American Society of Nephrology Presentation 2006
•
1 gostou•506 visualizações

This is a presentation given at the 2006 ASN Conference.
Recomendados

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (12)
Semelhante a American Society of Nephrology Presentation 2006
Semelhante a American Society of Nephrology Presentation 2006 (20)
Mais de Gary Abud Jr
Mais de Gary Abud Jr (19)
Último
Último (20)
American Society of Nephrology Presentation 2006
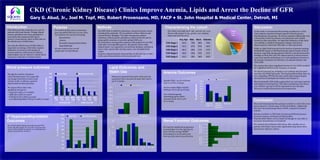
- 1. Lipid Outcomes and Statin Use Anemia Outcomes Blood pressure outcomes Introduction Discussion CKD (Chronic Kidney Disease) Clinics Improve Anemia, Lipids and Arrest the Decline of GFR Gary G. Abud, Jr., Joel M. Topf, MD, Robert Provenzano, MD, FACP • St. John Hospital & Medical Center, Detroit, MI Conclusion In this study we documented that during enrollment in a CKD clinic patients experienced improvement in blood pressure, hyperlipidemia and anemia. All of these patients additionally were concurrently treated by primary care physicians and variably treated by other specialists. An important limitation of this study was inability to attribute therapeutic changes and clinical improvement to either the CKD clinic or other physicians. While we didn’t find increased in the fraction of patients meeting K/DOQI BP targets we did find dramatic improvements in blood pressure, especially among patients with the worst blood pressure readings on their first visit. The improvements in blood pressure come from specific medications as we had significant increases in the fraction of patients on ß-blockers, Ca channel blockers and ACEi/ARB. The anemia data shows significant increase in use of ESA matched by a significant decline in the frequency of anemia. We found increased use of statins in our patients and increased meeting of K/DOQI lipid goals. The hyperparathyroidism data was less compelling. PTH did not show much improvement despite increased use of phosphorous binders and vitamin D. Most importantly GFR decline approached zero and many patients had improved renal function. This data is preliminary (less than a year of follow-up) and it will be important to trace this data forward to confirm that patients slow progression. This study demonstrated that patients enrolled in a CKD clinic have improvement in a broad range of CKD morbidities. Additionally they show decreased progression of CKD, compared to historic controls. Patients enrolled in a CKD clinic had decreased blood pressure, decreased anemia, and improved lipid profiles. Hyperparathyroidism was not improved though we were able to document intensification of treatment. We conclude that dedicated CKD clinics offer valuable care to patients with kidney disease that significantly helps them when measured by objective criteria. CKD clinics provide comprehensive care for patients with renal disease. Though clinical practice guidelines have been published to systematize the treatment CKD and to preserve renal function, there is little data on the effectiveness of CKD clinics. Knowing the effectiveness of CKD clinics is important as running a CKD clinic requires dedication of resources and changes in practice patterns; without proven efficacy nephrologists may be reticent to initiate them and payers reluctant to reimburse them. Anemia (Hgb<11g/dL) fell from 34% to 21% (P<0.0005). Severe anemia (Hgb<10g/dL) fell from 17% to 9% (p=0.002). Use of Erythropoietic stimulating agents (ESA) increased from 12% to 31% (P<0.0005). 0% 5% 10% 15% 20% 25% 30% SBP > 150 SBP > 160 SBP > 170 SBP > 180 DBP > 90 DBP > 100 DBP > 110 DBP > 120 SYSTOLIC BP DIASTOLIC BP First Visit Most Recent Visit %ofPatients Statin use increased from 53% to 60% and was associated with a decrease in mean LDL (106 to 95, P<0.0005). %ofPatients %ofPatients Purpose We undertook this study to determine how successful CKD care is in our clinic. We looked at our success in treating: We also looked at the overall progression of renal disease. Hypertension Anemia Secondary hyperparathyroidism Hyperlipidemia Methods Our CKD clinic is staffed by physicians, advanced practice nurses and physician assistants. We see patients at three clinics in and around Detroit, Michigan. The clinic incorporates patient education, clinical practice guidelines, anemia protocols and on going quality assurance to provide optimal CKD care. We performed a retrospective analysis of the patients in our CKD clinic after receiving IRB approval. All patients whose entire clinical history was captured in an electronic database, and had at least 2 visits, greater than 30-days apart, were included in the cohort. Analysis compared patient characteristics on the first day of clinic to the same characteristics on the most recent visit. Though the number of patients whose blood pressure was at goal did not change from first to most recent visit (p=0.08), we did see a general improvement in blood pressure. We suspect this is due to the significant increase in: • loop (43 to 55%, p=<0.0005) • ARB (23 to 28%, p=0.027) • ß-blockers (62 to 66% p=0.032) • non-dihydropyridine CCB (31 to 36% p=0.025) 2º Hyperparathyroidism Outcomes 0% 2% 4% 6% 8% 10% 12% 14% 16% 18% First Visit Most Recent Visit Characterizing the cohort The cohort was made up of 336 patients who were diverse with respect to age, gender, race, diabetic status and renal function. Avg. Age Male Black Diabetes CKD Stage 1 54.6 75% 50% 75% CKD Stage 2 53.2 67% 67% 44% CKD Stage 3 66.5 60% 31% 47% CKD Stage 4 69.8 53% 27% 41% CKD Stage 5 63.5 49% 49% 40% Active Vit. D Calcitriol Hectorol Phos Binder On arrival to clinic patients generally had good PTH levels, with 58% at goal. We were able to increase that only to 64% primarily through the use of phosphorous binders and activated vitamin D. Renal Function Outcomes We found no significant progression of renal failure over the 256 days in clinic with the average MDRD decreasing by 0.19 mL/min/year from 32.5 mL/min to 32.3 mL/min.