1. Get Homework/Assignment Done
Homeworkping.com
Homework Help
https://www.homeworkping.com/
Research Paper help
https://www.homeworkping.com/
Online Tutoring
https://www.homeworkping.com/
click here for freelancing tutoring sites
College of Nursing
Pamantasan ng Lungsod ng Maynila
(University of the City of Manila)
Intramuros, Manila
A Case Study on
Spinal Cord Injury
secondary to
Giant Cell Tumor
2. IN PARTIAL FULLFILMENT FOR THE REQUIREMENTS
IN GRAND CASE PRESENTATION
Submitted by:
Group J
Agustin , Christian Jefferson B.
Alicando, Zarah Jane
Ape, Joan Olivia G.
Aquino, Rae Marie G.
Arlegui, Jeyzel H.
Austria, Alesi Marian S
Bacani, Aeimil Clarize D
Baraquia, Maria Leona Victoria G.
Barrientos, Katrina
Batingan, Irene C.
Briones, Aillene Jade
Cabanela, Jessica
Submitted to:
Prof. Raymond Fernandez RN, MAN
August 02, 2012
I. INTRODUCTION
Spinal cord injury is a damage to any part of the spinal cord or nerves at the end
of the spinal canal. It often causes permanent changes in strength, sensation and other
body functions below the site of the injury. Depending on where the spinal cord
and nerve roots are damaged, the symptoms can vary widely, from pain to paralysis to
incontinence. It is estimated that the annual incidence of spinal cord injury not including
those who die at the scene of the accident, is approximately 40 cases per million
population in the U. S. or approximately 12,000 new cases each year. Spinal cord
3. injuries typically occur during an individual's most productive years, between the ages of
16 and 30
Giant cell tumor is an osteolytic tumor affecting the metaphyses and epiphyses
of long bones, composed of a stroma of spindle cells containing dispersed multinucleate
giant cells, and usually being benign but sometimes malignant. It generally occurs in
adults between the ages of 20 and 40 years. It is very rarely seen in children or in adults
older than 65 years of age. Giant cell tumors occur in approximately one person per
million per year.
The patient is a 35 year old male, admitted at 6:00 pm of August 30, 2011 at
Philippine General Hospital Spine Ward. The patient’s chief complaint is back pain .
After series of assessment and procedures, the patient had been diagnosed of Spinal
cord injury, T12, complete, Asia A secondary to giant cell tumor
On July 23-24, 2012, the patient was in the care of Group J of BSN IV. The
patient has been handled for two days by the said group.
For an organized investigation, this case study is composed of the background of
the patient, anatomy and physiology related to the case, laboratory findings, drug study
of the patient’s medications, and interventions necessary for the patient.
4. II. OBJECTIVES
General:
This study aims for its readers to understand the cause, manifestations,
treatments and preventions of CHF, secondary ASHD, to consider COPD which will
lead to an increase of awareness of every individual who may have this kind of disease
and to the members of the health care team who have read this case study.
Specifically, the nursing students intend to appreciate the patient’s condition in
practice of the Medical-Surgical nursing through:
5. 1. Gather all necessary information regarding the patient and his family members
as may be related to our case study.
2. Ascertain patient’s past and present health history.
3. Perform physical assessment on patient’s condition so as to attain baseline data.
4. Present the definitions of the complete diagnosis that would explain the illness of
our patient.
5. Determine the diagnostic tests, their implications, significance and analysis of the
patient.
6. Utilization of the medical and or surgical procedures possible or indicated for the
management of the patient
7. Identify and prioritize the need of our patient.
8. Formulate an appropriate nursing care plan based on the assessment identified
needs and problems of the patient.
III. NURSING HEALTH HISTORY:
A. Biographic data:
a. Name : AP
b. Address: Paranaque
c. Age: 35 y/o
d. Date of birth: June 21, 1977
6. e. Place of birth: Paranaque
f. Occupation: Body Guard
g. Marital status: Married
h. Number of children: 4
i. Gender: Male
j. Religion: Iglesia ni Kristo
k. Date and time of admission: August 30, 2011, 6:00pm
l. Date received: July 23, 2012
m. Source of information: Patient himself, patient’s sister and the patient’s
chart which both have 100% reliability
.
B. Chief Complaint:
Obtained from admitting history : Back pain
Admitting Diagnosis:
Spinal cord injury, T12, complete, Asia A secondary to giant cell tumor
C. History of Present Illness
The patient explained that 9 months prior to his admission, he had
acute onset of low back pain, localized, with pain scale of 5/10, aggravated by
prolonged standing, usually noted in the afternoon, usually relieved by rest. He
self-medicated with unrecalled pain medications with temporary relief. No
associated signs and symptoms. Condition tolerated. There was no history of
7. trauma. 8 months prior to admission, there was persistence of condition thus,
decided to seek consult at a private hospital where work up was done with an
impression of Pott’s disease. Patient followed up frequently however there was
no relief of symptoms. 7 months prior to admission, condition persisted with
increased severity of pain to 10/10. This was relieved by overnight rest. 5
months prior to admission, there was persistence of pain but now with
involvement of the thighs down to the level of the knees. Patient still had intact
motor and sensory function as claimed. Sought consult where MRI was done
showing tumor on T12 vertebral body with L4-L5 diffused disc bulge. He was
advised for surgical management however, did not pursue due to financial
constraints. 2 months prior to admission, patient was admitted for 2 weeks for
alternative medicine treatment with no relief of symptoms. 1 week prior to
admission, patient had reflexology treatment where patient stretching was done
and claimed to have aggravated the pain, and frequency. Pain was now partially
relieved by rest and pain relievers. 3 days prior to admission, patient was unable
to move lower extremities and gradual onset of numbness. At August 30, 2011,
6:00pm, he was admitted with a chief complaint of Back pain at Philippine
General Hospital .
D. Past Medical Health History
Patient stated that he has been vaccinated but he could no longer
remember what vaccines were given. Patient reported that he has no allergies to
foods, medications, dust, pollen, animals, etc. and had never been in any
accident. He stated that he has never been hospitalized before.
8. E. Family History of Illness
The patient explained that he have no family history of any disease
F. Lifestyle:
The patient stated that he works as a bodyguard during weekdays
as a source of their income. He also stated that they have a sari-sari store
9. as another source of income. He stated that he has a good appetite and
was eating 3 times a day- breakfast, lunch and supper respectively. He
stated that he eats vegetables and meat. The patient also stated that he
has an average of 8 hours of sleep per day, usually from 8:00pm to
4:00am. On weekends, the patient helps out with household chores like
going to the grocery and washing dishes. He also takes his turn in selling
at their sari-sari store. The patient stated that this is his regular time
allocation but it still varies with regards to different factors which he named
as weather, and emergency situations which needed his presence.
G. Social Data:
The patient stated that he has a good relationship with his wife and
children. They seldom quarrel at home. His four sons, both living with him
also share their problems and they haven’t encountered any problem in
communicating with one another. The patient stated that they seek help
from their neighbours and other family members in the times of
emergency situations or in case of calamity.
H. Psychologic Data:
In the past, the patient usually goes out to play with his children, read
the news paper, does household chores (ie. going to wet market to buy
food), and sells at their sari-sari store in order to pass the time. Currently,
he finds time to read the news, listen to music, and play chess with his
children when they come to visit
10. I. Patterns of Health Care
The patient has explained of not having any family physician, he
usually self medicates and consults hospitals if the symptoms still persists
11. IV. GORDON’S FUNCTIONAL HEALTH PATTERNS
BEFORE HOSPITALIZATION DURING HOSPITALIZATION
1) Health Perception
Health
Management
Pattern
• The patient perceives
that he is healthy
because he can
perform his activities of
daily living well.
• The patient feels
healthy except for his
disability
2) Nutritional
Metabolic Pattern
• The patient’s
significant other stated
that “Ang alat niya kasi
magtimpla ng ulam,
tapos ang hina pa
uminom ng tubig”. The
patient also stated that
“Madalas 24hours ang
biyahe ng taxi ko, pero
hindi ko nauubos yung
isang bote (referring to
a 1 liter bottle) ng tubig
na baon ko”.
• The patient stated that
during his
hospitalization, “Wala
naman akong reklamo
sa pagkain ko.”
3) Elimination Pattern • The patient urinates
and defecates
• “nakakaihi ako dahil sa
catheter ko at
12. everyday nakakadumi” as stated
by patient IV.
4) Activity Exercise
Pattern
• The patient states that
his activity was his
usual job, doing
household chores and
playing basketball with
his children
• The patient stated,
“Nakakapag-exercise
ako araw-araw gamit
yung mga bote ng tubig
at nagpapatulong ako
para sa paa ko”. The
patient also stated that
he cannot perform his
job anymore.
5) Sleep Rest Pattern • The patient stated that
his usual sleep was
10pm until 6am
because of his duty as
a taxi driver.
• “Sapat naman tulog ko
at madalas akong
nakakapagpahinga” as
stated by his significant
other.
6) Cognitive
Perceptual Patter
• The patient is well
oriented with time,
place and person.
• The patient is still
oriented with time,
place and person.
7) Self-Perception
Self-Concept
Pattern
• The patient stated that
he is a person that
helps his family.
• “Dapat ako nag-aalaga
pero ngayon ako ang
inaalagaan”, as stated
by patient.
8) Role-Relationship
Pattern
• The patient stated that
he was the provider of
the family and that he
• The patient stated that
his wife and children
visit and take care of
13. helps in taking care of
his children
him in the hospital
9) Sexuality-
Reproductive
Pattern
• The patient stated that
they are active during
their rest days.
• The patient and his
significant other are not
having sexual
intercourse.
10)Coping-Stress
Tolerance Pattern
• “Palagi kong nililibang
ang sarili ko, naglalaro
ng basketball kasama
ang mga anak ko,
namamalengke o
nagtitinda sa tindahan
namin” as stated by
the patient.
• “Mas relaxed ako
ngayon kasi palagi
akong nakahiga. Sana
nga lang mapa-in-cash
yung guarantee letter
ko”, as stated by
patient IV.
11)Value-Belief Pattern • “Palagi akong
nasamba at
namamanata sa aming
kapilya” as stated by
the patient
• The patient offers up a
prayer every now and
then.
V. REVIEW OF SYSTEMS
Skin
14. The patient stated that he doesn’t have any feeling of itchiness all over his body.
He also stated that he has a scar on his back from the operation and also ulcerations
that have healed on the calcaneal region
Eyes
The patient stated that he is not experiencing visual disturbances like excessive
tearing or night blindness. He said that he has no sensation of pain in his eyes. He also
stated that he doesn’t use eye glasses or contacts.
Ears
The patient stated that he doesn’t experience any hearing deficits, feeling of light
headedness, or ringing in the ears. The patient said that he doesn’t use hearing aid and
he doesn’t have any discharge or pain in the ears.
Mouth
The patient stated that he brushes his teeth every morning. He said that he
doesn’t use dental floss or any mouth wash. He stated that he is not having tooth ache,
bleeding or swollen gums, difficulty in chewing, or change in taste sensation.
15. Breast and Axilla
The patient stated that he doesn’t feel pain or tenderness in his breast. He said
that he doesn’t have any breast disease or cancer and presence of unusual discharge.
Endocrine
The patient said that he is not experiencing mood swings. He said that he doesn’t
have allergic reactions to any food or drugs. He also stated that he doesn’t experience
excessive hunger, thirst, or increase in urination.
Neurological
The patient stated that he doesn’t have any sensory impairment. He also said
that sometimes he is experiencing dizziness or when he tries to stand. He said that he
doesn’t experience loss of memory, change in speech, or any involuntary movements.
Cardiovascular
The patient stated that he doesn’t experience chest pain and palpitations. The
patient said that he doesn’t experience any difficulty in sleeping in supine position.
Respiratory
16. The patient stated that he has no difficulty in breathing. He also stated that he
does not experience any pain when coughing
Gastrointestinal
The patient stated that he doesn’t have diarrhea or constipation. He admitted that
he does not feel pain in his abdomen. He said that he defecates at least once every
other day.
Musculoskeletal
The patient stated that he has no vascular pain in extremities. He also said that
he could not move his lower extremities and a feeling of numbness.
Urinary
The patient stated that he does not experience physical discomfort even with a
foley catheter inserted.
17. VI. Physical Assessment
General Survey
The patient was received conscious, coherent and oriented. The patient is lying
on bed with indwelling foley catheter attached to a urine bag draining well. The patient
shows no signs of distress. The patient’s movement is coordinated.
The patient’s vital signs are as follows:
Blood Pressure: 120/80
Respiratory Rate: 22 cpm
Pulse Rate: 81 bpm
Temperature: 36.7o
C
Head (Skull, Scalp, Hair)
18. Head is normocephalic and all of the structures are symmetrical. There were no
presence of any lesions, scales and infestations. Hair is black, lustrous, curled, and oily.
There’s no area of patchy hair loss or excessive hair growth.
Skin and Nail
Skin color is fair, no pallor, jaundice, or cyanosis. Discoloration of skin found on
thoraco-lumbar region of the back. The patient shows grade 1 ulcerations on lower
extremities on the calcaneal region. Angle of the nail base is 160 degrees. Nail edges
are even. The client’s skin temperature is within normal range. Using the blanch test,
the clients capillary refill was slightly pink for about 4-5 seconds.
Eyes
Eyes have no edema, scaling or lesions present on the eyelids. Eyelids
completely cover the corneas when closed. Eyelid color is the same as surrounding skin
color. Upper eyelids are symmetrical and lesion free, and don’t sag or droop when the
patient opens her eyes. Eyelashes are evenly distributed and curve outward. Globe of
the eye neither protrudes nor is sunken into the orbit. Eyebrows are of equal size, color
and distribution. Nystagmus is not present. The patient has a pale conjunctiva. White
sclera is visible through conjunctiva. Lids of both eyes close when stoke each cornea
with a wisp of cotton. Pupils are round, reactive to light and accommodation. Both pupils
constrict when you light on one. Eyes are properly aligned. Eye movement in each of
the six cardinal fields of gaze is parallel. Eyelids show no evidence of swelling or
tenderness. Globes feel equally firm, not overly hard or spongy.
19. Ears
Auricles are bilaterally symmetrical and proportionately sized. Tip of the ear
crosses the eye-occiput line. Ears and facial skin are the same color. No inflammation,
lesions, or nodules are apparent. No cracking, thickening, scaling or lesions are
detectable behind the ear. No visible discharge from the auditory canal was apparent.
External meatus is patent. Skin color on the mastoid process matches the skin color of
the surrounding area. No masses or tenderness on the auricle tragus is detectable
during palpation. Mastoid process has well-defined bony edges with no signs of
tenderness.
Nose
Nose is symmetrical and lesion free, with no deviation of the septum or
discharge. Nostrils are patent without any obstructions and nasal flaring is not apparent.
Upon palpation, there were no masses as well as tenderness and lesions on his
sinuses. Patient can identify familiar odors. No evidence of foreign bodies or dried blood
in the nose. External nose is free from structural deviation, tenderness and swelling.
Mouth
Lips are pink and non-tender with no fissures, lesions, or cyanosis and with
dryness. Patient can purse his lips and puff out her cheek. Patient can easily open and
close his mouth. Oral mucosa is light pink and moist with no ulcers or lesions. Palate is
pink and soft. Gums are pink, with no inflammation and bleeding. Tongue is pink, with
20. no swelling, coating, ulcers, or lesions. Tongue moves easily and without tremor.
Tonsils are lesion free and are right in size for the patient’s age. Voice is clear yet
minimal. Uvula moves upward when the patient says “ah”. Lips are free from pain and
indurations. Floor of the mouth is free from tenderness, nodules and swelling.
Neck
Neck is symmetrical with intact skin and no visible pulsations, masses, swelling,
venous distention, or thyroid or lymph node enlargement. Lymph nodes are not
palpable.
Breast
Breast skin is smooth, undimpled, and the same color as the rest of the skin.
Breasts are symmetrical. The patient has edema but no erythema, skin or nipple
dimpling or nipple discharge is apparent. Nipples are round and protrude. No nodules
or unusual tenderness is apparent. Axillary nodes feel soft, small and not tender.
Thorax and Lungs
Chest configuration is symmetrical side-to-side. Anteroposterior diameter is less
than the transverse diameter, with a ratio 1:2. Chest shape is normal with no
deformities, like barrel chest, kyphosis, retraction, sternal protrusion, or depressed
sternum. Costal angle is less than 90 degrees, with the ribs joining the spine at a 45-
degree angle. Respirations are labored. Chest wall expands symmetrical during
21. respirations. Skin color matches the rest of the body’s complexion. Skin is warm and
dry. No tender spots or bulges in the chest are detectable. Upon auscultation, crackles
were heard.
Cardiovascular System
No pulsations were visible, except at the point of maximal impulse in the left 5th
intercostal space. No lifts or retractions are visible in the four valves area of the chest
wall. No vibrations or thrills are detectable. No murmurs were heard.
Abdomen
Abdomen is flabby and soft. No variations in the color of the patient’s skin are
detectable. The abdomen moves with respiration. The liver, spleen and kidneys are
non-palpable.
Urinary
The patient has a Foley catheter in place with a urine output level of 550 ml for
about 8 hours.
Musculoskeletal System
22. No gross deformities are apparent. Body parts are symmetrical. Body is in
alignment. No involuntary movements are detectable. All muscles and joints of upper
extremities have active range of motion, with no pain. Bilateral limb strength of upper
extremities is equal. Lower extremities have no sensory and motor function. No
involuntary contractions or twitching is detectable.
Neurologic System
Patient can shrug his shoulders. Pupils are equal, round, and reactive to light.
The lids of both eyes close when you stroke each cornea with a wisp of cotton. Patient
can identify familiar odors. Patient can hear a whispered voice. Patient can purse his
lips and puff out his cheeks. Tongue moves easily and without tremor. No involuntary
movements are detectable. Patient is oriented to herself, to other people, place, and
time. Memory and attention span are intact. Deep tendon reflexes are present. Strength
in the facial muscles is symmetrical. The patient’s cranial nerves were assessed as
follow:
CN I: the patient can identify the smell of coffee while eyes are closed.
CN II: the patient can read written words.
CN III, IV, VI: Pupils are equally round and reactive to light and accommodation.
Extra ocular eye movements are intact and move in unison.
CN V: he is able to clench her teeth
CN VII: the patient is able to puff out cheeks and purse lips with symmetry. He
can demonstrate different facial expression.
23. CN VIII: He is able to hear and respond to spoken words with a normal voice
tone
CN IX, X: the patient’s voice is negative for hoarseness. He can swallow without
difficulty. He can move his tongue side-to-side and up-and-down.
CN XI: neck muscle strength resistance is equal.
CN XII: Patient can protrude tongue and can move it side-to-side.
VII. ANATOMY AND PHYSIOLOGY
SKELETAL SYSTEM
Functions of The Skeleton
1. Support
• The skeleton is the framework of the body, it supports the softer tissues
and provides points of attachment for most skeletal muscles.
2. Protection
• The skeleton provides mechanical protection for many of the body's
internal organs, reducing risk of injury to them.
For example, cranial bones protect the brain, vertebrae protect the spinal
cord, and the ribcage protects the heart and lungs.
3. Assisting in Movement
24. • Skeletal muscles are attached to bones, therefore when the associated
muscles contract they cause bones to move.
4. Storage of Minerals
• Bone tissues store several minerals, including calcium (Ca) and
phosphorus (P). When required, bone releases minerals into the blood -
facilitating the balance of minerals in the body.
5. Production of Blood Cells
• The red bone marrow inside some larger bones (including, for example,
the ....) blood cells are produced.
6. Storage of Chemical Energy
• With increasing age some bone marrow changes from 'red bone marrow'
to 'yellow bone marrow'.
Yellow bone marrow consists mainly of adipose cells, and a few blood
cells. It is an important chemical energy reserve.
The axial skeleton provides: (a) structural support for the body, (b) attachment points
for ligaments and muscles, and (c) protects the brain, spinal cord and major organs of
the chest. The axial skeleton includes bones of the skull, inner ear, chest and spinal
column.
Bones of the Skull: Can be categorized into two groups: (A) Neurocranium and (B)
Splanchnocranium. With the exception of the mandible, all the bones of the skull are
joined together by sutures.
The Neurocranium includes the following bones:
• Frontal bone: makes up the forehead and part of the eye orbits and part of the
nasal cavities.
• Parietal bones: here are 2 parietal bones, which articulate together and form the
roof of the cranium.
• Temporal bones: one on either side of the skull, contain the inner ear. These
bones also provide a foramen (canal) for the major blood supply to the brain, the
carotid artery and jugular vein.
• Occipital bone: makes up the back and floor of the cranium. The brainstem
passes through this bone and then continues as the spinal cord.
• Ethmoid bone: forms the front part of the cranial floor, part of the eye orbits, and
contains the ethmoid sinuses.
25. • Sphenoid bone: contains the sphenoidal sinus cavity. Has a unique depression
called the sella turcica, which houses the pituitary gland.
• Palatine Bone: these bones are at the back of the roof of the mouth. They form
the wall of the nasal cavities and the floor of the eye orbit.
Bones of the Face: The bones of the face (Splanchnocranium) are 14 in total. They
are: 2 nasal, 2 maxilla, 2 zygomatic, 2 lacrimal, mandible, 2 palatine, 2 inferior nasal
conchae and vomer.
• Lacrimal Bone: is the smallest bone of the face, from part of the inside wall of
the eye orbit.
Nasal Bone: the two nasal bones meet in the middle and this forms the bridge of
the nose.
Inferior Nasal Conchae: these bones form the lateral wall of the nasal cavity and
cause the inhaled air to swirl and be filtered.
• Vomer Bone: is a triangular shaped bone that forms part of the nasal septum.
Zygomatic Bone: it is a paired bone, which makes up the lower eye orbit and is
frequently referred to as the cheekbone.
• Maxilla Bone: the largest bones of the face; they form together to make the
whole upper jaw. These bones hold the upper teeth.
• Mandible Bone: the strongest bone of the face; it forms the lower jaw and holds
the lower teeth. It is the only bone of the skull that moves.
• The hyoid bone is a bone in the neck, which does not articulate with any other
bone. Muscles of the neck support it and it provides support for the root of the
tongue; it is involved in the production of speech.
Bones of the Inner Ear: The bones of the inner ear are called the (a) Malleus
(hammer), (b) Incus (anvil) and (c) Stapes (stirrup). These bones function together to
transmit sound waves from the external environment to the fluid filled cochlea.
• Malleus (hammer): The malleus, or hammer, is a hammershaped bone that is
attached to the incus. It is attached to the inner surface of the eardrum and,
therefore, it moves as the eardrum vibrates in response to incoming sound.
• Incus (anvil): is an anvil-shaped bone in between the malleus and the stapes. It
is the bridge that connects the incoming sound waves to the inner ear.
• Stapes (stirrup): The stapes, or stirrup, transmits the sound vibrations from the
Incus to the oval window. The oval window connects the inner ear bones with the
cochlea.
Bones of the Chest
Clavicles (or collar bones) are long bones, which support the ribcage and shoulder
joints. The clavicles provide an attachment for the scapula and rotate when the arm is
26. moved forward. There are twelve ribs in the rib cage, 10 pairs that are joined to the
sternum and spine and 2 floating pairs. The ribs protect the underlying organs and
assist in respiration.
• Scapula: also known as the shoulder blade; it is a pair of broad flat bones that
connect the arm bone with the clavicle.
• Sternum: also known as the breastbone; it is a long flat bone in the center of the
chest. It connects to the ribs via cartilage and completes the rib cage. It has three
portions, from the top downward: (A)Manubrium, (B) Body and
(C) Xiphoid Process.
The Vertebral Column:
• Cervical: The cervical region is the first portion of the spinal column and is made
up of 7 vertebras. The first and second vertebrae are unique, and they are called
the atlas and the axis.
• Thoracic: The thoracic region of the vertebral column is located in the chest. It
contains 12 vertebrae and is connected to the lumbar region of the spine.
• Lumbar: The lumbar region of the vertebral column is the last main portion of the
vertebral column and is located in the lower back. It contains 5 vertebrae and is
connected to the pelvis, through the sacrum and coccyx.
• Sacrum: The sacrum is a triangular shaped bone that is made up of 5 fused
sacral vertebrae. It articulates with and provides a strong foundation for the
pelvis.
• Coccyx: The coccyx is also a triangular shaped bone that is made of 4 fused
coccygeal vertebrae, and is also known as the tailbone. It is attached to the
sacrum by cartilage, and this allows some movement between them and shock
absorbance.
SPINAL CORD
The spinal cord has two functions:
• Transmission of nerve impulses. Neurons in the white matter of the spinal cord
transmit sensory signals from peripheral regions to the brain and transmit motor
signals from the brain to peripheral regions.
• Spinal reflexes. Neurons in the gray matter of the spinal cord integrate incoming
sensory information and respond with motor impulses that control muscles
(skeletal, smooth, or cardiac) or glands.
The spinal cord is an extension of the brainstem that begins at the foramen magnum
and continues down through the vertebral canal to the first lumbar vertebra (L1). Here,
the spinal cord comes to a tapering point, the conus medullaris. The spinal cord is held
27. in position at its inferior end by the filum terminale, an extension of the pia mater that
attaches to the coccyx. Along its length, the spinal cord is held within the vertebral canal
by denticulate ligaments, lateral extensions of the pia mater that attach to the dural
sheath.
External features of the spinal cord:
• Spinal nerves emerge in pairs, one from each side of the spinal cord along its
length.
• The cervical nerves form a plexus (a complex interwoven network of nerves—
nerves converge and branch).
• The cervical enlargement is a widening in the upper part of the spinal cord (C4–
T1). Nerves that extend into the upper limbs originate or terminate here.
• The lumbar enlargement is a widening in the lower part of the spinal cord (T9–
T12). Nerves that extend into the lower limbs originate or terminate here.
• The anterior median fissure and the posterior median sulcus are two grooves that
run the length of the spinal cord on its anterior and posterior surfaces,
respectively.
• The cauda equina are nerves that attach to the end of the spinal cord and
continue to run downward before turning laterally to other parts of the body.
• There are four plexus groups: cervical, brachial, lumbar, and sacral.The thoracic
nerves do not form a plexus.
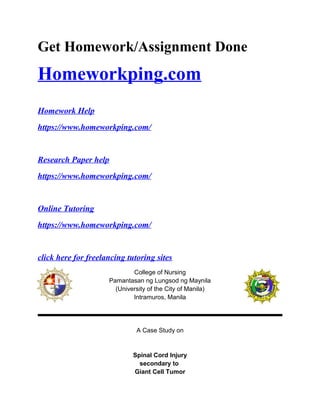
Figure 1. External features of the spinal cord.
28. Features of the cross section of the spinal cord:
• Roots are branches of the spinal nerve that connect to the spinal cord. Two
major roots form the following:
A ventral root (anterior or motor root) is the branch of the nerve that
enters the ventral side of the spinal cord. Ventral roots contain motor
nerve axons, transmitting nerve impulses from the spinal cord to skeletal
muscles.
A dorsal root (posterior or sensory root) is the branch of a nerve that
enters the dorsal side of the spinal cord. Dorsal roots contain sensory
nerve fibers, transmitting nerve impulses from peripheral regions to the
spinal cord.
A dorsal root ganglion is a cluster of cell bodies of a sensory nerve. It is
located on the dorsal root.
• Gray matter appears in the center of the spinal cord in the form of the letter H (or
a pair of butterfly wings) when viewed in cross section:
The gray commissure is the crossbar of the H.
29. The anterior (ventral) horns are gray matter areas at the front of each
side of the H. Cell bodies of motor neurons that stimulate skeletal
muscles are located here.
The posterior (dorsal) horns are gray matter areas at the rear of each
side of the H. These horns contain mostly interneurons that synapse with
sensory neurons.
The lateral horns are small projections of gray matter at the sides of H.
These horns are present only in the thoracic and lumbar regions of the
spinal cord. They contain cell bodies of motor neurons in the sympathetic
branch of the autonomic nervous system.
The central canal is a small hole in the center of the H crossbar. It
contains CSF and runs the length of the spinal cord and connects with
the fourth ventricle of the brain.
• White columns (funiculi) refer to six areas of the white matter, three on each side
of the H. They are the anterior (ventral) columns, the posterior (dorsal) columns,
and the lateral columns.
• Fasciculi are bundles of nerve tracts within white columns containing neurons
with common functions or destinations:
Ascending (sensory) tracts transmit sensory information from various parts
of the body to the brain.
Descending (motor) tracts transmit nerve impulses from the brain to
muscles and glands.
Figure 2. A cross section of the spinal cord.
31. SPINAL CORD INJURY SECONDARY TO GIANT CELL TUMOR
Predisposing and Precipitating factors
↓
Formation of giant cell tumor
↓
Production of chemoattractants
↓
Attraction of osteoclasts and osteoclast precursors
↓ ↓
Formation of lesions Further growth of the tumor
↓ ↓ ↓
Destruction of cortex Incrreased Pressure Palpable mass
↓ ↓
Irritation of the periosteum Spinal Cord Compression
↓ ↓
Weakening of the bone Spinal Cord Injury
↓ ↓
Pain in the site Limited Movement
XIII. DIAGNOSTIC PROCEDURES AND LABORATORY
32. Interpretation:
The significant increase in WBC may be due to the post decompression and
application of bone cements that the patient undergone last June 7, 2012. The body’s
compensation to weakened immunodefense brought about by the disease process may
also contribute to the significant increase of the WBC. It also means that the patient has
an existing infection. Decreased number of hemoglobin may indicate the existence of
anemia. Consistent decrease among the values of hemoglobin, hematocrit and RBC
may account from the diagnosed giant cell tumor. Slight decrease of hemoglobin,
hematocrit and RBC values may due to the chronic effect of the tumor that can manifest
anemia. Slight increase of neutrophil count may due to the malignant disease. Decrease
lymphocytes means that the patient is susceptible to infection. Anemia brought about by
Hematology 06-17-2012
Component Result Unit Normal Value Analysis
WBC 18.70 X 10 ^ 9 / L 4.50-11.0 Significant
increase
RBC 3.81 X 10 ^ 12 /L 4.6-6.2 Slight decrease
Hemoglobin 115 g / L 135-180 Slight decrease
Hematocrit 0.328 0.40-0.54 Slight decrease
Differential
Count:
Neutrophil 0.848 0.50-0.70 Slight increase
Lymphocyte 0.064 0.20-0.50 decrease
Monocyte 0.051 0.02-0.09 Normal
33. the malignant disease may contribute to the decreased lymphocyte count. Weaker
immunodefense brought about by the existing disease of the patient contributes to the
decreased lymphocyte count.
X.MEDICAL SURGICAL MANAGEMENT
34. The goal for the medical management of the patient is to control symptoms and
factors contributing to the patient’s condition.
1. Foley Catheter
Foley Catheter is a thin, sterile tube inserted in the bladder to drain urine.
It is also inserted to monitor the intake and output of the patient. It is also indicated
since the patient’s lower limbs don’t have a sensory and motor function thus the reason
for his immobility.
Nursing Considerations:
• Use strict aseptic technique for catheter insertion
• Minimize urethral trauma during insertion: use generous amount of lubricant
• Stabilize the catheter to minimize urethral trauma
• Maintain drainage bag below bladder level and tubing in dependent position to
facilitate urine flow
• Increase fluid intake
• Gently cleanse perineum and proximal catheter daily and after each bowel
movement
• Assess bowel function and implement measures to eliminate impaction or correct
constipation
2. Posterolateral Resection of the tumor
The posterolateral resection of the tumor is a surgical approach in
which the surgeon removes the tumor by working from the back and to the side. It is a
35. bone-sparing procedure which focuses on maintaining the structural stability of the
spine. It conserves anatomical structure during the removal of the tumor.
Nursing Considerations:
• Reinforce the health care provider’s explanations of the surgery and related
procedures
• Acquaint the patient with postoperative treatment devices, procedures, exercises
and other measures
• Provide routine preoperative nursing care
3. Diet
Diet as Tolerated
The patient was ordered a DAT when his appetite, ability to eat and
tolerance for certain foods changed. This means that the patient can tolerate all types of
foods and that he can have regular deserts and fluids as long as it is tolerated.
Nursing Considerations
• Offer patient assistance with hand washing and oral hygiene before and after a
meal
• Assist patient in a comfortable position
• Encourage patient to have a well-balanced food such as food high in protein,
carbohydrates, etc.
36. 4. Pharmacologic Therapy:
1. Caltrate (Calcium Carbonate)
Act as an activator in the transmission of nerve impulses and contraction
of cardiac, skeletal, and smooth muscle. It is essential for bone formation and
blood coagulation. It is also a replacement of calcium in deficiency states. And it
serves as a control of hyperphosphatemia in end-stage renal disease without
promoting aluminum absorption (calcium acetate).
Nursing Considerations:
• Explain to the patient the effect of the drug
• Monitor the vital signs of the patient especially blood pressure and pulse
rate
• Observe patient closely for symptoms of hypocalcemia(paresthesia,
muscle twitching, laryngospasm, colic, cardiac arrhythmias, Chvostek’s or
Trousseau’s sign
• Inspect abdomen; auscultate bowel sounds; assess for heartburn,
indigestion, and abdominal pain
• Monitor serum calcium or ionized calcium chloride, sodium, potassium,
magnesium, albumin, and parathyroid hormone (PTH) concentrations
before and periodically during therapy for treatment of hypocalcemia
• Monitor cardiac rate and rhythm closely
• Do not administer concurrently with foods containing large amounts of
oxalic acid(spinach, rhubarb), phytic acid(brans, cereals), or
phosphorus(milk or dairy products)
• Do not take within 1-2 hours of other medications if possible
37. • Advise patient to avoid excessive use of tobacco or beverages containing
alcohol or caffeine
2. Enoxaparin
It is a low molecular weight heparin with anticoagulant properties. It acts
by enhancing the inhibition rate of activated clotting factors including
thrombin and factor Xa through its action on antithrombin III.
Nursing Considerations:
• Explain to the patient the effect of the drug
• Administer medication through deep subcutaneous injections; do
not give by IM injection
• Apply pressure to all injection sites after needle is withdrawn; do
not massage the injection sites
• Inspect injection sites for hematoma
• Do not mix with other injections or infusions
• Check patient for signs of bleeding; monitor for blood tests
• Provide safety measures (electric razor, toothbrush) to prevent
injury to patient who is at risk for bleeding
38. XI. NURSING MANAGEMENT
• Monitor the patient’s vital signs
• Administer the prescribed medications on the right time, Exonaparin and Caltrate
• Assist client in repositioning self to avoid pressure ulcers
• Provide proper wound dressing.
• Assist in changing the urinary catheter
• Instruct in the use of side rails, overhead trapeze, roller pads for position
changes/transfer
• Encourage to support affected body parts using pillows, foot supports, air
mattress, water bed and so forth
39. • Provide regular skin care to include pressure area management.
• Encourage intake of fluids/nutritious foods.
• Encourage participation in recreational/social activities and hobbies appropriate
for situation.
• Provide proper health teaching regarding the client’s condition
40. XIV. NURSING CARE PLAN
Nursing Priority No. 1: Impaired physical mobility related to paralysis of the lower extremities
ASSESMENT DIAGNOSIS INFERENCE PLANNING INTERVENTION RATIONALE EVALUATION
OBJECTIVE:
Complete ASIA A
T12 level
(-) Motor
function
(-) Sensory
function
(+) Limited ROM
V/S taken as
follows:
T: 37.1 C
P: 91 cpm
Impaired
physical
mobility
related to
paralysis of the
lower
extremities
Giant cell tumor
Compression of
the T12
vertebrae
Modest back
pain
Tingling
sensation and
slight numbness
of the lower
After 8 hours
of nursing
interventions,
the patient
will
demonstrate
techniques or
behaviors that
would help
enable
resumption of
activity.
-Establish rapport
- Obtain vital
signs
-Assist with
passive ROM
exercises
-To develop a
therapeutic
nurse-patient
relationship and
a sense of trust
-To have a
baseline data
-Enhances
circulation,
restores muscle
tone and joint
mobility.
After 8 hours of
effective nursing
intervention,
goal was met
and
the patient was
able to
demonstrate
techniques or
behaviors that
would help
enable
resumption of
activity.
41. R: 19 bpm
BP: 120/90
mmHg
extremeties
Prolonged
compression
Hemiplegia
Impaired
Physical Mobility
-Do patient
turning
-Elevate lower
extremities at
intervals when in
chair or raise foot
or bed when
permitted in
individual
situation.
-Plan activities to
provide
uninterrupted
-Reduce the risk
of pressure
ulcers
-Reduce risk of
hypotension and
thrombus
formation.
-Prevents
fatigue,
allowing
opportunity for
44. Nursing Priority No. 2: Impaired skin integrity related to impaired sensation
ASSESSMENT DIAGNOSIS INFERENCE PLANNING INTERVENTIONS RATIONALE EVALUATION
Subjective:
“May nakita kong
parang pagbabalat
sa may paanan
ko”
Objective:
Disruption of the
skin surface
( - ) Sensation on
pain prick test
Impaired skin
integrity related
to impaired
sensation
Tumor
formation
Spinal cord
compression
Neurologic
deficits
Sensory nerve
Impairement
Inability to feel
pressure
formation
Increase in
pressure and
friction
After 8 hours of
nursing
intervention the
patient will
display improved
skin integrity and
prevent further
disruption
exacerbation of
skin lesions.
To determine
the cause
and extent of
skin lesions.
.
• Assess
sensation
through
pani prick
test.
• Perform
capillary
• Impaired
sensation
causes
inability of
to feel
impending
signs of
inflammati
on
After 8 hours
of nursing
intervention
the patient
had displayed
improved skin
integrity and
prevented
further
disruption
exacerbation
of skin
lesions.
45. Microcircultaio
n in the
capillaries
vasoconstrict
Decrease in
tissue
perfusion
Ischemia
Inflammation
Formation of
Decubitus ulce
refill
• Assess
skin.
Inspect and
palpate for
size shape,
turgor,
texture
temperature
and
characteristi
c of lesion.
• Measure
length,
width and
depth of the
lesion.
• .Check
blood
circulation.
• Provides
baseline
data and
assess the
extent of
the lesion
which
helps in
determinin
g what
type of
care shall
be
provided,
46. To assist
patient with
correcting
and
minimizing
extent of the
disease.
• Keep the
area clean
and dry,
aseptically
dress
wounds.
• Massage
the area to
stimulate
circulation
• Expose
lesion to air
• Dtermine
the
degree,
and depth
of injury, or
damage to
integument
ary
system.
• Prevent
further
complicatio
n
especially
infection.
47. and light if
excess
moisture is
impending
healing.
• Use paper
or tape or
nonadheren
t dressing
on frail skin.
Remove
slowly,
• Turn patient
every two
hours
• Assist
body’s
natural
process of
repair
through
promoting
adequate
blood
circulation.
• Maintai
n
appropr
iate
moistur
e
environ
ment to
promot
e fast
48. To promote
optimal
healing
through
continuous
care provided
by the
significant
others.
• Perform
passive
range of
motion.
.
• Reassess
skin on a
wound
healing.
• Impaire
d skin
can
easily
be
damag
ed
through
extensi
ve
contact.
• Facilitat
e blood
circulati
on and
49. To evaluate
the effects of
the care on
the patients
wound.
regular
schedule.
• Inform the
patient and
the
significant
other the
importance
of reporting
any
possible
lesion and
maintenanc
e of wound
hygiene
decrea
ses
injury
on
bony
promin
ences.
• Immobil
ity
predisp
oses
the
patient
to
further
skin
damag
e.
Assiste
d range
of
52. Nursing Priority No. 3: Disturbed body image related to paralysis of the lower extremities
53. Assessment Diagnosis Inference Planning Intervention Rationale Evaluation
SUBJECTIVE:
“Minsan
nakakahiya sa
kanila, lagi na
lang ako
inaasikaso” as
verbalized by
patient referring
to his family
members.
OBJECTIVE
Complete ASIA A
T12 level
(-) Motor
function
(-) Sensory
function
(+) Limited ROM
V/S taken as
follows:
T: 37.1 C
P: 91 cpm
Disturbed body
image related to
paralysis of the
lower
extremities
Giant cell
tumor
Compression
of the T12
vertebrae
Modest back
pain
Tingling
sensation and
slight
numbness of
the lower
extremeties
Prolonged
compression
After 4 hours of
nursing
interventions
patient will be
able to:
-verbalize
understanding of
body changes
-verbalize
acceptance of
self in situation
-verbalize relief
of anxiety and
adaptation to
altered body
image
-Establish rapport
with the patient
-Encourage
patient in
verbalization of
feeling and
thoughts about
self image
-Visit client
frequently and
acknowledge
patient as a
person
worthwhile
-Provide
assistance with
self care needs
--To develop
therapeutic
nurse-client
relationship and
a sense of trust
-To enhance
handling of
situations
-To develop a
sense of trust
-To provide
opportunities on
listening for
concerns
-To provide
assistance
After 4 hours of
effective nursing
interventions
patient, the goal
was met as
manifested by:
-verbalization of
understanding of
current body
changes
-verbalization of
acceptance of
self in situation
-verbalization
relief of anxiety
and adaptation
to altered self
image
54. XV. DRUG STUDY
Drug Mechanism of
action.
Contraindication Dosage Side effects Nursing
consideration
Analysis
Exonaparin
• Enoxaparin is
an
anticoagulant
(blood
thinner) that
prevents the
formation of
blood clots.
• used to treat
• acts by
enhancing the
inhibition rate
of activated
clotting
factors
including
thrombin and
factor Xa
through its
action on
• Cannot give to
patient with
hypersensitivity,
acute bacterial
endocarditis;
major bleeding
disorder,
haemorrhagic
stroke and drug-
induced
thrombocytopen
• 40mg/ml
OD 8am,
SQ
• Unusual heada
ches,
dizziness, or
weakness
• Unusual
bruising
(bruises that
develop without
known cause
or grow in size)
• Blood in the
• Lab tests:
Baseline
coagulation
studies;
periodic CBC,
platelet count,
urine and stool
for occult
blood.
• Monitor
• This drug is
indicated for
the patient to
prevent the
accumulation
of thrombosis
55. or prevent a
type of blood
clot called
deep vein
thrombosis
(DVT), which
can lead to
blood clots in
the lungs
(pulmonary
embolism)
antithrombin
III.
ia. urine
• Blood in the
stool (usually
seen as red or
black stools)
• Nosebleeds
• Bleeding gums
• Bleeding from
cuts that takes
a long time to
stop
• Coughing up
blood.
platelet count
closely.
Withhold drug
and notify
physician if
platelet count
less than
100,000/mm3.
• Monitor closely
patients with
renal
insufficiency
and older
adults who are
at higher risk
for
thrombocytope
nia.
• Monitor for
and report
immediately
any sign or
symptom of
unexplained
bleeding such
as: pink, red,
or dark brown
urine; red or
56. dark brown
vomitus;
bleeding gums
or bloody
sputum; dark,
tarry stools.
• Do not take
any OTC
drugs without
first consulting
physician.
Caltrate
• Calcium
carbonate is
used to
prevent and
to treat
calcium
deficiencies
• It is also used
as a dietary
supplement
where
calcium
intake may
be
inadequate.
• As dietary
supplements
to prevent or
treat negative
calcium
balance (eg,
osteoporosis),
the calcium in
calcium salts
moderates
nerve and
muscle
performance
and allows
• Can’t give to
patient with
hyperparathyroi
dism, vitamin D
overdosage,
decalcifying
tumors such as
plasmocytoma;
bone
metastases,
severe renal
disease and in
calcium loss
due to
immobilization.
• 50mg/1
tablet BID
PO.
• Nausea or
vomiting
• Decreased
appetite
• Constipation
• Dry mouth or
increase thirst.
• Urination more
than usual.
• Watch out for
severe
allergic
reaction such
as hives,
difficulty of
breathing and
swelling of
face, lips,
tongue and
throat.
• Take it with
food.
• Instruct
patient to
chew the
• Will serve as a
calcium
supplement to
the patient
because of
prolonged
immobility in
his lower
extremities
57. normal
cardiac
function.
tablet first
before
swallowing
it.
• Less intake
of whole
grain foods
as it may
decrease
calcium
absorption.
• Should be
administered
1-2 hours
before or
after iron
supplementa
tion as it
decrease
iron
absorption.
• Monitor
serum
calcium
levels.
58. XVII. Discharge Planning
The discharge planning is done before the client is discharged and aims to
ensure the continuity of care of the patient through identification, assessment, goal
setting, planning, implementation, coordination and evaluation while considering
contributing factors to the health of the patient, such as his significant others, lifestyle,
economic status.
Medication Educate the patient and family about the medications (purpose,
desired effects, adverse effects, dosage, administration
schedule, and precautions to be followed) and importance of
strict compliance to these medications. If signs and symptoms
worsen, tell patient to report these immediately to the
physician.
Exercise Teach patient and family members simple passive ROM
exercises to maintain good circulation and prevent
complications on immobility. Promote activity and exercise
within limits and adequate rest should be reinforced. Refer to
physical therapist for further information.
Treatment The focus of management is on recuperative and palliative
care of the patient. Adherence to treatment regimen is
reinforced to the patient and family about the medications, fluid
and passive ROM exercises, check- ups, and other
management directed to provide optimal functioning.
Health teaching Patient education is directed towards maintaining function of
movable parts and maintaining integrity over lower extremities.
59. Individual verbal and written instructions are provided to the
patient and family concerning medications, passive ROM
exercises. Teach also the importance of keeping follow-up
appointments and adherence to treatment regimen.
Out-patient
department
The importance of follow- up examinations and treatments are
stressed to the patient and family for further assessment on the
progress of the patient. Reminders about the need for health
promotion activities (hygiene, multiple dietary restrictions, etc)
are an important part of nursing care for the patient.
Diet Dietary intervention must be reviewed with the patient and
family members. Adequate caloric intake and vitamin
supplementation must be ensured.