Abdominal Aortic Aneurysm Nursing Care Plan and Management
•
16 gostaram•18,668 visualizações

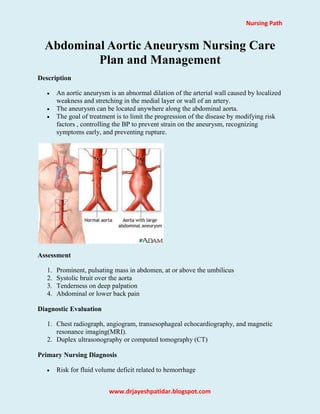
An aortic aneurysm is an abnormal dilation of the arterial wall caused by localized weakness and stretching in the medial layer or wall of an artery.

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Abdominal Aortic Aneurysm Nursing Care Plan and Management
Semelhante a Abdominal Aortic Aneurysm Nursing Care Plan and Management (20)
Mais de Nursing Path
Mais de Nursing Path (20)
Último
Último (20)
Abdominal Aortic Aneurysm Nursing Care Plan and Management
- 1. Nursing Path www.drjayeshpatidar.blogspot.com Abdominal Aortic Aneurysm Nursing Care Plan and Management Description An aortic aneurysm is an abnormal dilation of the arterial wall caused by localized weakness and stretching in the medial layer or wall of an artery. The aneurysm can be located anywhere along the abdominal aorta. The goal of treatment is to limit the progression of the disease by modifying risk factors , controlling the BP to prevent strain on the aneurysm, recognizing symptoms early, and preventing rupture. Assessment 1. Prominent, pulsating mass in abdomen, at or above the umbilicus 2. Systolic bruit over the aorta 3. Tenderness on deep palpation 4. Abdominal or lower back pain Diagnostic Evaluation 1. Chest radiograph, angiogram, transesophageal echocardiography, and magnetic resonance imaging(MRI). 2. Duplex ultrasonography or computed tomography (CT) Primary Nursing Diagnosis Risk for fluid volume deficit related to hemorrhage
- 2. Nursing Path www.drjayeshpatidar.blogspot.com Other Diagnoses that may occur in Nursing Care Plans For Abdominal Aortic Aneurysm Acute pain related to surgical tissue trauma Anxiety related to threat to health status Decreased cardiac output related to: o changes in intravascular volume o increased systemic vascular resistance o third-space fluid shift Deficient knowledge (preoperative and postoperative care) related to newly identified need for aortic surgery Ineffective breathing pattern related to: o effects of general anesthesia o endotracheal intubation o presence of an abdominal incision Medical Management Medical or surgical treatment depends on the type of aneurysm. For a rupture aneurysm, prognosis is poor and surgery is performed immediately. When surgery can be delayed, medical measures include: Strict control of blood pressure and reduction in pulsatile flow. Systolic pressure maintained at 100 to 120 mm Hg with antihypertensive drugs, such as nitroprusside. Pulsatile flow reduced by medications that reduce cardiac contractility, such as propanolol. Surgical Management Removal of the aneurysm and restoration of vascular continuity with a graft (resection and bypass graft or endovascular grafting) is the goal of surgery and the treatment of choice for abdominal aortic aneurysms larger than 5.5 cm (2 inches) in diameter or those that are enlarging. Intensive monitoring in the critical care unit is required. Nonsurgical Intervention 1. Modify risk factors. 2. Instruct the client regarding the procedure for monitoring BP. 3. Instruct the client on the importance of regular physician visits to follow the size of the aneurysm.
- 3. Nursing Path www.drjayeshpatidar.blogspot.com 4. Instruct the client that if severe back or abdominal pain or fullness, soreness over the umbilicus, sudden development of discoloration in the extremities, or a persistent elevation of BP occurs to notify the physician immediately. 5. Instruct the client with a thoracic aneurysm to report immediately the occurrence of chest or back pain, shortness of breath, difficulty swallowing, or hoarseness. Pharmacologic Highlights 1. 1-10 mg IV of opioid analgesic (morphine) to relieve surgical pain. 2. 50–100 mcg IV of opioid analgesic (Fentanyl) to relieve surgical pain. 3. Antihypertensives and/or diuretics for rising BP may stress graft suture lines. 4. 80-400 mg/day in divide doses of Beta blocker (propanolol) to use in people with small aneurysms without risk for rupture; decreases rate of AAA expansion Nursing Intervention 1. Monitor vital signs. 2. Assess risk factors for the arterial disease process. 3. Obtain information regarding back or abdominal pain. 4. Question the client regarding the sensation of palpation in the abdomen. 5. Inspect the skin for the presence of vascular disease or breakdown. 6. Check peripheral circulation, including pulses,temperature, and color. 7. Observe for signs of rupture. 8. Note any tenderness over the abdomen. 9. Monitor for abdominal distention. Documentation Guidelines Location,intensity,and frequency of pain,and the factors that relieve pain Appearance of abdominal wound (color,temperature,intactness,drainage) Evidence of stability of vital signs,hydration status,bowel sounds,electrolytes Presence of complications: Hypotension, hypertension, cardiac dysrhythmias, low urine out- put,thrombophlebitis,infection,graft occlusion,changes in consciousness,aneurysm rupture, excessive anxiety,poor wound healing Discharge and Home Healthcare Guidelines 1. Wound care. Explain the need to keep the surgical wound clean and dry. Teach the patient to observe the wound and report to the physician any increased swelling,redness,drainage,odor,or separation of the wound edges. Also instruct the patient to notify the physician if a fever develops. 2. Activity restriction. Instruct the patient to lift nothing heavier than 5 pounds for about 6 to 12 weeks and to avoid driving until her or his physician permits.
- 4. Nursing Path www.drjayeshpatidar.blogspot.com Braking while driving may increase intra-abdominal pressure and disrupt the suture line. Most surgeons temporarily discourage activities that require pulling, pushing, or stretching—activities such as vacuuming,changing sheets,playing tennis and golf,mowing grass,and chopping wood. 3. Smoking cessation. Encourage the patient to stop smoking and to attend smoking cessation classes. 4. Complications following surgey. Discuss with the patient the possibility of clot formation or graft blockage. 5. Complicatios for patients not requiring surgery. Compliance with the regime of monitoring the size of the aneurysm by computed tomography over time is essential. The patient needs to understand the prescribed medication to control hypertension. Advise the patient to report abdominal fullness or back pain,which may indicate a pending rupture.