
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Wilms tumor
Semelhante a Wilms tumor (20)
Mais de GAURAV NAHAR
Último
Último (20)
Wilms tumor
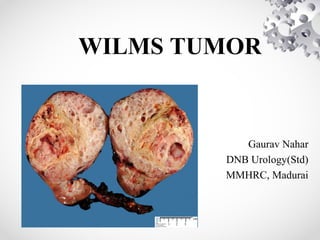
- 1. WILMS TUMOR Gaurav Nahar DNB Urology(Std) MMHRC, Madurai
- 2. INTRODUCTION • Wilms tumor - Nephroblastoma. • Most common primary malignant renal tumor of childhood. • This embryonal tumor develops from remnants of immature kidney.
- 3. EPIDEMIOLOGY • Accounts for 6% to 7% of all childhood cancers. • Children<15 yrs: annual incidence rate 7 to 10 cases per million. • More than 80% of cases are diagnosed before 5 years of age, with a median age of 3.5 years.
- 4. • B/L Wilms tumors present at earlier age. • Incidence lower in East Asian populations & higher in black populations compared with North American and European whites. • Environmental risk factors play a minor role.
- 5. ETIOLOGY • Majority of Wilms tumors arise from somatic mutations restricted to tumor tissue. • A much smaller percentage originate from germline mutations. • Several genetic events result in Wilms tumor development.
- 6. • 10% tumors- have coexistent congenital anomalies and syndromes. • 5% to 10% tumors- bilateral/multicentric. • 1% to 2% are familial.
- 8. WT1: • 1st Wilms tumor gene to be identified. • Gross deletions at chromosome 11p13. • Associated syndromes: 1.WAGR syndrome 2.Denys-Drash syndrome 3.Frasier syndrome
- 9. • WT1 gene is important for normal kidney & gonadal development. • WT1 encodes a zinc-finger transcription factor expressed in kidney, gonads, spleen, & mesothelium • WT1 is necessary for ureteric bud outgrowth and nephrogenesis.
- 10. • WAGR (Wilms tumor, Aniridia, Genital anomalies, mental Retardation) syndrome. • Aniridia, found in 1.1% of Wilms tumor patients, is caused by an abnormality of the PAX6 gene located adjacent to WT1. • Wilms tumor develops in 40% to 70% of aniridia patients with deletions of WT1.
- 11. • Denys-Drash syndrome (DDS): specific association of male pseudohermaphroditism, renal mesangial sclerosis, and nephroblastoma. • Caused by point mutations in zinc finger DNA binding region of WT1. • >90% of DDS patients harbor germline point mutations in only one WT1 allele.
- 12. • WAGR and DDS patients- more likely to have bilateral tumors & are diagnosed at a younger age. • WAGR patients- increased risk of renal failure if they survive into puberty. • Genitourinary anomalies- renal fusion anomalies, cryptorchidism, hypospadias are present in 4.5% of patients with Wilms tumor.
- 13. WT2: • 11p15 locus- LoH(Loss of Heterozygosity) a/w Beckwith-Wiedemann Syndrome. • Genes involved- H19 & IGF-2.
- 14. • Beckwith-Wiedemann syndrome(BWS) characterized by excess growth at cellular, organ (macroglossia, nephromegaly, hepatomegaly), or body segment (hemihypertrophy) levels. • Adrenocortical neoplasms and hepatoblastoma also occur in BWS. • Most cases sporadic; 15% heritable- AD.
- 15. WTX: • Tumor suppressor gene, Wilms Tumor gene on the X chromosome, at Xq11.1, • Inactivated in up to one third of Wilm's tumors. • Targets single X chromosome in males & active X chromosome in females with tumors.
- 16. Familial Wilm's Tumor : (FWT1, FWT2) • 1% to 2% of Wilms tumor patients have a family h/o Wilms tumor. • Earlier age of onset & increased frequency of B/L disease.
- 17. • TP53 mutations- increased frequency in anaplastic histology. • LoH at 1p and 16q are associated with an increased risk of tumor relapse and death.
- 18. SCREENING • Ultrasound surveillance- from time of diagnosis until 5 years of age, with a frequency of every 3 to 4 months. • BWS, Simpson-Golabi-Behmel, and familial Wilms- continue to 7 years. • Screening recommended when WT incidence > 5%. • Screening of contralateral kidney after nephrectomy for U/L Wilm's.
- 19. • CT or MRI if USG shows any suspicious lesion. • 7-fold increased risk of Wilm's tumor in HK. • an increased risk of müllerian duct anomalies in girls with Wilms tumor- Approx.10% girls will have abnormalities, such as duplication of cervix or uterus, or bicornuate uterus.
- 20. PATHOLOGY Favorable-Histology Wilms Tumor(FH): • Wilms tumor compresses adjacent normal renal parenchyma, forming an "intrarenal pseudocapsule." • Tremendous histologic diversity. • 90% of all renal tumors have favorable histology.
- 21. • “Classical” Wilms tumor is characterized by islands of compact undifferentiated blastema, presence of variable epithelial differentiation in the form of embryonic tubules, rosettes, and glomeruloid structures, separated by a significant stromal component.
- 23. • Predominantly epithelial differentiation- low degree of aggressiveness, majority are stage I tumors, • But may be more resistant to therapy, if they present as advanced-stage disease.
- 24. Survival Rates in Patients with Favorable-Histology Wilms Tumor
- 25. Anaplastic Wilms Tumor: • Anaplasia is characterized by the presence of three abnormalities: 1.nuclear enlargement to three or more times the diameter of adjacent cells, 2.hyperchromasia of enlarged nuclei, and 3.abnormal mitotic figures. • Rarely seen in children< 3 years.
- 26. • Resistant to chemotherapy. • Poor prognosis. • Further divided into focal & diffuse patterns.
- 27. Nephrogenis Rests: • Precursor lesions; still most don't form Wilm's tumor. • A rest can undergo maturation, sclerosis, involution, or complete disappearance. • Two types based on location: Perilobar & Intralobar(PLNRs & ILNRs).
- 28. • Perilobar NRs- found only in the lobar periphery, elaborated late in embryogenesis. • Subcortical, sharply demarcated, and contain predominantly blastema & tubules. • Usually found in BWS, linked to 11p15 locus.
- 29. • Intralobar NRs found anywhere within the lobe, renal sinus and wall of PCS. • Result of earlier gestational aberrations. • ILNRs are commonly stroma rich. • Typically seen in aniridia, WAGR, DDS or other features a/w WT1.
- 31. CLINICAL PRESENTATION • A palpable smooth abdominal mass- 90%. Incidentally discovered. • Abdominal pain, gross hematuria & fever- less frequent. • Tumor rupture with hemorrhage into peritoneal cavity- mimics acute abdomen. • Extension into renal vein & IVC- varicocoele, hepatomegaly due to hepatic vein obstruction, ascites, and congestive heart failure- <10%.
- 32. • Hypertension- common at diagnosis, d/t elevated plasma renin levels; resolves shortly after removal. • Acquired von Willebrand disease found in 8% of newly diagnosed Wilms tumor.
- 33. IMAGING • FOUR FIELD CHEST RADIOGRAPHY: may show lung metastasis. RENAL ULTRASOUND: 1st study to evaluate child with abd.mass. demonstrate solid nature of the lesion. Doppler USG helps to exclude intracaval tumor extension, & its proximal extent.
- 34. Solid renal tumor: CT demonstrates that lesion is amenable to renal-sparing surgery
- 35. • CT SCAN: helps to determine origin of the tumor, lymph node involvement, B/L kidney involvement, invasion into major vessels (IVC), and liver metastases. CT chest to rule out lung metastasis.
- 36. CT scan of a left Wilms tumor with a small rim of functioning renal parenchyma
- 37. • MRI ABDOMEN: Most sensitive imaging modality for caval patency, to determine tumor extension into IVC. low signal intensity on T1-weighted images and high signal intensity on T2-weighted images.
- 38. MRI depicting extension of Wilms tumor into the inferior vena cava.
- 39. STAGING
- 40. DIFFERENTIAL DIAGNOSIS • Mesoblastic nephroma - Most common renal tumor in the first month of life. • Renal cell carcinoma • Clear cell sarcoma of the kidney • Rhabdoid tumor of the kidney • Nonmalignant mass • Hydronephrosis • Multicystic kidney disease • Renal cyst • Renal thrombosis • Dysplastic kidney • Renal hemorrhage
- 41. • Differential Diagnoses • Neuroblastoma • Polycystic Kidney Disease • Rhabdomyosarcoma
- 42. PROGNOSTIC FACTORS • Most Important determinants of outcome: histopathology & tumor stage. • Chromosomal Abnormalities: LOH for chromosome 16q and/or 1p (20% of Wilms tumors) a/w increased risk for relapse & death. • High telomerase activity- an unfavourable prognostic feature. • DNA Content: Aneuploidy & DNA index . 1.5- strongly a/w anaplastic histology. • Cytokines: VEGF angiogenic cytokine.
- 43. TREAMENT • Usual approach- nephrectomy followed by chemotherapy, with or without postoperative radiotherapy. • Multiple RCTs to determine therapeutic protocols by: 1. National Wilm's Tumor Study Group/Children's Oncology Group(NWTSG/COG), 2. International Society of Pediatric Oncology(SIOP), and 3. United Kingdom Children’s Cancer Study Group (UKCCSG) .
- 45. COG AREN0321 protocol for high risk Wilms tumor • Focal anaplastic stage I-III Wilms tumors and diffuse anaplastic stage I Wilms tumors - Nephrectomy followed by vincristine, actinomycin-D, and doxorubicin in addition to local radiotherapy • Focal anaplastic stage IV Wilms tumors and diffuse anaplastic stage II-III tumors –Patients undergo the same treatment, with the addition of cyclophosphamide, etoposide, and carboplatin • Stage IV diffuse anaplastic Wilms tumors - More aggressive treatment is delivered; nephrectomy is followed by initial irinotecan and vincristine administration, which in turn is followed by actinomycin-D, doxorubicin, cyclophosphamide, carboplatin, etoposide, and radiotherapy.
- 46. SURGICAL CONSIDERATIONS: • Radical nephrectomy by transperitoneal approach. • Thorough exploration of the abdominal cavity to exclude local tumor extension, liver and nodal metastases, or peritoneal seeding. • Accurate staging to determine appropriate chemotherapy & need for radiation therapy. • Selective sampling of suspicious nodes is essential. • Formal RPLND is not recommended.
- 47. • Risk factors for local tumor recurrence (Shamberger): 1.tumor spillage, 2.unfavorable histology, 3.incomplete tumor removal, and 4.absence of any lymph node sampling.
- 48. PREOPERATIVE CHEMOTHERAPY: • Situations where preoperative chemotherapy is recommended:- 1. Children for whom renal-sparing surgery is planned, 2. Tumors are inoperable at surgical exploration, and 3. There is tumor extension into IVC above hepatic veins. • An inoperable tumor should be considered stage III and treated accordingly.
- 49. • Inoperability should not be based on preoperative imaging studies, which can overestimate local tumor extension. • Pretreatment with chemotherapy almost always reduces the bulk of tumor and renders it resectable. • Majority of reduction in tumor volume occurs in first 4 weeks of chemotherapy.
- 50. A, MRI of a Wilms tumor that was pretreated with chemotherapy. B, After 6 weeks of chemotherapy, the tumor is much smaller in size
- 51. MANAGEMENT OF LUNG METASTASIS: • CXR negative but CT positive: tissue diagnosis of lung nodules because several conditions (eg, histoplasmosis, atelectasis, pseudotumor, intrapulmonary lymph node, pneumonia) can mimic pulmonary metastases.
- 52. • WT FH with lung mets, no other mets/1p or 16q deletion: 6 weeks of actinomycin-D, doxorubicin, and vincristine. Complete resolution- No radiation required. No resolution- cyclophosphamide and etoposide in addition + radiation therapy.
- 53. MANAGEMENT OF B/L WILMS TUMORS: • No initial radical nephrectomy. • Preoperative chemotherapy for 6 weeks. • tumors amenable to renal-sparing procedures can proceed with surgery. • Tumors not responding- B/L open biopsy & additional chemo based on biopsy findings.
- 54. • Proceed to Sx at 12 weeks of therapy (no benefit beyond 12 weeks). • Partial nephrectomy, tumor enucleation or wedge excision of tumor. • In FH tumors, even with positive margins or large B/L residual masses, adjuvant therapy provides a good outcome.
- 55. LATE EFFECTS OF Rx RADIATION: • Musculoskeletal problems like scoliosis. • Reduction in stature. • Hypogonadism & temporary azoospermia. • Delayed sexual maturation. • Ovarian failure. • Adverse pregnancy outcomes with increased risk for miscarriage, LBW, prematurity & congenital malformations. • Increased risk of 2nd malignant neoplasms.
- 56. CHEMO: • Congestive heart failure caused by anthracyclines(DOX)
- 57. FOLLOW-UP
- 58. THANK YOU