
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a antimuscarnic drug
Semelhante a antimuscarnic drug (20)
Mais de Islam Home
Último
Último (20)
antimuscarnic drug
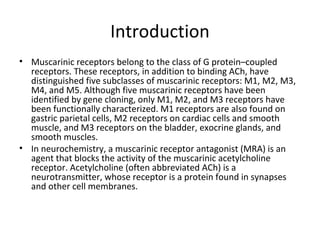
- 1. Introduction • Muscarinic receptors belong to the class of G protein–coupled receptors. These receptors, in addition to binding ACh, have distinguished five subclasses of muscarinic receptors: M1, M2, M3, M4, and M5. Although five muscarinic receptors have been identified by gene cloning, only M1, M2, and M3 receptors have been functionally characterized. M1 receptors are also found on gastric parietal cells, M2 receptors on cardiac cells and smooth muscle, and M3 receptors on the bladder, exocrine glands, and smooth muscles. • In neurochemistry, a muscarinic receptor antagonist (MRA) is an agent that blocks the activity of the muscarinic acetylcholine receptor. Acetylcholine (often abbreviated ACh) is a neurotransmitter, whose receptor is a protein found in synapses and other cell membranes.
- 2. Antimuscarinic drugs cosist of:- • 1- Aropine (ISOPTO ATROPINE) • 2- scopolamine(SOPTO HYOSCINE, SCOPACE) • 3-Benztropine (COGENTIN) • 4-Cyclopentolate (AK-PENTOLATE, CYCLOGYL) • 5-Darifenacin (ENABLEX) 6-Fesoterodine ( TOVIAZ) • 7-Ipratropium (ATROVENT) 8-Oxybutynin (DITROPAN, GELNIQUE) • 9- Solifenacin (VESICARE) 10-Tiotropium (SPIRIVA HANDIHALER) • 11-Tolterodine( DETROL) 12-Trihexyphenidyl (ARTANE) • 13-Tropicamide (MYDRIACYL, TROPICACYL) • 14- Trospium chloride (SANCTURA) •
- 3. Pharmacokinetics of Atropine • Atropine is the prototypical nonselective muscarinic blocker. This alkaloid is found in Atropa belladonna and many other plants. Because it is a tertiary amine, atropine is relatively lipid-soluble and readily crosses membrane barriers. The drug is well distributed into the CNS and other organs and is eliminated partially by metabolism in the liver and partially unchanged in the urine. The elimination half-life is approximately 2 h, and the duration of action of normal doses is 4–8 h except in the eye, where effects last for 72 h or longer.
- 4. Pharmacokinetics of Other Muscarinic Blockers • In ophthalmology, topical activity (the ability to enter the eye after conjunctival administration) and duration of action are important in determining the usefulness of several antimuscarinic drugs (see Clinical Uses). Similar ability to cross lipid barriers is essential for the agents used in parkinsonism. In contrast, the drugs used for their antisecretory or antispastic actions in the gut, bladder, and bronchi are often selected for minimum CNS activity; these drugs may incorporate quaternary amine groups to limit penetration through the blood- brain barrier.
- 5. Mechanism of Action • The muscarinic blocking agents act like competitive (surmountable) pharmacologic antagonists; their blocking effects can be overcome by increased concentrations of muscarinic agonists.
- 6. Effects • The peripheral actions of muscarinic blockers are mostly predictable effects derived from cholinoceptor blockade .These include the ocular, gastrointestinal, genitourinary, and secretory effects. The CNS effects are less predictable. CNS effects seen at therapeutic concentrations include sedation, reduction of motion sickness, and, as previously noted, reduction of some of the signs of parkinsonism. Cardiovascular effects at therapeutic doses include an initial slowing of heart rate caused by central or presynaptic vagal effects followed by the tachycardia and decreased atrioventricular conduction time that would be predicted from peripheral vagal blockade.
- 8. Clinical Uses • The muscarinic blockers have several useful therapeutic applications in the CNS, eye, bronchi, gut, and urinary bladder. CNS Scopolamine is standard therapy for motion sickness; it is one of the most effective agents available for this condition. A transdermal patch formulation is available. Benztropine, biperiden, and trihexyphenidyl are representative of several antimuscarinic agents used in parkinsonism. Although not as effective as levodopa ,these agents may be useful as adjuncts or when patients become unresponsive to levodopa. Benztropine is sometimes used parenterally to treat acute dystonias caused by antipsychotic medications.
- 9. Eye • Antimuscarinic drugs are used to cause mydriasis, as indicated by the origin of the name belladonna ("beautiful lady") from the ancient cosmetic use of extracts of the Atropa belladonna plant to dilate the pupils. They also cause cycloplegia and paralyze accommodation. In descending order of duration of action, these drugs are atropine (>72 h), homatropine (24 h), cyclopentolate (2–12 h), and tropicamide (0.5–4 h). These agents are all well absorbed from the conjunctival sac into the eye. Bronchi • Parenteral atropine has long been used to reduce airway secretions during general anesthesia. Ipratropium is a quaternary antimuscarinic agent used by inhalation to promote bronchodilation in asthma and chronic obstructive pulmonary disease (COPD). Although not as efficacious as agonists, ipra-tropium is less likely to cause tachycardia and cardiac arrhythmias in sensitive patients. It has very few antimuscarinic effects outside the lungs because it is poorly absorbed and rapidly metabolized. Tiotropium is a newer analog with a longer duration of action.
- 10. Gut • Atropine, methscopolamine, and propantheline were used in the past to reduce acid secretion in acid-peptic disease, but are now obsolete for this indication because they are not as effective as H2 blockers and proton pump inhibitors ,and they cause far more frequent and severe adverse effects. The M1-selective inhibitor pirenzepine is available in Europe for the treatment of peptic ulcer. Muscarinic blockers can also be used to reduce cramping and hypermotility in transient diarrheas, but drugs such as diphenoxylate and loperamide are more effective.
- 11. Bladder • Oxybutynin, tolterodine, or similar agents may be used to reduce urgency in mild cystitis and to reduce bladder spasms after urologic surgery. Tolterodine, darifenacin, solifenacin, and fesoterodine are promoted for the treatment of stress incontinence. Toxicity • A traditional mnemonic for atropine toxicity is "Dry as a bone, red as a beet, mad as a hatter." This description reflects both predictable antimuscarinic effects and some unpredictable actions.
- 12. Predictable Toxicities • Antimuscarinic actions lead to several important and potentially dangerous effects. Blockade of thermoregulatory sweating may result in hyperthermia or "atropine fever." This is the most dangerous effect of the antimuscarinic drugs in children and is potentially lethal in infants. Atropine toxicity is described as feeling "dry as a bone" because sweating, salivation, and lacrimation are all significantly reduced or stopped. Moderate tachycardia is common, and severe tachycardia or arrhythmias are common with large overdoses. In the elderly, important additional targets of toxicity include the eye (acute angle-closure glaucoma may occur) and the bladder (urinary retention is possible, especially in men with prostatic hyperplasia). Constipation and blurred vision are common adverse effects in all age groups.
- 13. Other Toxicities Toxicities not predictable from peripheral autonomic actions include the following. CNS Effects •CNS toxicity includes sedation, amnesia, and delirium or hallucinations ("mad as a hatter"); convulsions may also occur. Central muscarinic receptors are probably involved. Other drug groups with antimuscarinic effects, for example, tricyclic antidepressants, may cause hallucinations or delirium in the elderly, who are especially susceptible to antimuscarinic toxicity.
- 14. Cardiovascular Effects • At very high doses, intraventricular conduction may be blocked; this action is probably not mediated by muscarinic blockade and is difficult to treat. Dilation of the cutaneous vessels of the arms, head, neck, and trunk also occurs at these doses; the resulting "atropine flush" ("red as a beet") may be diagnostic of overdose with these drugs. The mechanism is unknown.
- 15. Contraindications • The antimuscarinic agents should be used cautiously in infants because of the danger of hyperthermia. The drugs are relatively contraindicated in persons with glaucoma, especially the closed-angle form, and in men with prostatic hyperplasia.