Seal of Good Local Governance (SGLG) 2024Final.pptx
thyroid & antithyroid drugs..
1. Thyroid & Antithyroid Drugs
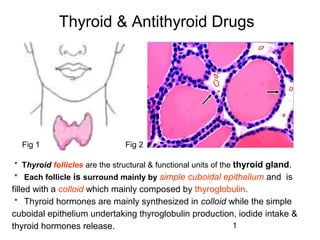
Fig 1 Fig 2
* Thyroid follicles are the structural & functional units of the thyroid gland.
* Each follicle is surround mainly by simple cuboidal epithelium and is
filled with a colloid which mainly composed by thyroglobulin.
* Thyroid hormones are mainly synthesized in colloid while the simple
cuboidal epithelium undertaking thyroglobulin production, iodide intake &
thyroid hormones release. 1
2. ●Synthesis of thyroid hormones
Thyroid hormones MIT: monoiodotyrosine
triiodothyronine (T3) DIT: diiodotyrosine
tetraiodothyronine (T4, thyroxine)
Materials
iodine & tyrosine Thioamid
e drugs
Steps
1. Iodide is trapped by sodium-iodide symporter
2. Iodide is oxidized by thyroidal peroxidase to iodine
3. Tyrosine in thyroglobulin is iodinated and forms MIT & DIT
4. Iodotyrosines condensation
MIT+DIT→T3; DIT+DIT→T4 2
3. Intra-thyroidal synthesis and processing of thyroidal hormones
1. Iodide is taken up at the basolateral cell thyroidal peroxidase
membrane and transported to the apical
membrane
2. Polypeptide chains of Tg (thyroglobulin) are
synthesized in the rough endoplasmic reticulum,
and posttranslational modifications take place in
the Golgi
3. Newly formed Tg is transported to the cell surface
in small apical vesicles (AV)
4. Within the follicular lumen, iodide is activated and
iodinates tyrosyl residues on Tg, producing fully
iodinated Tg containing MIT, DIT, T4 and a small
amount of T3 (organification and coupling), which
is stored as colloid in the follicular lumen
5. Upon TSH stimulation, villi at the apical
membrane engulf the colloid and endocytose the
iodinated Tg as either colloid droplets (CD) or
small vesicles (MPV)
6. Lysosomal proteolysis of the droplets or vesicles
hydrolyzes Tg to release its iodinated amino acids
and carbohydrates
7. T4 and T3 are released into the circulation
8. DIT and MIT are deiodinated, and the iodide and
tyrosine are recycled 3
4. ●Regulation of thyroid function
TRH: thyrotropin-releasing hormone
TSH: thyroid-stimulating hormone
4
5. ●Physiological actions of thyroid hormones
To normalize growth and development, body temperature,
and energy levels
▲Insufficiency→ cretinism (infant & child), and
myxedema (adult);
▲Excess→hyperthyroid
To enhance CNS excitability & sensitivity of CVS to NA
# T3 is 3 to 4 times more potent than T4 in heat production;
# T4 in colloid is about 4 times more numerous than T3 ;
5
7. Myxedema
Stems from both the hyperthyroid and hypothyroid conditions,
results from the accumulation of increased amounts of
hyaluronic acid and chondroitin sulfate in the dermis in both
lesional and normal skin.
The mechanism that causes myxedema is still not yet
understood. Sympotoms include:
●Skin thickening ●Coarse skin ●Change in facial appearance
●Thickening nose ●Swollen lips ●Puffiness around the eyes
●Jelly-like infiltrations in subcutaneous tissues ●Slow speech
●Mental dullness ●Lethargy ●Mental problems
●Dry skin ●Yellow skin ●Swollen subcutaneous tissue
●Weight gain ●Constipation ●Thinning hair
● Brittle hair ●Bald patches ●Muscle pains
7
8. ●Mechanism of actions
of thyroid hormones
T3, via its nuclear
• Some of T4 are converted to T3 in
receptor, induces
kidney and liver
new proteins
• The actions of T3 on several
organ systems are shown generation which
produce effects
• BMR: basal metabolic rate; CNS:
central nervous system
8
9. Thyroid drugs
● Representative drugs
levothyroxine (L-T4, levoxyl, synthroid)
liothyronine (T3, cytomel, triostat)
liotrix (T4 plus T3) (euthyroid, thyrolar)
● Pharmacokinetics
po easily absorbed; the bioavailablity of T4 is 80%, and T3 is
95%.
Drugs that induce hepatic microsomal enzymes (e.g., rifampin,
phenbarbital, phenytoin, and etc) improve their metabolism.
9
10. ●Pharmacological effect
see physiological effect
● Clinical use
1. Hypothyroidism: cretinism & myxedema;
2. simple goiter: for pathogeny remaining unclear
(endemic goiter directly supply iodine)
3. Others:
● Adverse reactions
Overmuch leads to thyrotoxicosis;
Angina or myocardial infarction usually appears in
ageds
10
11. Antithyroid drugs
● Drugs
Class Representative
propylthiouracil
methylthiouracil
Thioamides
methimazole
carbimazole
Iodides KI, NaI
Radioactive iodine 131
I
β-adrenoceptor blockers propranolol
11
13. Pharmacological action
Inhibition of the synthesis of T3 & T4
Mechanism
All thioamides inhibit peroxidase-catalyzing reactions
Iodine organification First choice for
Iodotyrosines condensation thyroid crisis
Propylthiouracil also inhibit T4 converting to T3
Characteristics
① Result appears slowly: in 3-4 w hyperthyroid
ameliorated, and in 2-3 months BMR normalized;
② Long-term use leads to thyroid hyperplasia
③ Methimazole is 10 times as potent as propylthiouracil
13
14. Clinical use
treatment of hyperthyroid
1. Mild hyperthyroid and those surgery & 131I
not permitted;
2. Operation preparation;
3. Thyroid crisis (comprehensive therapy).
Adverse reactions
1. Long-term use leads to thyroid hyperplasia;
2. Pruritic maculopapular rash is the most common
adverse raaction
3. The severe adverse reaction is agranulocytosis
14
15. Iodides (NaI, KI)
Pharmacological action
Inhibition of T3 & T4 release and synthesis
Decrease of size & vascularity of the hyperplastic gland
Clinical use
Ministrant treatment of hyperthyroid
1. Operation preparation;
2. Thyroid crisis.
Adverse reactions
1. Acneiform rash (similar to that of bromism);
2. Swollen salivary glands, mucous membrane ulcerations, and etc.
15
16. Radioactive iodine (131I)
131
I is the only isotope for treatment of thyrotoxicosis.
Its therapeutic effect depends on emission of β rays with an
effective half-life of 5 days & a penetration range of 0.4-2 mm.
Woman in pregnancy or lactation is forbidden!
β-adrenoceptor blockers
βblockers are effective in treatment of thyrotoxicosis.
Propranolol is the most widely studied and used.
16