Gait disorders
•Transferir como PPTX, PDF•
47 gostaram•8,616 visualizações

gait and disorders

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Gait disorders
Semelhante a Gait disorders (20)
Mais de Manideep Malaka
Mais de Manideep Malaka (17)
Último
Último (20)
Gait disorders
- 2. Introduction The maintenance of an upright posture and the act of walking are among the first, and ultimately most complex, motor skills humans acquire. individual’s pattern of walking may be so distinctive they can be recognized by the characteristics of their gait or even the sound of their steps. Many diseases of the nervous system are identified by the disturbances of gait and posture.
- 3. Anatomical aspects of gait 2 basic systems responsible for equilibrium and locomotion 1. Brainstem locomotor centers pedunculopontine & adjacent nuclei of midbrain 2. Spinal locomotor centers Additional level of supraspinal control is needed to maintain bipedal stance and gait 1. Frontal cortex 2. Parietal cortex 3. cerebellum
- 4. Brainstem locomotor centers: Projects from the pontomedullary reticular formation, through reticulospinal pathways into ventromedial spinal cord. Stimulation results in increase in axial and limb muscle tone to assume an upright posture before stepping begins Spinal locomotor centers: Assemblies of spinal interneurons Activate motor neurons of limb and trunk muscles in a patterned and repetitive manner to drive stepping movements propriospinal networks that link the trunk and limbs to facilitate synergic coordinated limb and trunk movements of
- 5. Frontal cortex prefrontal cortex ◦ via corticobulbar and corticostriatal tracts ◦ modulates midbrain and cerebellar locomotor regions. Frontal motor projections to the pontomedullary reticular formation ◦ innervate axial muscles modulate postural responses associated with stepping to the spinal motor neurons, ◦ enables precision of foot movements.
- 6. Parietal cortex It integrates sensory inputs indicates position and orientation in space, the relationship to gravitational forces, Cerebellum Modulates the rate,rhythm,amplitude and force of stepping contributes to medial brainstem efferent system through projections from flocculonodular and anterior lobes ◦ Controlls the equilibrium and truncal posture
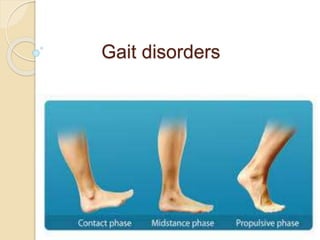
- 7. PHYSIOLOGICAL ASPECTS OF GAIT Stability when standing is based on ◦ musculoskeletal linkages between the trunk and legs ◦ neurological control detecting and correcting body sway i.e, postural responses. Synergitic action axial and proximal limb muscle and postural responses maintain static postural control.
- 8. Postural reflexes: 2 types ◦ anticipatory postural reflexes: feed-forward occurring before limb movement. ◦ Reactive postural reflexes: feedback postural adjustments counteracting body perturbations during movement. ◦ modified by voluntary control. ◦ generated by the integration of visual, vestibular, and proprioceptive inputs in the context of voluntary intent.
- 9. Once the trunk is upright and stable, locomotion can begin. The initiation of gait is heralded by a series of shifts in the center of pressure beneath the feet. ◦ first posteriorly, ◦ then laterally toward the stepping foot ◦ finally toward the stance foot to allow the stepping foot to swing forward This sequence is then followed by the stereotyped stance, swing, and step phases of the gait cycle.
- 10. GAIT CYCLE Period between two successive points at which the heel of the same foot strikes the ground Cadence:“the rhythm and number of steps per minute”
- 11. Gait cycle 2 phases 8 events Phases stance swing Events 4 stance phase events 4 swing phase events
- 12. Stance phase Swing phase Accounts for 60% gait cycle. Consists of 4 phases initial contact loading mid-stance terminal stance. Accounts for 40% gait cycle. Consists of 4 phases Preswing Initial swing Mid swing Terminal swing
- 13. Events during stance phase 1. Heel strike: initiates gait cycle body’s center of gravity is at its lowest position 2. Foot flat : plantar surface of the foot touches the ground 3. Mid stance Swinging contra lateral foot passes the stance foot Center of gravity at its highest position 4. Heel off Heel looses contact with ground. 5. Toe off terminates the stance phase as foot leaves the ground
- 14. Events during swing phase 1. Acceleration: begins as soon as foot leaves the ground activation of hip flexors to accelerate leg forward 2. Mid swing: foot passes directly beneath the body coincident with mid stance of other foot 3. Deceleration: describes the action of muscles as they slow the leg and stabilize the foot in preparation for next heel strike
- 16. Distance measures: Stride length ◦ distance between heels from one heel strike to the next heel strike on same side ◦ distance travelled by a person during a gait cycle Step length ◦ length between heel strike of one foot to other ◦ Rt + Lt step length = stride length Step width ◦ medio lateral distance between feet
- 17. A typical adult walking parameters comfortably on a level surface includes: ◦ velocity of about 80 m per minute, ◦ about 113 steps per minute, ◦ stride length of 1.41 m. ◦ About 60% of the gait cycle is spent in stance phase ◦ 40% in swing phase ◦ 10% in double limb support. The body's center of mass is located just anterior to the S2 vertebral body.
- 19. HISTORY A detailed history provides the first clues to diagnosis. note the circumstances in which walking difficulty occurs. Ask for any associated symptoms, especially falls. Walking over uneven ground exacerbates most walking difficulties. Often an individual is unaware of their gait abnormality, and family or friends note altered cadence, shuffling or slowness.
- 20. Weakness: weakness of certain muscle groups produces characteristic difficulties during particular movements of the gait cycle. ◦ weakness of ankle dorsiflexion - foot drop ◦ Weakness of knee extension - buckling attacks ◦ Weakness of ankle plantar flexion - shallow stepped gait. ◦ ◦ proximal muscle weakness - Difficulty in climbing stairs or rising from a seated position Catching or scraping a toe on the ground and a
- 21. Slowness and Stiffness: Slowness of gait is normal reaction when walking on slippery surfaces. Similarly, when the balance was threatened any musculoskeletal or neurological disorder patient will have slowness of gait. In Parkinson disease (PD) and other basal ganglia diseases, slowness of walking is due to shuffling with short, shallow steps. Difficulty rising from a chair or turning in bed may be clues to loss of truncal mobility in diffuse cerebro vascular disease, hydrocephalus, and basal ganglia diseases.
- 22. Complaints of stiffness, heaviness in the limbs are the symptoms of a spasticity. It is important to remember that leg muscle tone in some upper motor neuron syndromes and dystonia may be normal when the patient is examined in the supine position but is increased during walking. In childhood, an action dystonia of the foot is a common initial symptom, walking on the toes only becoming evident after walking or running.
- 23. Imbalance: poor balance and unsteadiness are cardinal features of cerebellar ataxia and sensory ataxia. cerebellar gait ataxia complains of ◦ Unsteadiness and inability to walk in a straight line and near falls. ◦ Turning and suddenly changing direction results in veering to one side. ◦ Symptoms are exacerbated by an uneven support surface.
- 24. Sensory ataxia: ◦ presents with unsteadiness when walking in the dark. ◦ Patients complain of being uncertain of the exact position of their feet when walking. ◦ impression of walking on a spongy surface or cotton wool. Acute vestibulopathy: ◦ Is associated with vertigo and severe imbalance. Chronic vestibular dysfunction ◦ often causes veering and problems in an environment with many moving objects.
- 25. A wide-based unsteady gait also is a feature of frontal lobe diseases ◦ normal pressure hydrocephalus, ◦ diffuse small vessel ischemia of frontal sub cortical white matter. Imbalance in sub cortical cerebro vascular disease commonly manifests when ◦ turning while walking, ◦ stepping backwards, ◦ bending over to pick up something.
- 26. Falls: Toppling Falls ◦ muscle tone is retained ◦ falling like a tree trunk ◦ due to impaired static and dynamic postural responses that control body equilibrium collapsing falls ◦ muscle tone is lost ◦ imply a loss of consciousness characteristic of syncope or seizures Tripping falls: ◦ many people attribute falls to tripping when in fact tripping did not occur. ◦ Tripping may be due to foot drop or shallow steps ◦ also be a consequence of secondary to inattention, dementia, or poor vision.
- 27. Proximal muscle weakness may result in the legs giving way and falls. Unsteadiness and poor balance in an ataxic syndrome may lead to falls. falls associated with postural adjustments, or falls occurring when performing multiple tasks suggest an impairment of postural responses. Backward falls in early stages ◦ Feature of an akinetic-rigid syndromes ◦ Favors a diagnosis of MSA or PSP rather than PD ◦ Falls do occur in PD but are late feature. • In PD falls are usually forward and may also occur while turning and changing the posture. Collapsing falls related to orthostatic hypotension, a
- 28. Sensory Symptoms and Pain: distribution of sensory complaints provides a clue to the site of the lesion. ◦ Ex: Distal symmetrical paresthesias of limbs S/O peripheral neuropathy. Skeletal pain due to degenerative joint disease is aggravated by movement of the affected joints. The normal pattern of walking is frequently modified by joint disease. strategies to minimize pain by avoiding full weight bearing on the affected limb will produce limping.
- 29. Urinary Incontinence: Urinary urgency and urge incontinence seen in ◦ spinal cord lesion ◦ parkinsonism ◦ subcortical white-matter ischemia. frontal lobe tumors, frontal lobe infarction, and hydrocephalus also produce urinary incontinence. Cognitive Changes: Slowing of gait may be a marker of impending cognitive impairment and dementia. executive dysfunction including inattention may produce falls. disinhibition and impulsivity are associated with reckless gait problems and falls.
- 30. EXAMINATION OF POSTURE AND GAIT First observe the overall pattern of limb and body movement during walking. Normal walking progresses in a smooth and effortless manner. The truncal posture is upright, and the legs swing in a fluid motion with a regular stride length. Synergistic head, trunk, and upper-limb movement flow with each step. After the overall walking pattern is observed, the specific aspects of posture and gait should be examined.
- 31. specific aspects of posture and gait includes: 1. Arising to stand from seated position 2. Stance and posture 3. Walking 4. Turning while walking 5. Other maneuvers ◦ Tandem walking ◦ Walking backwards ◦ Running ◦ Walking on toes, heels
- 32. Arising from Sitting: informs about ◦ pelvic girdle strength, ◦ control of truncal movement, ◦ coordination, and balance. proximal muscle weakness: Inability to rise when the feet are appropriately placed under the body. incoordination or imbalance: An abnormally wide stance base when standing. Frontal lobe diseases: Feet are not positioned directly under the body
- 33. Stance: Stance base = the distance between the feet gives an indication of balance. Wide stance base indicates poor balance. Wide-based gaits are ◦ typical of cerebellar or sensory ataxia ◦ diffuse cerebro vascular disease ◦ frontal lobe lesions. Eversion of the feet to increase stability seen in diffuse cerebrovascular disease. In mild ataxia, a widened base may only be evident with turning. Tandem (heel to toe) walking is a good objective measure of walking stability.
- 34. Trunk Posture: Flexion of the trunk and a stooped posture - PD. Upright posture with neck and trunk extension- PSP. Slight flexion at the hips to lower the trunk - feature of cautious gait. Neck flexion – MND Myasthenia gravis MSA Parkinsonism Tilt of the trunk to one side - dystonia. exaggerated lumbar lordosis ◦ stiff person syndrome[d/t Paraspinal muscle spasm] ◦ Proximal myopaties.
- 36. Truncal tilt away from the side of the lesion ◦ acute vascular lesions of the thalamus( postero lateral) and basal ganglia. Truncal tilt away from the side of the lesion ◦ Acute vestibular imbalance in the lateral medullary syndrome Truncal flexion (camptocormia) ◦ paraspinal myopathies that produce weakness of trunk extension. restricted range of spinal movement and persistence of the abnormal spinal posture when supine or during sleep are useful pointers toward a bony spinal deformity.
- 37. Postural Responses: 1.Reactive postural responses 2. anticipatory postural responses. 3.protective postural responses. .
- 38. pull test Reactive postural responses are examined by “the pull test”. Examiner sharply pulls the upper trunk backward or forward while the patient is standing. The pull should be sufficient to require the patient to step to regain their balance. The examiner must be prepared to prevent the patient from falling. A few short, shuffling steps backward or an impending fall backward or forward suggests impairment of righting reactions
- 39. Falls after postural changes such as arising from a chair or turning while walking suggest impaired anticipatory postural responses. Falls without rescue arm movements or stepping movements to break the fall indicate loss of protective postural responses. Injuries sustained during falls provide a clue to the loss of postural responses A tendency to fall backward spontaneously is a sign of impaired postural reflexes in PSP and gait disorders associated with frontal lobes
- 40. Romberg test Patients with proprioceptive loss depends on visual cues. the removal of vision greatly exaggerates the ataxia. This is the basis of the Romberg test. In which eye closure leads to a dramatic increase in unsteadiness and even falls in the patient with sensory ataxia. When performing the Romberg test, it is important the patient is standing comfortably before eye closure and to remember that a modest increase in body sway is a normal response to eye closure.
- 41. Walking: Initiation of Gait: start hesitation – difficulty in gait initiation. slipping clutch phenomenon ◦ few short, shuffling steps on the spot without forward progress. magnetic foot phenomenon. ◦ complete immobility with the feet seemingly glued to the floor Patients may make exaggerated upper-body movements or alter the step pattern.
- 42. Start hesitation seen in ◦ frontal lobe disease, ◦ diffuse cerebrovascular disease, ◦ hydrocephalus. ◦ gait ignition failure. ◦ PD Isolated start hesitation is seen in the syndrome of gait ignition failure.
- 43. Stepping: length and trajectory of each step and the rhythm of stepping should be noted. Short, regular, shallow steps or shuffling and a slow gait - akinetic-rigid syndromes. Freezing typically occurs when turning, when walking has been interrupted by an obstacle. Festination (increasingly rapid, small steps) is common in PD but rare in other akinetic-rigid syndromes.
- 44. Unilateral loss of synergistic arm swing while walking 1. valuable sign of early PD 2. Unilateral UMN lesion 3. acute cerebellar syndrome Turning: Requires more balance more than walking in a straight line. Slowing on turns may be the first abnormality in walking in PD Multiple steps on turning ◦ PD
- 45. More Challenging Tests of Walking: Tandem walking: Subtle degrees of cerebellar ataxia unmasked by tandem walking. Walking on toes and heels: may bring out abnormal movements as well as deficits in the strength of dorsiflexion and plantar flexion of the ankle. Walking backward: will sometimes reduce or abolish the dystonic foot posturing observed walking forward in action dystonia of the foot. Running: examine the patient running to identify an action dystonia of the legs in early stages.
- 46. Associated and Synergistic Limb Movements While Walking: Dystonic posturing of an arm or leg ◦ dystonia, ◦ parkinsonism, ◦ old hemiparesis. Choreiform movements are more prominent during walking than at rest in ◦ most chorea syndromes, ◦ levodopa-induced dyskinesia, ◦ tardive dyskinesia. Parkinsonian tremor of the dependent upper limb is often observed while walking.
- 47. MOTOR AND SENSORY EXAMINATION: motor and sensory function in the limbs is examined with the patient sitting or supine. The size and length of the limbs should be measured in any child presenting with a limp. The spinal column should be inspected for scoliosis, and the lumbar region for skin defects or hairy patches indicative of spinal dysraphism.
- 48. DISCREPANCIES ON EXAMINATION OF GAIT: minimal abnormal signs on physical examination of the recumbent patient, in contrast to the observed difficulty when walking. Cerebellar gait ataxia caused by a vermis lesion: ◦ perform the heel-to-shin test normally when supine but is ataxic when walking. Action dystonia: ◦ Abnormal posturing of the feet only when walking. ◦ A dystonic gait may be evident only when running or walking forward but not when walking backward.
- 49. Frontal lobe lesion, hydrocephalus,or diffuse cerebrovascular disease : ◦ Patient totally unable to walk when standing. ◦ Gegenhalten (paratonia), with or without brisk tendon reflexes, may be the only abnormal sign in the recumbent patient ◦ Such patients perform the heel-shin test and make bicycling movements of their legs normally when lying on a bed. Leg tremor of orthostatic tremor ◦ only appears during weight bearing, especially when standing still.
- 50. GAIT DISORDERS
- 51. CLASSIFICATION OF GAIT PATTERNS: A scheme based on Hughlings Jackson’s three orders of neurological function. Lower Level Gait Disorders (simplest) Middle Level Gait Disorders Higher Level Gait Disorders (complex, integrative ) Each level contributes sensory and motor function, but that of higher centers is more complex and dispersed within the nervous system.
- 52. Lower Level Gait Disorders manifest physical signs such as weakness or sensory loss. are due to diseases of the muscle and peripheral nerves that produce muscle weakness. Lower level sensory gait disorders follow loss of one of the three basic senses important for gait and balance: ◦ proprioception ◦ vision ◦ vestibular sensation.
- 53. Low level (sensory and motor) gait disorders: 1. Waddling gait - proximal weakness (myopathy) 2. high stepping gait - distal weakness (neuropathy) 3. Sensory ataxia – proprioception loss. 4. Vestibular ataxic gait -acute peripheral vestibulopathy 5. Gait difficulty due to acute visual impairment
- 54. Myopathic Weakness and Gait: Weakness of proximal leg and hip-girdle muscles interferes with stabilizing the pelvis and legs on the trunk. produces exaggerated rotation of the pelvis with each step and a waddling gait. The hips are slightly flexed (d/t hip extensor weakness). exaggerated lumbar lordosis. Gower’s sign positive myopathy is the most common cause of proximal muscle weakness, neurogenic weakness of proximal muscles can also
- 56. Neurogenic Weakness and Gait: Muscle weakness of peripheral nerve origin. typically affects distal leg muscles results in a steppage gait. The patient lifts the leg and foot high above the ground with each step because of weakness of ankle dorsiflexion and foot drop. unilateral foot drop: ◦ common peroneal or sciatic nerve palsy or an L5 radiculopathy Less common is foot drop caused by myopathic weakness, as in the scapuloperoneal syndromes. Weakness of ankle plantar flexion - shallow stepped gait.
- 58. A femoral neuropathy as in diabetes mellitus: ◦ produces weakness of knee extension and buckling of the knee when walking or standing. This may first be evident when walking down stairs. similar weakness: ◦ Progressive muscular atrophy in MND ◦ quadriceps myopathy ◦ inclusion body myositis
- 59. Sensory Ataxia: wide stance base advance cautiously taking slow steps under visual guidance. the feet are thrust forward with variable direction and height. The sole of the foot strikes the floor forcibly with a slapping sound - slapping gait. Romberg test positive. Walking on uneven surfaces is particularly difficult. Results from ◦ peripheral neuropathies, ◦ posterior root or dorsal root ganglionopathies, ◦ dorsal column lesions.
- 60. Vestibular Imbalance, Vertigo, and Gait: Acute peripheral vestibulopathy ◦ produce veering to the side of the lesion. ◦ Veering less prominent while running than walking. ◦ Patients prefer to lie stand still. In chronic vestibular failure, ◦ gait may be normal, ◦ unsteadiness can be unmasked during eye closure and rotation of the head from side to side while walking.
- 61. Middle-Level Gait Disorders Related to impaired modulation of force generated by the lower level motor system include: (1) spastic gait from corticospinal tract lesions (2) ataxic gait arising from disturbances of the cerebellum and its connections. (3) hypokinetic gaits associated with parkinsonism. (4) hyperkinetic gaits associated with chorea,dystonia, and
- 62. Spastic Gait: Spasticity of the arm and leg on one side: The leg is slightly flexed at the hip and extended at the knee, with plantar flexion and inversion of the foot. During the swing phase ◦ lateral flexion of the trunk toward the unaffected side. ◦ circumduction of the extended paretic leg. ◦ dragging the foot or catching the toe on the ground. ◦ Minimal associated arm swing occurs on the affected side. Muscle tone was increased on effected side along with brisk DTR and extensor plantar response.
- 63. Spasticity of both legs: legs are stiffly extended at the knees, plantar flexed at the ankles, and slightly flexed at the hips. Both legs circumduct, and the toes of the plantar flexed feet catch on the floor with each step. There is a tendency to adduct the legs, particularly when the disorder begins in childhood. [scissoring gait] Occasionally, bilateral leg dystonia (dystonic paraparesis) mimics a spastic paraparesis.
- 64. This typically occurs in doparesponsive dystonia in childhood. may be misdiagnosed as HSP or cerebral diplegia. Clinical differentiation between these conditions can be difficult. Brisk tendon reflexes occur in both, and spontaneous extension of a great toe in patients with striatal disorders may be interpreted as a Babinski response. Fanning of the toes and knee flexion suggest spastic paraplegia. Other distinguishing features include changes in muscle tone, such as spasticity in HSP and rigidity in dystonic paraparesis.
- 65. Cerebellar Ataxic gait: Lesions of spino cerebellum produces gait ataxia. wide-based stance. Steps are taken slowly and carefully. tendency to lurch and stagger. Accentuated by tandem walking Gait with lurching and staggering quality - midline cerebellar pathology. Swaying to one side
- 67. A pure truncal ataxia - midline (vermis) cerebellar syndrome. - normal examination in supine position Patients with anterior lobe atrophy: ◦ develop a 3-Hz antero posterior sway of the trunk and a rhythmic truncal and head tremor (titubation) that is superimposed on the gait ataxia. Lesions of vestibulo cerebellum: exhibit multidirectional body sway, & dysequilibrium.
- 68. Lesions of neo cerebellum: produce limb ataxia characterized by a decomposition of normal leg movement. Steps are irregular and variable in timing (dyssynergia), length, and direction (dysmetria). With lesions confined to one cerebellar hemisphere, ataxia is limited to the ipsilateral limbs there is little postural instability or truncal imbalance if the vermis is not involved. Cerebellar gait ataxia is exacerbated by the rapid postural adjustments like turning.
- 69. Spastic Ataxic gait: A combination of spasticity and ataxia produces a distinctive “bouncing” gait. Gait is wide based clonus is precipitated by standing or walking, creating a bouncing motion. Compensatory movements, made in an effort to regain balance, set up a vicious cycle of ataxic movements, clonus, and increasing unsteadiness, rendering the patient unable to stand or walk. Bouncing gaits must be distinguished from action myoclonus of the legs and cerebellar truncal tremors.
- 70. Hypokinetic (Parkinsonian) Gait: Early PD: ◦ Asymmetrical reduction of arm swing and ◦ Mild slowing in gait, particularly when turning. Advanced PD: ◦ stooped posture with flexion of the shoulders, neck, trunk. ◦ little associated limb movements while walking. ◦ the arms are held immobile at the sides or slightly forward. ◦ Rest tremor of the upper limbs is often apparent when walking but leg tremor is rare during walking. ◦ Begins with start hesitation with a few rapid, short, shuffling steps. ◦ Followed by shuffling gait with small, shallow steps on a narrow base with freezing episodes ◦ In the long term, levodopa therapy may induce
- 71. The posture of generalized flexion of the patient with PD exaggerates the normal tendency to lean forward when walking. To maintain balance when walking and avoid falling forward, the patient may advance with a series of rapid, small steps (festination). The shuffling gait of PD that is responsive to levodopa characterizes the mid-level gait pattern. As the disease progresses, dysequilibrium and falls emerge as features of a higher level gait disorder.
- 74. Choreic Gait: random movements of chorea - increased during walking. The superimposition of chorea on the trunk and leg movements gives the gait a dancing quality. Chorea can also interrupt the walking pattern, leading to a hesitant gait. Huntington disease ◦ causes a stumbling and stuttering gait with steps forward, backward, or to one side. ◦ Variable stance but generally wide-based ◦ Excessive swaying of trunk. ◦ Balance and equilibrium are maintained until the terminal stages
- 76. Dystonic Gait: Produce bizzare gait pattetns. classic presentation of childhood-onset primary torsion dystonia: ◦ action dystonia of a leg, with sustained abnormal posturing of the foot (typically plantar flexion and inversion) on attempting to run. In contrast, walking backward or even running backward may be normal at an early stage. Striatal toe: tonic extension of the great toe. Important early sign.
- 78. A characteristic feature common to dystonic gaits is excessive flexion of the hip when walking. Patients may hop or walk sideways in a crab-like fashion. Hyperflexion of the hips and knee produce an attitude of general body flexion in a simian posture. excessive flexion of the hip and knee and plantar flexion of the foot produce a birdlike (peacock) gait during the swing phase of each step. Many patients have been thought to be hysterical
- 79. Dopa-responsive dystonia ◦ characteristically presents in childhood with walking difficulties ◦ child walks normally in the early morning ◦ dystonic posturing of the legs increases as the day progresses or after exercise. ◦ Symptoms may be relieved by a nap (“sleep benefit”). ◦ Examination reveals dystonic plantar flexion and inversion of the foot, with brisk tendon reflexes. ◦ Some of these patients respond dramatically to levodopa. ◦ Indeed, all children presenting with a dystonic foot or leg should have a therapeutic trial of levodopa before other therapies such as anticholinergic drugs are commenced.
- 80. Paroxysmal kinesogenic choreoathetosis: ◦ present with difficulty walking as the result of dystonic postures and involuntary movements of the legs. ◦ often appearing after standing from a seated position. ◦ These attacks are typically brief, lasting a matter of seconds.
- 81. Mixed Movement Disorders and Gait: Athetoid cerebral palsy: Produce motor signs reflecting abnormalities at many levels of the nervous system. These include spasticity of the legs, truncal and gait ataxia, dystonia, and dystonic trunk and limb spasms. DD - primary torsion dystonia. patient with cerebral palsy usually has a ◦ history of perinatal injury or birth asphyxia. ◦ history of hypotonia. ◦ delayed developmental motor milestones. ◦ presence of spasticity and ataxia.
- 82. Tremor of the trunk and Legs: Leg tremor in benign essential tremor occasionally symptomatic. Trunk and leg tremor may contribute to unsteadiness in cerebellar disease. Orthostatic tremor: ◦ has a unique frequency (16 Hz) and distribution. ◦ rapid tremor produces an intense sensation of unsteadiness often with little obvious shaking of the legs. ◦ relieved by walking or sitting down. ◦ Patients avoid standing still (e.g., in a queue) and may shuffle on the spot in an effort to relieve the unsteadiness. ◦ Examination reveals a rippling of the quadriceps muscles during standing.
- 83. Action Myoclonus: Postanoxic action myoclonus of the legs is often accompanied by negative myoclonus (asterixis) that disrupts standing and walking. Repetitive action myoclonus produces jerky movements of the legs. Lapses of muscle activity between the jerks (negative myoclonus) cause the patient to sag toward the ground. sequence of events gives rise to an exaggerated bouncing appearance, which is sustainable for only a few seconds before falling.
- 84. Difficulty walking is one of the major residual disabilities of post-anoxic myoclonus. Stimulus sensitive cortical reflex myoclonus ◦ similar disorder of stance and gait, ◦ reflex myoclonus of the quadriceps, resulting in a bouncing posture. acute onset negative myoclonus can occur with vascular lesions , particularly of the thalamus and frontal lobes.
- 85. Higher Level Gait Disorders characterized by varying combinations of ◦ dysequilibrium, ◦ Falls due to impaired postural responses ◦ short shuffling steps, and freezing. formal neurological examination fails to reveal signs that adequately explain the gait disturbance. Slowness of sequential leg movement and poor truncal control are often present.
- 86. Stepping patterns are influenced by environmental cues that induce freezing of gait. Freezing or falling while performing multiple simultaneous tasks is common. a variety of terms for higher level gait disorders such as ◦ apraxia of gait, ◦ magnetic gait, ◦ lower half parkinsonism, ◦ frontal gait,
- 87. Hypokinetic Higher Level and Freezing Gait Patterns: With progression of PD, ◦ freezing of gait, ◦ disequilibrium, ◦ loss of postural responses and falls become increasingly troublesome. This will poorly respond to levodopa therapy. DBS of ( STN / Gpi ) may improve or worsen gait with increased falls. DBS in the region of the pedunculopontine nucleus is under investigation for dysequilibrium and freezing of gait.
- 88. Akinetic rigid syndromes: most common are MSA,PSP,CBD. Gait patern was similar to PD except festination is less common. Another distinguishing feature is early appearance of falls due to loss of postural and righting responses. Falls occur in 80% of patients with progressive supranuclear palsy and can be dramatic, leading to injury. Dramatic response to levodopa that is typical of PD does not occur in these other akinetic rigid syndromes.
- 89. Gait in frontal lobe lesions: Varies from an ataxic gait to an akinetic-rigid gait Often had combination of these features. early stages - wide stance base with turning difficulty. There may be episodes of freezing. Arm swing is normal or even exaggerated, giving the appearance of a “military two-step” gait. The normal fluidity of trunk and limb motion is lost. voluntary upper limb and hand movements are normal and there is a lively facial expression.
- 90. There difficulty in gait initiation [slipping clutch or magnetic feet]. Once walking is underway, steps may be better. freezing re-emerge while attempting to turn. Upper motor neuron signs including pseudobulbar palsy paratonic rigidity (gegenhalten) , Frontal releasing signs commonly occurs. Postural and righting reactions are impaired and eventually lost. Urinary incontinence and dementia frequently occur.
- 91. Called as “lower half parkinsonism” or marche à petits pas of Dejerine or Critchley’s atherosclerotic parkinsonism. Commonly seen in diffuse small vessel cerebrovascular disease. upper motor neuron signs including pseudobulbar palsy, and the absence of a resting tremor distinguish this syndrome from PD.
- 93. syndrome of gait ignition or gait initiation failure: ◦ Also called as “pure akinesia” or “primary progressive freezing of gait.” ◦ exhibit profound start hesitation and freezing. ◦ but step size and rhythm are normal once walking is underway. ◦ These findings are similar to those seen with walking in PD. ◦ but speech and upper limb function are normal ◦ there is no response to levodopa.
- 94. some elderly patients experience severe walking difficulties that resemble those described in frontal lobe disease. The history is usually of gradual onset, without stroke- like episodes. No identifiable lesions of the frontal lobes or in white matter on imaging. The criteria for normal pressure hydrocephalus are not fulfilled. there are no signs of parkinsonism and levodopa is ineffective. There is no evidence of more generalized cerebral dysfunction. The cause of these syndromes is unknown although it is increasingly recognized that subcortical white-matter
- 95. ELDERLY GAIT PATTERNS CAUTIOUS GAITS: Healthy, neurologically normal elderly people ◦ Walk at slower speeds ◦ Shorter and shallower steps ◦ Stance width slightly wider than normal ◦ Synergistic associated arm movements are less vigorous. ◦ The rhythmicity of stepping is preserved.
- 96. These changes give the normal elderly gait a cautious or guarded appearance. Factors contributing to a general decline in mobility of the elderly include ◦ degenerative joint disease, ◦ reducing range of limb movement, ◦ decreased cardiovascular fitness, ◦ limiting exercise capacity.
- 97. A cautious gait is a normal response to the perception of impaired or threatened balance. They may be unable to walk without support. The gait improves dramatically when support is provided. Accordingly, a cautious gait should be interpreted as compensatory and not specific for any level of the gait classification. A formal program of gait retraining may help restore confidence and improve the ability to walk.
- 98. RECKLESS GAIT PATTERNS: seen in patients with impaired postural responses and poor truncal control. Patients do not recognize their instability and take risks that result in falls and injuries. Such patients make inappropriate movements of the feet and trunk when sitting or standing. The most striking examples occur in frontal dementia. impulsivity and a failure to adapt to the precarious balance are part of the cognitive decline.
- 99. HYSTERICAL GAIT DISORDERS The typical gait patterns encountered include: 1. transient fluctuations in posture while walking 2. knee buckling without falls 3. excessive slowness and hesitancy 4. stooped or other abnormal posture of the trunk 5. complex postural adjustments with each step 6. exaggerated body sway or excessive body motion especially brought out by tandem walking.
- 100. common features of psychogenic gait (and movement) disorders are: ◦ Suggestibility ◦ Variability ◦ Improvement with distraction, ◦ History of sudden onset ◦ Rapid, dramatic, and complete recovery. Other signs like give away weakness or non physiological sensory loss will be present. Hoover sign: ◦ As the patient lifts the normal leg, the examiner places a hand under the “paralyzed” leg and feels the presence (and strength) of synergistic hip extension.
- 101. ASTASIA – ABASIA: Unable to either stand or walk, More or less normal use of their legs while in bed Normal neurologic examination When such patients are placed on their feet, they may take a few steps and then become unable to advance their legs. they lurch in all directions and crumple to the floor if not assisted BEFORE LABELLING A HYSTERICAL GAIT, RULE OUT 1. Lesions of anterosuperior cerebellar vermis 2. NPH 3. Frontal lobe disease 4. Intoxications such as with phenytoin