betweenupper and lower borders. For spleen, • When a spleen enlarges, it expands downward and medially toward the right iliac fossa and pushed the umbilicus to be flat . Fullness in the left hypochondrial may be the first clue of spleenomegally. Spleen enlargement replaces the tympany of the stomach with the dullness of a solid organ • Percussion cannot confirm splenic enlargement, but it can raise your suspicion. • There are two techniques to percuss splenic enlargement. • Percuss the left lower anterior chest wall betweenlung resonance (6 IC) above & the costal margin (an area termedTraube’s space) • As you percuss laterally, note the extent of the tympany; if tympany is prominent laterally, splenomegaly is unlikely. • Can also check for a splenicpercussionsign • Percussthe lowestinterspace in the leftanterior axillaryline;the area is usuallytympanitic • Then ask the patientto take a deepbreath and percuss again
- 14. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 14 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION • Whenthe spleenisnormal, the space usuallyremains tympanitic ASCITES • Shifting Dullness • Percuss centrally from the epigstrium to umbilicus then to each flank • Locate point of change on side • Ask patient to roll towards you • Wait….for a minute for fluid to move to other side • Percuss again ?area of dullness moved • Fluid Thrill – Use patients right hand in midline – Flick one side and feel the other side – This is done if the patient has huge abdomen which is tense and difficult to palpate and there is no area of central resonance for comparison and for fluid to move from side to another.
- 15. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 15 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION What are the causes of ascitis? As apart of generalised cause (( with bilateral pitting pedal odema )) 1. Portal hypertesion—liver cirrhosis 2. Chronic renal failure 3. Nephrotic syndrome 4. Hypothyrodism 5. Congestive heart failure 6. Protein losing enteropathy As a part of local abdomenal disease, 1. Tuberculosis 2. GIT tumours--- stomach ,colon , pancrease 3. Metastases to the peritoneum 4. Connective tissues diseases 5. Budd chiari syndrome 6. Acute pancreatitis
- 16. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 16 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION AUSCULTATION: • Provides important information about bowel motility: decreased motility suggests peritonitis; increased motility suggests obstruction • Need to listen before percussion or palpation since these maneuvers may alter the frequency of bowel sounds • Can also appreciate BRUITS over the aorta or other arteries, suggesting narrowing of the arteries from atherosclerosis Bruits are high pitched sounds due to obstruction to flow due to narrowing (stenosis) of arteries Listen midline (bruit in aorta) Right / left upper quadrant (renal artery bruits) • Listen with diaphragm of stethoscope • Normal sounds occurs every 5-10 seconds & consist of clicks and gurgles • Need to listen for 2 minutes to declare no bowel sounds; since bowel sounds are widely transmitted, need only to listen in one spot • Occasionally hear borborygmi - long, prolonged gurgles of hyperperistalsis - the familiar stomach growling SUMMARY PONTS: 1. BOWEL SOUNDS a. ABSENT b. LOUD 2. VENOUS HUMS a. B/W XIPHISTERNUM AND UMBILICUS 3. Renal Bruit 4. Hepatic Bruit
- 17. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 17 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION • Succussion Splash • Puddle Sign • Cover the patient up • Turn to the examiner “ I wouldlike to complete myexaminationby examiningthe external genitalia, performing a digital rectal examination and dipstick the urine.” You can ellicit succussion splash in normals following ingestion of aerated drink. Whenever there is air and fluid inside a bowel you can ellicit this sign. NOTE: Special manevures may also be performed, to elicit signs of specific diseases.These include Gallbladder: Murphy's sign It is performed by asking the patient to breathe out and then gently placing the hand below the costal margin on the right side atthe mid-clavicular line (the approximate location of the gallbladder).The patient is then instructed to inspire (breathe in).Normally,during inspiration,the abdominal contents are pushed downward as the diaphragm moves down.If the patient stops breathing in (as the gallbladder is tender and,in moving downward,comes in contactwith the examiner's fingers) and winces with a 'catch' in breath, the test is considered positive.In the elderly the sensitivity is markedly lower; a negative Murphy's sign in an elderly person is not useful for ruling out cholecystitis if other tests and the clinical history suggest the diagnosis • Courvoisier'slaw: States that in the presence of an enlarged gallbladder which is non tender and accompanied with mild jaundice, the cause is unlikely to be gallstones. Usually, the term is used to describe the physical examination finding of the right-upper quadrant of the abdomen. This sign implicated possible malignancy of the gall bladder or pancreas and the swelling is unlikely due to gallstones(( because gallstones are formed over an extended period of time, resulting in a shrunken, fibrotic gall bladder which does not distend easily)). This shrunken gallbladder is less likely to be palpable on exam. In contrast, the gallbladder is more often enlarged (and more easily palpated) in pathologies that cause obstruction of the biliary tree over a shorter period of time such as pancreatic malignancy leading to passive distention from back pressure. Note that a palpable tender gallbladder may be seen in acute acalculous cholecystitis, which commonly follows trauma or ischemia and causes acute inflammation of the gallbladder in the absence of gallstones. The exceptions to the law are stones that dislodge and acutely jam the ductdistally to the hepatic/cystic duct junction: 1. Gallstone falling and blocking the Ampulla of Vater 2. Gallstone falling and blocking the cystic/hepatic duct junction .The psoas sign: is a medical sign thatindicates irritation to the iliopsoas groupof hip flexors in the abdomen, and consequently indicates that the inflamedappendix is retrocaecal in orientation (as the iliopsoas muscle is retroperitoneal). It is elicited by performing the psoastest by passively extendingthe thighof a patientlying on his side withknees extended, or askingthe patientto actively flex his thighat the hip. If abdominal pain results, it is a "positive psoas sign". In particular, the right iliopsoas muscle lies under the appendix whenthe patient is supine, so a positive psoas signon the
- 18. MAGDI AWADSASI 2014 ABDOMENAL EXAMINATION 18 DR.MAGDI AWAD SASI ABDOMENAL EXAMINATION right may suggest appendicitis. A positive psoas sign may alsobe presentin a patient with a psoas abscess. It may also be positive withother sources of retroperitoneal irritation, e.g.as causedby hemorrhage of an iliac vessel. .Blumberg's sign is a sign that is elicitedduringphysical examinationin medicine. It is indicative of peritonitis. The abdominal wall is compressedslowly and thenrapidly released. A positive signis indicated by presence of pain upon removal of pressure on the abdominal wall. It is very similar to rebound tenderness Appendicitis or peritonitis: Psoas sign - pain when tensing the psoas muscle Obturator sign - pain when tensing the obturator muscle Rovsing's sign - pain in the right iliac fossa on palpation of the left side of the abdomen Carnett's sign - pain when tensing the abdominal wall muscles Patafio's sign - pain when the patient is askedto cough whilst tensing the psoas muscle Cough test - pain when the patient is askedto cough Suspected Pyelonephritis: Murphy's punch sign Hepatomegaly: Liver scratchtest Ascites: bulging flanks, fluid wave test, shifting dullness IF THE PATIENT HAS A HUGE ASCITIS , WHAT IS THE COMMONEST CAUSE AND WHAT OTHER SIGNS YOU HAVE TO LOOK FOR? Liver cirrhosis with portal HTN is the commonest cause. The signs that you have to look for are the stigmata of chronic liver disease. They are: Jaundice , spider neavi , Gyanecomastia in male & Breast atrophy in female , flapping tremors ,palmer erythema , muscle wasting , kilonychia ,leuchonychia , ecchymosis , pedal odema. Those are mandatory to look for in any case of abdominal examination. THANKS MAGDI AWAD SASI HOPPING , IT WILL HELP AND ALLAH ACCEPT MY TRIAL TO HELP OTHERS