
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a SLIPPED CAPITAL FEMORAL EPIPHYSIS - By Dr. Lokesh Sharoff
Semelhante a SLIPPED CAPITAL FEMORAL EPIPHYSIS - By Dr. Lokesh Sharoff (20)
Mais de Lokesh Sharoff
Último
Último (20)
SLIPPED CAPITAL FEMORAL EPIPHYSIS - By Dr. Lokesh Sharoff
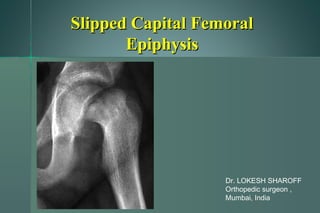
- 1. Slipped Capital FemoralSlipped Capital Femoral EpiphysisEpiphysis Dr. LOKESH SHAROFF Orthopedic surgeon , Mumbai, India
- 2. IncidenceIncidence Annual incidence 2-10 per 100,000Annual incidence 2-10 per 100,000 2.4 M : 1 F2.4 M : 1 F LEFT > RIGHT HIPLEFT > RIGHT HIP Boys 13-15 yrs (14)Boys 13-15 yrs (14) Girls 11-13 yrs (12)Girls 11-13 yrs (12) presentation outside these ages consider endocrine orpresentation outside these ages consider endocrine or systemic disorder !!systemic disorder !!
- 3. IntroductionIntroduction Obese (50-75% over 95thObese (50-75% over 95th centile)centile) Delay in skeletal maturityDelay in skeletal maturity Bilateral in 17% (50%Bilateral in 17% (50% present-50% sequential)present-50% sequential)
- 4. IntroductionIntroduction femoral neck displace ANTERIORLY ANDfemoral neck displace ANTERIORLY AND SUPERIORLY with the head in the acetabulum causing anSUPERIORLY with the head in the acetabulum causing an apparent varus deformityapparent varus deformity
- 5. AetiologyAetiology Mechanical factorsMechanical factors obesityobesity Increase in femoral retroversionIncrease in femoral retroversion Vertically oriented physeal plateVertically oriented physeal plate Thinning of perichondral ringThinning of perichondral ring
- 6. AetiologyAetiology InflammatoryInflammatory synovial hyperplasiasynovial hyperplasia increase in IG and C3increase in IG and C3
- 7. AetiologyAetiology EndocrineEndocrine Association withAssociation with Hypothyroidism Primary hyperparathyroidism Panhypopituitarism Hypogonadal conditions Renal osteodystrophy GH deficiency and therapy Rubenstein - taybi syndrome Klinefelters syndrome
- 8. PathologyPathology -Periosteum torn anteriorly-Periosteum torn anteriorly -Antero-superior part of neck forms a rounded-Antero-superior part of neck forms a rounded humphump -area between neck and periosteum posteriorly is-area between neck and periosteum posteriorly is filled with osseous tissuefilled with osseous tissue
- 9. HistopathologyHistopathology -PRE SLIP STAGE - widening of physis-PRE SLIP STAGE - widening of physis -DISPLACEMENT - occurs through Proliferative-DISPLACEMENT - occurs through Proliferative and Hypertrophic zonesand Hypertrophic zones -organisation of chondrocytes changes from-organisation of chondrocytes changes from columnar to clumpscolumnar to clumps
- 10. Slipped Capital FemoralSlipped Capital Femoral Epiphysis classificationEpiphysis classification According to duration of symptoms--According to duration of symptoms-- Preslip: synovitisPreslip: synovitis Acute <3wksAcute <3wks Chronic >3 wksChronic >3 wks Acute on Chronic >3 wks with furtherAcute on Chronic >3 wks with further displacement of epiphysisdisplacement of epiphysis
- 11. Slipped Capital FemoralSlipped Capital Femoral Epiphysis PresentationEpiphysis Presentation Physeal stability– Loder classificationPhyseal stability– Loder classification Stable: can wt bearStable: can wt bear Unstable : cannot wt. bearUnstable : cannot wt. bear Acute Slipped Capital Femoral Epiphysis: the Importance of Physeal StabilityAcute Slipped Capital Femoral Epiphysis: the Importance of Physeal Stability Loder et alLoder et al JBJS 1993; 75-A:1134-1140JBJS 1993; 75-A:1134-1140
- 12. Presentation--chronicPresentation--chronic -often obese and present with pain in the hip (85%) or knee (15%)-often obese and present with pain in the hip (85%) or knee (15%) —increases in evening or after exertion—increases in evening or after exertion -Limp-Limp -thigh atrophy-thigh atrophy -extremity shortening-extremity shortening Knee Axilla sign: On attempted flexion of the hip, the patients legKnee Axilla sign: On attempted flexion of the hip, the patients leg goes into external rotationgoes into external rotation Internal rotation is lost.Internal rotation is lost. Abduction and extension is also restrictedAbduction and extension is also restricted
- 13. Presentation—acute on chronicPresentation—acute on chronic -sudden onset of pain-sudden onset of pain -unable to move the limb-unable to move the limb -unable to bear weight-unable to bear weight -limb in external rotation-limb in external rotation
- 14. Presentation --ChondrolysisPresentation --Chondrolysis -Pain is continous-Pain is continous -Pain throughout ROM-Pain throughout ROM -Global restriction of ROM-Global restriction of ROM -Flexion contracture-Flexion contracture
- 15. Slipped Capital FemoralSlipped Capital Femoral Epiphysis RadiologyEpiphysis Radiology APAP Physeal wideningPhyseal widening Steels Metaphyseal Blanch sign (density in neck)Steels Metaphyseal Blanch sign (density in neck) Klein line/Trethowan signKlein line/Trethowan sign Schams signSchams sign Break in Shenton’s lineBreak in Shenton’s line
- 16. RadiologyRadiology --Klein's Line:--Klein's Line: – line drawn along superior border of femoral neck shouldline drawn along superior border of femoral neck should cross at least a portion of the femoral epiphysiscross at least a portion of the femoral epiphysis – slip must be suspected if a straight line drawn up lateralslip must be suspected if a straight line drawn up lateral surface of femoral neck does not touch the femoral headsurface of femoral neck does not touch the femoral head
- 17. RadiologyRadiology Metaphyseal blanch sign (STEELS)---Metaphyseal blanch sign (STEELS)---
- 18. RadiologyRadiology SCHAMS sign --SCHAMS sign -- The posterior acetabular margin normally cutsThe posterior acetabular margin normally cuts the medial corner of the metaphysis. In slip the whole metaphysisthe medial corner of the metaphysis. In slip the whole metaphysis remains lateral to the acetabular margin.remains lateral to the acetabular margin.
- 19. Slipped Capital FemoralSlipped Capital Femoral Epiphysis RadiologyEpiphysis Radiology LateralLateral Shoot-through/Frog legShoot-through/Frog leg It shows the bending of the femoral neck and theIt shows the bending of the femoral neck and the anterior hump of bone growthanterior hump of bone growth head-shaft angle of SOUTHWICK can be calculatedhead-shaft angle of SOUTHWICK can be calculated
- 20. RadiologyRadiology SOUTHWICK’SSOUTHWICK’S CLASSIFICATIONCLASSIFICATION calculate the Head-Shaft anglecalculate the Head-Shaft angle <30--mild<30--mild 30-60--moderate30-60--moderate >60--severe>60--severe
- 21. Slipped Capital FemoralSlipped Capital Femoral Epiphysis RadiologyEpiphysis Radiology Classification—Classification— Determined by percentage of displacement of theDetermined by percentage of displacement of the EPIPHYSIS in relation to the neck, as follows:EPIPHYSIS in relation to the neck, as follows: grade I (<33%),grade I (<33%), grade II (33-50%),grade II (33-50%), grade III (>50%)grade III (>50%)
- 22. Slipped Capital FemoralSlipped Capital Femoral Epiphysis TreatmentEpiphysis Treatment Prevent further slippagePrevent further slippage Reduce the degree of slippageReduce the degree of slippage Salvage treatmentSalvage treatment
- 23. CT--SCANCT--SCAN --To check HEAD – NECK angle--To check HEAD – NECK angle --Neck in ante or retroversion--Neck in ante or retroversion --post-op—whether implant has penetrated into--post-op—whether implant has penetrated into the jointthe joint --closure of physis--closure of physis --compression achieved by screws--compression achieved by screws --residual deformity--residual deformity
- 24. ULTRASOUNDULTRASOUND --to check for joint effusion--to check for joint effusion --to check for step between femoral neck and--to check for step between femoral neck and epiphysisepiphysis
- 25. MRIMRI --used to asses the pre-slip stage but is expensive--used to asses the pre-slip stage but is expensive
- 26. BONE SCANBONE SCAN --Increased uptake in SCFE--Increased uptake in SCFE --decreased uptake in AVN--decreased uptake in AVN --increased in the joint space in chondrolysis--increased in the joint space in chondrolysis
- 27. SCFE Treatment to preventSCFE Treatment to prevent further slippagefurther slippage Hip spicaHip spica Bone peg epiphysiodesisBone peg epiphysiodesis Pin or screw fixationPin or screw fixation
- 28. SCFE Treatment to preventSCFE Treatment to prevent further slippagefurther slippage THEORIESTHEORIES --smooth pins– to allow epiphysial growth--smooth pins– to allow epiphysial growth --threaded pins –to arrest physeal growth--threaded pins –to arrest physeal growth --single cannulated screw—threads placed across--single cannulated screw—threads placed across physis to arrest growthphysis to arrest growth --double screws—for additional rotational stability--double screws—for additional rotational stability in unstable hipsin unstable hips
- 29. SCFE Treatment to preventSCFE Treatment to prevent further slippagefurther slippage In situ screw or pin fixationIn situ screw or pin fixation biplane fluoroscopybiplane fluoroscopy percutaneous techniquepercutaneous technique Position fixation centrally in headPosition fixation centrally in head
- 30. SCFE Treatment to preventSCFE Treatment to prevent further slippagefurther slippage In situ screw or pin fixation--positionIn situ screw or pin fixation--position pin must be placed perpendicular to plane of the femoral headpin must be placed perpendicular to plane of the femoral head starting position anterior of the femoral neck and not lateralstarting position anterior of the femoral neck and not lateral cortexcortex
- 31. SCFE Treatment to preventSCFE Treatment to prevent further slippagefurther slippage In situ screw or pin fixation—to avoidIn situ screw or pin fixation—to avoid avoid superior and anterior quadrant of femoral headavoid superior and anterior quadrant of femoral head following fixation whilst moving hip to ensure no penetrationfollowing fixation whilst moving hip to ensure no penetration
- 32. SCFE Treatment to preventSCFE Treatment to prevent further slippagefurther slippage --BONE GRAFT EPIPHYSIODESIS--BONE GRAFT EPIPHYSIODESIS Advantages—rapid epiphysial closureAdvantages—rapid epiphysial closure ---no risk of implant penetration into jt.---no risk of implant penetration into jt. ---no reoperation---no reoperation Disadvantages---infectionDisadvantages---infection ---chondrolysis---chondrolysis ---avn---avn Uses --- in failed pinning operationUses --- in failed pinning operation
- 33. SCFE Treatment to ReduceSCFE Treatment to Reduce degree of slippagedegree of slippage Closed manipulationClosed manipulation although after in situ pinning ROM improves this is inalthough after in situ pinning ROM improves this is in main due to resolution of synovitis and spasm.main due to resolution of synovitis and spasm. There is little remodellingThere is little remodelling Closed manipulation >24hrs significantly increases theClosed manipulation >24hrs significantly increases the risk of osteonecrosisrisk of osteonecrosis
- 34. SCFE Treatment to ReduceSCFE Treatment to Reduce degree of slippagedegree of slippage OsteotomiesOsteotomies -- to reduce deformity-- to reduce deformity --to prevent further slipping--to prevent further slipping --to re-orient and stabilise physis--to re-orient and stabilise physis
- 35. SCFE Treatment to preventSCFE Treatment to prevent further slippagefurther slippage OsteotomiesOsteotomies 1–-dunn’s1–-dunn’s 2—kramer2—kramer 3—barmada3—barmada 4---southwick4---southwick
- 36. SCFE Treatment to ReduceSCFE Treatment to Reduce degree of slippagedegree of slippage OsteotomiesOsteotomies more distal less correction at primary site of deformitymore distal less correction at primary site of deformity more proximal more risk of osteonecrosismore proximal more risk of osteonecrosis used in cases of moderate to severe slipsused in cases of moderate to severe slips
- 37. SCFE Treatment to ReduceSCFE Treatment to Reduce degree of slippagedegree of slippage OsteotomiesOsteotomies Cuneiform Osteotmy at femoralCuneiform Osteotmy at femoral physis Fish/ Dunnphysis Fish/ Dunn --done in severe slips in open--done in severe slips in open physisphysis Osteonecrosis 12-35%Osteonecrosis 12-35% Fish 3.5% osteonecrosis and 11%Fish 3.5% osteonecrosis and 11% chondrolysischondrolysis
- 39. Intertrochanteric - SouthwickIntertrochanteric - Southwick Compensatory osteotomy, the more distal the lessCompensatory osteotomy, the more distal the less correction at primary source of deformity.correction at primary source of deformity. Maximum head-shaft correction is 50Maximum head-shaft correction is 50°.°. Antero-lateral wedge is removed,so flexion and valgus ofAntero-lateral wedge is removed,so flexion and valgus of distal fragment is achieved .distal fragment is achieved . Wedge removed -- therefore shorteningWedge removed -- therefore shortening.. Done in severe slipsDone in severe slips
- 40. SCFE Treatment to ReduceSCFE Treatment to Reduce degree of slippagedegree of slippage OsteotomiesOsteotomies IntertrochantericIntertrochanteric single, bi or multiple-planesingle, bi or multiple-plane corrects 45’-50’corrects 45’-50’ low incidence oflow incidence of osteonecrosis, butosteonecrosis, but chondrolysis rate 6-50%chondrolysis rate 6-50%
- 41. SCFE Treatment to ReduceSCFE Treatment to Reduce degree of slippagedegree of slippage OsteotomiesOsteotomies Base of neck—Base of neck— KRAMER ANDKRAMER AND BARMADABARMADA anterior wedgeanterior wedge removedremoved corrects 30-50corrects 30-50 for chronic residualfor chronic residual deformitiesdeformities moderate to severe scfemoderate to severe scfe
- 42. SCFE Prophylactic pinning of theSCFE Prophylactic pinning of the contralateral hipcontralateral hip FU till skeletal maturityFU till skeletal maturity Pin if symptoms presentPin if symptoms present Pin knownPin known metabolic/endocrinemetabolic/endocrine disordersdisorders Pin if FU unreliablePin if FU unreliable
- 43. SCFE OsteonecrosisSCFE Osteonecrosis vascular injury, complication of treatmentvascular injury, complication of treatment increase with severity of slipincrease with severity of slip increase in acute, unstable slipsincrease in acute, unstable slips increases with manipulation, pin placement in superior quadrantincreases with manipulation, pin placement in superior quadrant
- 44. SCFE OsteonecrosisSCFE Osteonecrosis remove metal workremove metal work maintain ROMmaintain ROM shelf acetabuloplastyshelf acetabuloplasty arthrodesis/THRarthrodesis/THR
- 45. SCFE ChondrolysisSCFE Chondrolysis dissolution of articular cartilage with jointdissolution of articular cartilage with joint stiffness and painstiffness and pain CauseCause synovial malnutrition, ischaemia, excessive pressuresynovial malnutrition, ischaemia, excessive pressure AutoimmuneAutoimmune Females>malesFemales>males
- 46. SCFE ChondrolysisSCFE Chondrolysis incidence 2-20%incidence 2-20% higher in females, acute and severe slipshigher in females, acute and severe slips manipulation, prolonged immobilisation, realignmentmanipulation, prolonged immobilisation, realignment osteotomiesosteotomies pin penetrationpin penetration exclude infectionexclude infection
- 47. SCFE ChondrolysisSCFE Chondrolysis Non- wt bearing, NSAID, ROMNon- wt bearing, NSAID, ROM tractiontraction in pt therapyin pt therapy