
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Clotting and bleeding copy
Semelhante a Clotting and bleeding copy (20)
Último
Último (20)
Clotting and bleeding copy
- 1. BLEEDING AND THROMBOSIS ! Vessel wall , blood platelets and plasma proteins ! Normal hemostatic system = balance between thrombosis and bleeding ! Tendency for thrombosis : 1. immobilized after surgery 2. chronic heart failure 3. atherosclerotic vascular disease 4. malignancy 5. pregnancy ! Patient’s history : mode of onset, sites of bleeding, family bleeding tendency, drug ingestion ! Physical examination : bleeding in the skin or joint deformities ( due to previous hemarthroses ) ! General screening test " more specific test ( immunologic, functional or genetic tests ) ! Hypercoagulable or prothrombotic pt : a. repeated episodes of thromboembolism without an obvious predisposing condition b. family history of thrombosis c. thromboembolism in the adolescent and young adults NORMAL HEMOSTASIS ! trauma, disease or surgery " disrupts the vascular subendothelium connective tissue ! Primary hemostasis : platelet plug formation ; within seconds , capillaries, small arterioles and venules ! Secondary hemostasis # plasma coagulation system # result in fibrin formation # several minutes ; strengthens the primary hemostatic plug # larger vessels # lasts for hours or days ! Primary and secondary hemostasis are closely linked ! Activated platelets accelerate plasma coagulation reaction and thrombin induce platelet activation
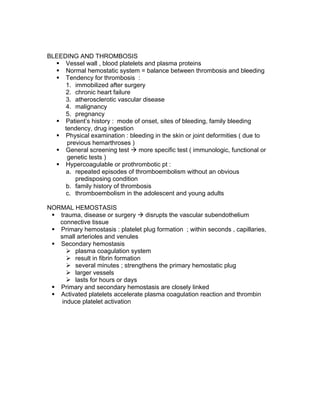
- 2. Figure 53-2 PRIMARY HEMOSTASIS ! A) Platelet activation and adhesion, B) aggregation, and C) granule release ! Platelets adhere to collagen fibrils in vascular subendothelium via (Gp) /Ia/IIa and GpVI ( see figure 53-2 ) ! GpVI binding " binds collagen " activates platelet via the Fc receptor gamma ( FcRγ) . ! Von Willebrand factor ( vWF) – an adhesive glycoprotein allow the platelets to remained attached to the vessel wall by forming a link between the platelet receptor Gp Ib/IX and collagen fibrils ! Activated platelets " release preformed granules with mediators ( Fig 53-1) ( Fig 53-1) ! Platelet activation and secretion regulated by : changes in cyclic nucleotides, influx of calcium, hydrolysis of membrane phospholipids and phosphorylation of critical intracellular proteins Prothombotic mechanism : ! Binding of agonists ( epinephrine, collagen or thrombin ) to the platelet surface receptors " activates membrane enzymes ( phospholipase C and phospholipase A2 ) " (+) release Arachidonic Acid (AA) from the membrane phospholipids (phospatidylinositol and phospahatidylcholine) ! AA" Thromboxane A2 via the cyclooxygenase " ( +) phospholipase C
- 3. ! Generation of thromboxane A2 in platelets and prostacyclin ( PGI2) in endothelial cells ! Four receptors for platelet adhesion: o Gp Ib/IX " binds to vWF o Gp IIb/IIIb " binds to fibrinogen o Gp Ia/ IIa and Gp VI " binds to collagen Platelet Granule release ( See Fig 53- 1 ) : ! Platelets secrete their granules in the plasma ! Endoglycosidase and Heparin cleaving enzymes ! vWF, fibronectin, thrombospondin, platelet derived growth factor ( PDGF) and heparin neutralizing factor ( platelet factor 4) : released form α granules ! released ADP binds to purigenic receptors and changes the conformation of Gp IIb/IIIa " binds to fibrinogen " linking other platelets" hemostatic plug ! P2Y12 – principal activating receptor on the platelet ! PDGF " (+) growth and migration of fibroblast and smooth muscle cells within the vessel wall ( repair process ) Antithrombotic mechanism : ! Prostacylin - from the endothelium , inhibits platelet activation via increase in the intraplatelet cAMP ! Endothelium " ecto-ADPase " hydrolyse the agonist platelet ADP
- 4. COAGULATION REACTIONS / CASCADE Intrinsic ( vascular ) pathway : factors 12 (Hageman )! 11! 9 + 8 ! 10 Extrinsic (tissue ) pathway : factors 7! 10 Common pathway : factors 10 !5 ! 2 ! 1 ( thrombin ) ! 13 !fibrin NOTE :” Factors “ should be in “ Roman numerals “ but the above numbers were made just for memory work only Classic Four Reactions : Figure 53-7 REACTION 1 ( INTRINSIC OR CONTACT PHASE ) ! 3 plasma CHONs forms a complex : Hageman factor (factor XII), high molecular kininogen (HMWK) and prekalikrein (PK) " bind to subendothelial collagen " Factor XII " XIIa" activates XIa REACTION 2 ( EXTRINSIC ) ! Complex : Factor VII + Ca + Tissue factor " major way to initiate coagulation ! Require calcium and Vitamin K : Factors II (prothrombin),IX, X (formed by the liver ) " inhibited by Vitamin K antagonist ( warfarin ) REACTION 3 ( COMMON ) ! Merging and interaction of the intrinsic and the extrinsic pathway ! Factor VIIa" X and IX ! Factor XIa" IX ! Factor X + VIIIa + IX REACTON 4 ( FINAL STEP) ! Prothrombin (PT) ( with Factor Va + Ca )" thrombin ! Thrombin : fibrinogen " fibrin ( major role) , (+) platelet aggregation and secretion , factors V, VII and XIII CLOT LYSIS / FIBRINOLYTIC PROCESS AND REPAIR ! Activators : Hageman factor fragments , urinary plasminogen activator ( uPA), or urokinase and tissue plasminogen activator ( tPA)
- 5. ! tPA and uPA ( endothelial cells) " binds with plasminogen " complex " plasmin" lyses the clot/ fibrin polymer into small fragments and also cause localized degradation of fibrin " cleared by the monocyte / macrophage system ! Plasmin " binds to α2 plasmin inhibitor ( lack of this will cause excessive bleeding due to unchecked fibrinolysis ) ! (PAI) 1 – from the endothelium blocks the activation of tPA ;prothrombotic HEMOSTATIC PLUG – does not propagate beyond the site of injury REGULATORY FACTORS ! reduce the enzymes and cofactors and reduce reaction rates : antithrombin , protein C and S , Tissue factor platelet inhibitor (TFPI ) ! ANTITHROMBIN – forms complexes with coagulation factors Except Factor VII ; Heparin accelerates heparin activity ! Protein C – converted to thrombomodulin ; inactivates factors V and VIII and slows coagulation reactions; (+) release of tPA from endothelial cells ! Protein S – enhances protein C ! Reduced Protein C ,S and antithrombin" hypercoagulabe state ! Factor V (Leiden ) " resistant to protein C inhibition" 20-50% of unexplained thromboembolism ! Red thrombi : veins ; slow blood flow, rich in fibrins and RBC; leg veins " embolize to the pulmonary circulation ! White thrombi : arteries ; high blood flow ; rich in platelets ; little fibrin ; emboli " occlusion of arteries like TIA and Stroke ( cerebral arteries ),
- 6. Amaurosis fugax ( retinal arteries ) , myocardial infarction ( coronary arteries ) HISTORY : ! History of bleeding ( minor surgery, dental extraction , childbirth), family history , multiple sites bleeding; warrants blood transfusion PHYSICAL EXAMINATION ! Skin and mucous membranes ( most common ) ! Purpura- collection of blood under the skin ! Petechiae – platelet disorder ( thrombocytopenia ) ; dermis, capillaries, pinpoint lesions ! Echymoses – subcutaneous, small arterioles and venules; common bruises ! Hematomas – deeper and palpable, platelet disorders and minor trauma ! Telangiectasia – dilated capillaries ! Senile purpura – loss of connective tissue support for the capillaries and small veins; subcutaneous ! Menorrhagia – women; thrombocytopenia and thrombocytopathia ! Von Willebrand disease - GI Hge +/- angiodyplasia ! Bleeding into body cavities, retroperitoneum or joints : plasma coagulation defects ! Joint deformities due to synovial thickening, erosions of the articular cartilage, chronic inflammation and fluid collections : Deficiencies of Factors VIII and IX (sex-linked , hemophilias) ! Femoral nerve compression – retroperitoneal hematomas causing compression ! Pseudotumor syndrome – mimic malignant tumors ; soft tissue accumulations ! Intracerebral Hge – most common cause of death of severe coagulation disorders
- 7. ! HIV infection – due to infection form frequent blood transfusions and blood products transfusions ; HIV also induces decreased platelet count and bleeding LAB TEST : ! Screening tests : a. Bleeding time ( BT ) – measures platelet function b. Platelet count- correlates with tendency to bleed ; normal = 150,000 to 450,000/ µl of blood ! 50,000 - 100,000 "mild prolonged BT ; < 50,000 " easy bruising, purpura, mucosal bleeding, < 20,000 " spontaneous bleeding, internal or intracranial bleed ! Partial thromboplastin time ( PTT ) – checks the plasma coagulation function ;screens the intrinsic pathway; used in heparin infusion monitoring ! Prothrombin time – assess Factors II, IX, X ; screens the extrinsic or tissue factor- dependent pathway ; used in warfarin monitoring ! Thrombin time (TT) or clotting fibrinogen level " if PT and PTT are prolonged ! Specific coagulation factors assay
- 8. Table 53- 5 THROMBOTIC DISORDERS INHERITED Defective inhibition of coagulation factors Factor V Leiden ( resistant to inhibition to protein C ) Antithrombin deficiency Protein C deficiency Protein S deficiency Prothrombin gene mutation Impaired clot lysis Dysfibrinogenemia Plasminogen deficiency tPA deficiency PAI-1 excess Uncertain mechanism Homocystinuria- ? endothelial damage ACQUIRED Diseases or syndromes Lupus anticoagulant/ anticardiolipin antibody syndrome Malignancy Myeloproliferative disorders Thrombotic thrombocytopenia Estrogen treatment Hyperlipidemia DM Hyperviscosity syndrome (e.g. polycythemia vera , Eisenmengerization in congenital heart diseases ) Nephrotic syndrome Congestive heart failure Paroxysmal nocturnal hemoglobinuria Physiologic states Pregnancy ( especially postpartum ) Obesity Postoperative state Immobilization Old age DISORDERS OF PLATELET AND VESSEL WALL • usually bleed into superficial sites such as the skin, mucous membranes, or genitourinary or gastrointestinal tract • responds to simple measures, such as pressure and packing, or requires systemic therapy with glucocorticoids, desmopressin, plasma fractions, or platelet concentrates. • Most common vessel wall disorders : (1) various forms of thrombocytopenia, (2) von Willebrand’s disease (vWD), and
- 9. (3) drug-induced platelet dysfunction PLATELET DISORDERS • from the fragmentation of megakaryocytes, which are very large, polyploid bone marrow cells produced by the process of endomitosis • From marrow space, about one-third of the platelets are sequestered in the spleen, while the other two-thirds circulate for 7 to 10 days • Small fraction used in hemostasis" usually grow old in the circulation " removed by the phagocytes • normal blood platelet count : 150,000 to 450,000/_L. • decrease in platelet count stimulates an increase in the number, size, and ploidy of megakaryocytes, releasing additional platelets into the circulation • reduction in platelet count increases the level of free TPO and thereby stimulates megakaryocyte and platelet production. • platelet count varies during the menstrual cycle, rising following ovulation and falling at the onset of menses • decreased in severe iron, folic acid, or vitamin B12 deficiency • are acute phase reactants ; • systemic inflammation, tumors, bleeding, and mild iron deficiency may have an increased platelet count, a benign condition called secondary, or reactive, thrombocytosis • cytokines interleukin (IL) 3, IL-6, and IL-11 may stimulate platelet production in acute inflammation • myeloproliferative disorders such as polycythemia vera, chronic myeloid leukemia, myeloid metaplasia, and essential thrombocytosis can be much higher and cause either severe bleeding or thrombosis Thrombocytopenia • caused by one of three mechanisms—decreased bone marrow production, increased splenic sequestration, or accelerated destruction of platelets. • examination of the peripheral blood film, an assessment of marrow morphology by examination of an aspirate or biopsy, and an estimate of splenic size by bedside palpation supplemented, if necessary, by ultrasonography or computed tomography (CT) • “Pseudothrombocytopenia,” a benign condition in which platelets agglutinate or adhere to leukocytes when blood is collected with EDTA as anticoagulant.
- 10. IMPAIRED PRODUCTION • injure stem cells or prevent their proliferation • varying degrees of anemia and leucopenia • most common causes of decreased platelet production are marrow aplasia, fibrosis, or infiltration with malignant cells, all of which produce highly characteristic marrow abnormalities • Cytotoxic drugs impair megakaryocyte proliferation and maturation • congenital amegakaryocytic hypoplasia and thrombocytopenia with absent radii (TAR syndrome), produce a selective decrease in megakaryocyte production SPLENIC SEQUESTRATION • one-third of the platelet mass is normally sequestered in the spleen, splenectomy will increase the platelet count by 30%. • Postsplenectomy thrombocytosis is a benign self-limited condition that does not require specific therapy • spleen enlarges, the fraction of sequestered platelets increases, lowering the platelet count. • most common causes of splenomegaly are portal hypertension secondary to liver disease and splenic infiltration with tumor cells in myeloproliferative or lymphoproliferative disorders
- 11. • leukemia, lymphoma, or a myeloproliferative syndrome have both marrow infiltration and splenomegaly and develop thrombocytopenia from a combination of impaired marrow production and splenic sequestration of platelets ACCELERATED DESTRUCTION • Abnormal vessels, fibrin thrombi, and intravascular prostheses can all shorten platelet survival and cause nonimmunologic thrombocytopenia. • vasculitis, the hemolytic uremic syndrome (HUS), thrombotic thrombocytopenic purpura (TTP), or as a manifestation of disseminated intravascular coagulation (DIC). • platelets coated with antibody, immune complexes, or complement are rapidly cleared by mononuclear phagocytes in the spleen or other tissues, inducing immunologic thrombocytopenia. • viral or bacterial infections, drugs (often heparin), and a chronic autoimmune disorder referred to as idiopathic thrombocytopenic purpura (ITP) • Immunologic thrombocytopenia : do not usually have splenomegaly and have an increased number of bone marrow megakaryocytes. DRUG INDUCED THROMBOCYTOPENIA • Cancer chemotherapeutic agents may depress megakaryocyte production • large quantities of alcohol has a marrow-depressing effect • Thiazide diuretics impair megakaryocyte production and can produce mild thrombocytopenia (50,000 to100,000/_L), which may persist for several months after the drug is discontinued • complement activation following the formation of drug antibody complexes prompt rise in the platelet count when the suspected drug is discontinued • most patients recover within 7 to 10 days and do not require therapy, occasional patients with platelet counts _10,000 to 20,000/_L have severe hemorrhage and may require temporary support with glucocorticoids, plasmapheresis, or platelet transfusions • avoid the offending drug in the future • cleared from body storage depots quite slowly, such as phenytoin, may induce prolonged thrombocytopenia
- 12. HEPARIN • Between 10and 15% of patients receiving therapeutic doses " (heparin- induced thrombocytopenia, HIT) "severe bleeding or intravascular platelet aggregation and paradoxical thrombosis • “white clot syndrome,” : can be fatal • directly agglutinating platelets (type I HIT). The more serious form (type II HIT) results from an immune reaction " complex formed between heparin and the platelet-derived heparin-neutralizing protein, platelet factor 4. • heparin–PF-4 antibody complexes " bind to platelet Fc receptor and induce platelet activation and secretion. • May use low molecular weight heparin LMWH " to avoid HIT however 80to 90% of the antibodies generated against conventional heparins cross-react with low-molecular-weight heparins • Argatroban is the current drug of choice IDIOPATHIC THROMBOCYTOPENIC PURPURA • following recovery from a viral exanthem or upper respiratory illness (acute ITP) is common in children ( rare in adults ) and accounts for 90% of the pediatric cases of immunologic thrombocytopenia • 60% recover in 4 to 6 weeks and _90% recover within 3 to 6 months. • infectious mononucleosis, acute toxoplasmosis, or cytomegalovirus infection • caused by immune complexes containing viral antigens that bind to platelet Fc receptors or by antibodies produced against viral antigens that cross-react with the platelet.
- 13. • differential diagnosis ( needs bone marrow exam ) includes atypical presentations of aplastic anemia, acute leukemia or metastatic tumor. • Chronic ITP. : indolent ; years : Women age 20 to 40 ; 3:1 M/F ratio • abrupt fall in platelet count and bleeding ; history of easy bruising or menometrorrhagia. • autoimmune disorder with antibodies directed against target antigens on the glycoprotein (Gp) IIb/IIIa or, less frequently, the Gp Ib/IX complex • may be the initial manifestation of systemic lupus erythematosus (SLE) or the first sign of a primary hematologic disorder • should have a bone marrow examination and an antinuclear antibody determination • hepatic or splenic enlargement, lymphadenopathy, or atypical lymphocytes should have serologic studies for hepatitis viruses, cytomegalovirus, Epstein-Barr virus, Toxoplasma, and HIV. TREATMENT : • adults have a higher incidence of intracranial bleeding than children, specific therapy may not be necessary unless the platelet count is < 20,000/µL or there is extensive bleeding " intracranial bleeding • glucocorticoids • may require temporary phagocytic blockade with intravenous immunoglobulin (IVIg) or anti-RhD (WinRho) • Emergency splenectomy : desperately ill and have not responded to any medical measures • IVIg and anti-RhD are only transiently effective and expensive. IVIg can cause meningismus and headache, and some lots have carried hepatitis C virus. • Anti-RhD can cause hemolysis. These drugs should be used to raise the platelet count temporarily and to support patients before surgery or labor and delivery; they are not substitutes for splenectomy. • Rituximab, an anti-CD20 monoclonal antibody used to treat lymphoma, has also proven an effective approach to ITP and is probably preferable to long-term glucocorticoid therapy. ; eliminates normal B cells, including those producing the antiplatelet antibody. This B cell depletion is transient (lasting 12 to 18 months, normally) and has surprisingly few side effects or toxicities FUNCTIONAL PLATELET DISORDERS • three critical platelet reactions—adhesion, aggregation, and granule release
- 14. von Willebrand’s Disease • most common inherited bleeding disorder, occurring in 1 in 100 to 500 individuals • heterogeneous multimeric plasma glycoprotein with two major functions: (1) It facilitates platelet adhesion under conditions of high shear stress by linking platelet membrane receptors to vascular subendothelium; and (2) it serves as the plasma carrier for factor VIII, the antihemophilic factor, a critical blood coagulation protein. • normal plasma vWF level is 10 mg/L. • single large vWF precursor subunit is synthesized in endothelial cells and megakaryocytes, where it is cleaved and assembled into the disulfide- linked multimers present in plasma, platelets, and vascular subendothelium • autosomal dominant traits, and affected patients are heterozygous with one normal and one abnormal vWF allele Lab : • prolonged bleeding time , a reduction in plasma vWF concentration,, a parallel reduction in biologic activity as measured with the ristocetin, cofactor assay, and reduced factor VIII activity • mild defects may have laboratory values that fluctuate over time and may occasionally be within the normal range Three major types of vWD. A. type I disease, the most common abnormality, have a mild to moderate decrease in plasma vWF. In the milder cases, although hemostasis is impaired, the vWF level is just below normal (50% activity, or 5 mg/L). In type I disease, vWF antigen, factor VIII activity, and ristocetin cofactor activity are decreased with a normal spectrum of multimers detected by sodium dodecyl sulfate (SDS)–agarose gel electrophoresis. B. Type II disease) : less common and characterized by normal or near- normal levels of a dysfunctional protein C. Type III disease). Type III very severe form of vWD phenotypically recessive patients are usually the offspring of two parents (usually
- 15. asymptomatic) with mild type I disease. Treatment 1. oral contraceptive agents that suppress menses. 2. Desmopressin- a vasopressin analogue that has minimal blood pressure– elevating and fluid-retaining properties and raises the plasma vWF level in both normal individuals and patients with mild vWD ; esp. Type 1 ; may develop tachypylaxis; may worsen Type IIa ; ineffective on Type III ACQUIRED vWF • antibodies that inhibit vWF function or by lymphoid or other tumors that selectively adsorb vWF multimers onto their surfaces. • Anti-vWF antibodies following multiple transfusions, as well as in patients with autoimmune and lymphoproliferative disorders Platelet Membrane Defects • two major platelet surface glycoproteins. vWF facilitates platelet adhesion by binding to Gp Ib/IX,while fibrinogen links platelets into aggregates via sites on the Gp IIb/ IIIa complex. • Bernard-Soulier syndrome have markedly reduced platelet adhesion and cannot bind vWF to their platelets due to deficiency or dysfunction of the Gp Ib/ IX complex. reduced levels of another membrane protein (GpV that associates with Gp Ib/II), mild thrombocytopenia, and extremely large, lymphocytoid platelets; autosomal recessive traits ; platelets react normally to all stimuli except ristocetin. • Glanzmann’s disease, or thrombasthenia, are deficient or defective in the Gp IIb/IIIa complex. Their platelets do not bind fibrinogen and cannot form aggregates, although the platelets undergo shape change and secretion and are of normal size; autosomal recessive traits • markedly impair hemostasis, leading to recurrent episodes of severe mucosal hemorrhage • In contrast , thrombasthenic platelets adhere normally and will agglutinate with ristocetin but will not aggregate with any of the agonists that require fibrinogen binding, such as adenosine diphosphate (ADP), thrombin, or epinephrine • Treatment : transfusion with normal platelets" Alloimmunization (developed inhibitor antibodies ) Platelet Release Defects • most common mild bleeding disorders arise from the ingestion of aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) that inhibit platelet production of thromboxane A2, (mediator of platelet secretion and aggregation) " inhibit cyclooxygenase (COX) which converts arachidonic acid to a labile endoperoxide intermediate that is critical for thromboxane formation • Aspirin - irreversibly acetylates the platelet enzyme so that a single dose
- 16. impairs hemostasis for 5 to 7 days. " partially inhibits platelet release and aggregation with weak agonists, such as ADP and epinephrine, and produces a mild hemostatic defect. • COX-1, which is constitutively expressed and active in the normal platelet, and COX-2, which is induced, especially in inflamed tissue. • COX 2 – arthritis and pain ; long-acting reversible inhibitors that have no adverse effects on platelet function ; chronic use may be associated with high blood pressure and risk of thrombosis • Penicillin ( high doses ), can coat the platelet surface, block platelet release, and impair hemostasis. • release defects generally have minimal symptoms such as easy bruising, and bleeding is usually confined to the skin " prolonged oozing after surgery ( especially mucosal ) • Platelet responses to collagen and thrombin are impaired at low doses but normal at higher doses • Uremic platelet dysfunction : clinically the most important. Mechanism : not well understood; retention of phenolic and guanidinosuccinic acids, excess prostacyclin production, or impaired vWF-platelet interactions ; degree of uremia correlates with bleeding symptoms and anemia " usually be reversed by dialysis and often improves after red cell transfusion or treatment with erythropoietin ; factor VIII concentrate or desmopressin, both of which raise plasma vWF levels, can also improve hemostasis ; Conjugated estrogens improve hemostasis and can be used as long-term therapy Storage Pool Defects • Platelet granules have considerable amounts of adenine nucleotides, calcium, and adhesive glycoproteins such as thrombospondin, fibronectin, and vWF, all of which promote platelet adhesion and aggregation. • may be inherited as an isolated disorder or be part of systemic granule packaging defects such as oculocutaneous albinism or the Hermansky- Pudlak or Che´diak-Higashi syndromes • cannot be distinguished from those with other functional platelet disorders, since they all have easy bruising, mucosal bleeding, and a prolonged bleeding time • will usually aggregate in response to arachidonic acid in contrast to COX defects • decreased levels of specific granule constituents such as ADP and serotonin and abnormalities in granule morphology that are best visualized by electron microscopy • acute or chronic leukemia or one of the myeloproliferative disorders develop an acquired storage pool disorder due to dysplastic megakaryocyte development • liver disease and some patients with SLE or other immune complex– mediated disorders may have circulating platelets that have degranulated
- 17. prematurely ; after prolonged cardiopulmonary bypass • only mildly impaired hemostasis. " treated with platelet transfusion and occasionally desmopressin VESSEL WALL DISORDERS • or nonthrombocytopenic purpura • usually mild and confined to the skin and mucous membranes. • bleeding time and tests of platelet function, are usually normal • damage to capillary endothelium, abnormalities in the vascular subendothelial matrix or extravascular connective tissues that support blood vessels, or from the formation of abnormal blood vessels THROMBOTIC THROMBOCYTOPENIC PURPURA • fulminant, often lethal disorder that may be initiated by endothelial injury and subsequent release of vWF and other procoagulant materials from the endothelial cell. • pregnancy, metastatic cancer, mitomycin C, high dose chemotherapy, HIV infection, and certain drugs, such as the antiplatelet agent ticlopidine • microvascular deposition of hyaline fibrin thrombi, thrombocytopenia, microangiopathic hemolytic anemia, fever, renal failure, fluctuating levels of consciousness, and evanescent focal neurologic deficits • hyaline thrombi in arterioles, capillaries, and venules without any inflammatory changes in the vessel wall is diagnostic • severe Coombs-negative hemolytic anemia with schistocytes or fragmented red blood cells in the peripheral blood smear, coupled with thrombocytopenia, and minimal activation of the coagulation system • Differential diagnosis : vasculitis and SLE " Platelet-associated IgG and complement levels are usually normal in TTP
- 18. • Hemolytic anemia with fragmentation of erythrocytes and signs of intravascular hemolysis, thrombocytopenia, diffuse and nonfocal neurologic findings, decreased renal function, and fever • neurologic and renal symptoms are usually seen only when the platelet count is markedly diminished (< 20 to 30 X 103 /µL). • Neurologic symptoms develop in > 90% of patients whose disease terminates in death • If the coagulation tests indicate major consumption of clotting factors, the diagnosis of TTP is doubtful. A positive antinuclear antibody (ANA) determination is obtained in < 20% of patients • due to a deficiency in the activity of a specific metalloproteinase called ADAMTS 13, a normal plasma constituent that cleaves the ultra-high- molecular-weight (UHMW) forms of vWF secreted by endothelial cells to yield the heterogeneous set of multimers normally present in plasma • recurrent episodes of a TTP-like illness (Upshaw-Schulman syndrome) and are deficient in ADAMTS 13; the syndrome is inherited as an autosomal recessive trait ; asymptomatic carriers with 50% levels of ADAMTS 13 are at increased risk of thromboembolism • Treatment : exchange transfusion or intensive plasmapheresis coupled with infusion of fresh-frozen plasma. " remove abnormal forms of vWF, lower the concentration of ADAMTS 13 inhibitor, and replenish the deficient enzyme. • relapsing form of TTP require maintenance plasmapheresis and plasma infusion, and a few patients are controlled only with glucocorticoids
- 19. • other tx : enzyme replacement and immunosuppression to block inhibitor production. HEMOLYTIC-UREMIC SYNDROME ( HUS ) • disease of infancy and early childhood that closely resembles TTP. • fever, thrombocytopenia, microangiopathic hemolytic anemia, hypertension, and varying degrees of acute renal failure. • In many cases, onset is preceded by a minor febrile or viral illness, and an infectious or immune complex–mediated cause has been proposed. • Epidemics related to infection with a specific strain of Escherichia coli (O157:H7) have been documented. • The bacteria contain a Shigella-like toxin that damages endothelial cells. • As in TTP, DIC is not found. In contrast to TTP, the disorder remains localized to the kidney, where hyaline thrombi are seen in the afferent arterioles and glomerular capillaries. Thrombi are not present in other vessels, and neurologic symptoms, other than those associated with uremia, are uncommon. • No therapy is proven effective; however, with dialysis for acute renal failure, the initial mortality is only 5% in children but may be higher in adults. • Between 10 and 50% of patients have some chronic renal impairment. • ADAMTS 13 levels are normal, and no inhibitors of the enzyme are present in this disorder HENOCH-SCHONLEIN PURPURA • or anaphylactoid, purpura is a distinct, self-limited type of vasculitis that occurs in children and young adults. • acute inflammatory reaction in capillaries, mesangial tissues, and small arterioles that leads to increased vascular permeability, exudation, and hemorrhage. • Vessel lesions contain IgA and complement components. • May be preceded by an upper respiratory infection or streptococcal pharyngitis or be associated with food or drug allergies. • a purpuric or urticarial rash on the extensor surfaces of the arms and legs and on the buttocks as well as polyarthralgias or arthritis, colicky abdominal pain, and hematuria from focal glomerulonephritis. • Despite the hemorrhagic features, all coagulation tests are normal. • may develop fatal acute renal failure, and 5 to 10% develop chronic nephritis. • Glucocorticoids provide symptomatic relief of the joint and abdominal pains but do not alter the course of the illness. METABOLIC AND INFLAMMATORY DISORDERS
- 20. • Acute febrile illnesses may cause capillary fragility and skin bleeding • Immune complexes containing viral antigens or the viruses themselves may damage endothelial cells • rickettsiae that cause Rocky Mountain spotted fever or other infections • Thrombocytopenia is also a frequent finding in acute infections • whenever the platelet count is < 10,000/µL, gaps develop between endothelial cells, which allow the diapedesis of red cells into the dermis, forming petechiae. • sulfonamides, penicillin, and allopurinol may cause vascular inflammation, resulting in maculopapular or urticarial rashes " additive, and drug reactions in thrombocytopenic individuals cause an intensely hemorrhagic rash. • Hyperglobulinemic purpura - Occasionally, patients with diffuse polyclonal hyperglobulinemia will develop purpuric lesions on the lower limbs ; a benign condition • Vascular purpura may occur in patients with various monoclonal gammopathies, including Waldenstrom’s macroglobulinemia, multiple myeloma, and cryoglobulinemia " markedly increase serum viscosity and may impair blood flow through capillaries and lead to retinal hemorrhage, central nervous system dysfunction, and skin necrosis ; globulins may impair platelet aggregation and adhesion and interfere with fibrin polymerization • mixed cryoglobulinemia develop a more extensive maculopapular lesion due to immune complex- mediated damage to the vessel wall ; may be associated with arthralgias, diffuse weakness, and unexplained nephritis. • Plasmapheresis will temporarily lower the level of globulins, remove immune complexes, and improve symptoms in these patients • Scurvy (vitamin C deficiency) develop painful episodes of perifollicular skin bleeding as well as bleeding into muscles and, occasionally, into the gastrointestinal and genitourinary tracts. ; hyperkeratosis of skin, gum swelling, and low levels of the vitamin in leukocytes ; Vitamin C is needed to synthesize hydroxyproline, an essential constituent of collagen $ collagen synthesis is impaired • Cushing’s syndrome : excess production of glucocorticoids, or patients on large doses of glucocorticoids develop generalized protein wasting and may show skin bleeding or easy bruising due to atrophy of the supporting connective tissue around blood vessels. • Senile purpura—dark purple, irregularly shaped hemorrhagic areas due to abnormal skin mobility that tears small blood vessels. ; atrophy of perivascular connective tissue on the extensor surfaces of the hands and arms • inherited disorders of the connective tissue matrix such as Marfan’s syndrome, Ehlers-Danlos syndrome, and pseudoxanthoma elasticum also have easy bruising. • Ehlers-Danlos syndrome may develop aneurysms in intraabdominal vessels and apoplectic rupture and hemorrhage due to defects in the
- 21. vascular collagen network. • Osler-Rendu-Weber disease [hereditary hemorrhagic telangiectasia (HHT)], an inherited autosomal dominant disorder, have frequent episodes of nasal and gastrointestinal bleeding from abnormal telangiectatic capillaries; may develop pulmonary arteriovenous fistulas • 2 Genetic defects : involving proteins that bind to transforming growth factor β (TGF- β); HHT-1 has mutations in endoglin, and HHT-2 has mutations in ALK-1. • Angiodysplasia of the colon have increased incidence of gastrointestinal bleeding. • Kasabach-Merritt syndrome, patients may have very extensive and progressively enlarging vascular malformation that may involve large portions of their extremities " Bleeding is secondary to DIC triggered by stagnant blood flow through the tortuous vessels.
- 22. PART TWO : DISORDERS OF COAGULATION AND THROMBOSIS • Characteristically bleed into muscles, joints, and body cavities hours or days after an injury • Inherited plasma coagulation disorders are due to defects in single coagulation proteins, with the two X-linked disorders, factors VIII and IX deficiency, accounting for the majority. • interval range for most coagulation factors is 50 to 150% of this average value, and the minimal level of most individual factors needed for adequate hemostasis is 25% • Acquired coagulation disorders are both more frequent and more complex, arising from deficiencies of multiple coagulation proteins and simultaneously affecting both primary and secondary hemostasis. • most common acquired hemorrhagic disorders are (1) disseminated intravascular coagulation (DIC), (2) the hemorrhagic diathesis of liver disease, and (3) vitamin K deficiency and complications of anticoagulant therapy • Risk factors such as atherosclerotic vascular disease, congestive heart failure, malignancy, and immobility predispose patients to thrombosis FACTOR VIII DEFICIENCY—HEMOPHILIA A Pathogenesis and Clinical Manifestations • Antihemophilic factor (AHF), or factor VIII coagulant protein - large (265- kDa), single-chain protein that regulates the activation of factor X by proteases generated in the intrinsic coagulation pathway ; synthesized in liver and circulates complexed to the von Willebrand factor (vWF) protein. Factor VIII molecule is present in low concentration (10 mg/L) and is susceptible to proteolysis. • One in 10,000 males is born with deficiency or dysfunction of the factor VIII molecule" hemophilia A, is characterized by bleeding into soft tissues, muscles, and weight-bearing joints • Symptomatic patients usually have factor VIII levels < 5%,! • !< 1% factor VIII activity have severe disease; they bleed frequently even without discernible trauma • < 5% have mild disease with infrequent bleeding that is usually secondary to trauma. • > 25% are discovered when they bleed after major trauma or surgery. • bleeding occurs hours or days after injury, can involve any organ, and, if untreated, may continue for days or weeks • Symptoms often precede objective evidence of bleeding. (2) Signs of bleeding may not appear until several days after well-documented trauma. • large collections of partially clotted blood putting pressure on adjacent normal tissues and can cause necrosis of muscle (compartment syndromes), venous congestion (pseudophlebitis), or ischemic damage to nerves.
- 23. • often develop femoral neuropathy due to pressure from an unsuspected retroperitoneal hematoma • large calcified masses of blood and inflammatory tissue that are mistaken for cancers (pseudotumor syndrome). • usually diagnosed shortly after birth because of an extensive cephalhematoma or profuse bleeding at circumcision. • presents with pain followed by swelling in a weight-bearing joint, such as the hip, knee, or ankle • blood in the joint (hemarthrosis) causes synovial inflammation, and repetitive bleeding erodes articular cartilage and causes osteoarthritis, articular fibrosis, joint ankylosis, and eventually muscle atrophy • Hematuria, without any genitourinary pathology, is also common " usually self-limited and may not require specific therapy • most feared complications of hemophilia are oropharyngeal and central nervous system bleeding • oropharyngeal bleeding may require emergency intubation to maintain an adequate airway • prolonged PTT with all other tests normal • Differential Diagnosis : factor VIII deficiency and factor IX deficiency " must determination of the assays Treatment : • For pain " Avoid the use of aspirin or aspirin-containing drugs, which impair platelet function and may cause severe hemorrhage. Cyclooxygenase inhibitors can be used, as they do not impair platelet function • Plasma products enriched in factor VIII reduce the degree of orthopedic deformity and permit virtually any form of elective and emergency surgery • factor VIII concentrates has also produced serious complications, including viral hepatitis, chronic liver disease, and AIDS • Cryoprecipitate, which contains about half the factor VIII activity of fresh- frozen plasma in one-tenth the original volume, is simple to prepare and is produced in hospital • Modification and Safety Measures adapted for Factor VIII : heating of lyophilized factor VIII concentrates under carefully controlled conditions can inactivate HIV without destroying factor VIII activity. Second, highly purified factor VIII can be produced by adsorbing and eluting factor VIII from monoclonal antibody columns. Third, recombinant factor VIII • One unit of factor VIII infused, defined as the amount present in 1 mL normal plasma, " raise the plasma level of the recipient by 2%/kg of body weight • Factor VIII has a half-life of 8 to 12 h, making it necessary to infuse it continuously or at least twice daily to sustain a chosen factor VIII level • Desmopressin (DDAVP), alternative option , which transiently increases the factor VIII level " increase the factor level two- to threefold but may cause hyponatremia or may precipitate thrombosis in elderly • Life-threatening bleeding into the central nervous system or major surgery
- 24. may require therapy for 2 weeks with levels kept at a minimum of 50% normal. • ε "!aminocaproic acid (EACA) four times daily for 3to 4 days after the dental procedure. EACA is a potent antifibrinolytic agent that inhibits plasminogen activators present in oral secretions and stabilizes clot formation in oral tissue • tranexamic acid, a longer-acting antifibrinolytic • Blood products " AIDS transmission ? , multiple episodes of hepatitis, and a majority have elevated hepatocellular enzyme levels and abnormalities on liver biopsy ; Between 10 and 20% of patients also have hepatosplenomegaly, and a small number develop chronic active or persistent hepatitis or cirrhosis • Other complications : Iron deficiency ( rare because it is recycled ) • Gene therapy : still investigational GENETIC COUNSELLING : • Precise diagnosis is possible early in pregnancy from either chorionic villus biopsy or amniocentesis. • Female carriers of hemophilia, who are heterozygotes, usually produce sufficient factor VIII from the factor VIII allele on their normal X chromosome for normal hemostasis • true female hemophiliacs arise from consanguinity within families with hemophilia or from concomitant Turner’s syndrome or XO mosaicism in a carrier female. FACTOR IX DEFICIENCY—HEMOPHILIA B • Factor IX is a single-chain, 55- kDa proenzyme that is converted to an active protease (IXa) by factor XIa or by the tissue factor–VIIa complex • Factor IXa then activates factor X in conjunction with activated factor VIII • Factor IX is one of six proteins synthesized in the liver that require vitamin K for biologic activity. Vitamin K is a cofactor for a unique posttranslational modification that inserts a second carboxyl group onto certain glutamic acid residues on factor IX • Vitamin K is a cofactor for a unique posttranslational modification that inserts a second carboxyl group onto certain glutamic acid residues on factor IX • Factor IX gene is on the X chromosome • Factor IX deficiency or dysfunction (hemophilia B, Christmas disease) occurs in 1 in 100,000 male births • indistinguishable clinically from factor VIII deficiency (hemophilia A) but requires different treatment • freshfrozen plasma or a plasma fraction enriched in the prothrombin complex proteins • Tx : Monoclonally purified or recombinant factor IX preparations
- 25. • Trace quantities of activated coagulation factors in prothrombin complex concentrates may activate the coagulation system and cause thrombosis and embolism " common in immobilized surgical patients and patients with liver disease • some centers have returned to fresh frozen plasma for factor IX–deficient surgical patients, while others have recommended the addition of small doses of heparin to the concentrate to activate antithrombin III during the infusion and reduce hypercoagulability. The recombinant or monoclonally purified products are less likely to be thrombogenic FACTOR XI DEFECIENCY • Factor XI is a 160-kDa dimeric protein activated to an active protease (XIa) by factor XIIa, in conjunction with highmolecular- weight kininogen and kallikrein • inherited as an autosomal recessive trait and is especially common in Ashkenazi Jews • spontaneous bleeding is less, and hemarthroses are rare. • posttraumatic bleeding or with bleeding in the perioperative period, and occasional factor XI–deficient women have menorrhagia • Daily infusions of fresh-frozen plasma are sufficient, since the half-life of factor XI is approximately 24 h. OTHER FACTOR DEFICIENCIES • Deficiencies in factors V, VII, X, and prothrombin (factor II) are exceedingly rare autosomal recessive disorders. • Spontaneous or posttraumatic musculoskeletal bleeding or menorrhagia can occur with these deficiencies, but hemarthroses are uncommon. • TX : Fresh-frozen plasma or prothrombin concentrates • Defects in the contact activation pathway involving Hageman factor (factor XII), high-molecular-weight kininogen, and prekallikrein cause laboratory abnormalities but no clinical bleeding because there is direct activation of factor IX by the tissue factor–VIIa complex AFIBRINOGENEMIA AND DYSFIBRINOGENEMIA • Fibrinogen is an abundant plasma protein (2.5 g/L). • Mutations have been identified that alter the release of fibrinopeptides from the Aα and Bβ chains of fibrinogen, the rate of polymerization of fibrin monomers, and the sites for fibrin cross-linking • almost always inherited as autosomal dominant traits • slightly prolonged PT and PTT, a prolonged thrombin time, and a disparity in levels of fibrinogen measured with functional and immunologic assays. • most patients have no symptoms or only moderate bleeding ; few have hypercoagulable state and increase the risk of thrombosis, and others have been associated with an increased incidence of abortion • patients with liver disease, hepatomas, AIDS, and lymphoproliferative
- 26. disorders develop an acquired form of dysfibrinogenemia ! FACTOR XIII DEFICIENCY AND DEFECTIVE FIBRIN CROSS-LINKING • Factor XIII is a transglutaminase that stabilizes fibrin clots by forming ε- amino– γ glutamyl cross-links between adjacent α and γ chains of fibrin • extremely rare inherited syndrome ; usually bleed in the neonatal period from their umbilical stump or circumcision • may have poor wound healing, a high incidence of infertility among males and abortion among affected females, and a high incidence of intracerebral hemorrhage. • isoniazid, may bind to cross-linking sites on fibrinogen and mimic factor XIII deficiency by blocking enzyme activity • Normal hemostasis requires only 1% of normal enzyme activity; a single infusion of fresh-frozen plasma or a purified factor XIII–rich product derived from human placenta called Fibrogammin • Factor XIII has a 14-day half-life. VITAMIN K DEFICIENCY • Vitamin K is a fat-soluble vitamin that plays a critical role in hemostasis. • mediates posttranslational modification of glutamate residues to - carboxylglutamate, a critical step for the activity of vitamin K-dependent proteins for calcium binding and proper assembly to phospholipid membranes • Dietary vitamin K is absorbed in the small intestine and stored in the liver. ; also synthesized by endogenous bacterial flora in the small intestine and colon; however, the quantity of endogenous vitamin K absorbed from the large intestine is debated. • Vitamin K " converted to an active epoxide in liver microsomes and serves as a cofactor in the enzymatic carboxylation of glutamic acid residues on prothrombin complex proteins • Three major causes of vitamin K deficiency are inadequate dietary intake, intestinal malabsorption, and loss of storage sites due to hepatocellular disease • common in association with the use of broad-spectrum antibiotics • Neonatal vitamin K deficiency, which causes hemorrhagic disease of the newborn, has disappeared from western countries with the routine administration of vitamin K to all newborn infants. • Although a 30-day supply of vitamin K is stored in the normal liver, acutely ill patients can become deficient within 7 to 10 day • biliary tract surgery who have no dietary intake of vitamin K, have T-tube drainage of bile, and are on broad-spectrum antibiotics • chronic liver disease, particularly primary biliary cirrhosis, and in some malabsorption states • cephalosporins inhibit the reduction and recycling of vitamin K, much like warfarin
- 27. • Deficiency of Vitamin K " prothrombin complex proteins (factors II, VII, IX, X; proteins C and S) decrease • shortest half-lives, factor VII and protein C, decrease first " may have a prolonged PT and a normal PTT " Later, as the levels of the other factors fall, the PTT will also become prolonged. • Parenteral administration of 10 mg vitamin K rapidly restores vitamin K levels in the liver and permits normal production of prothrombin complex proteins within 8 to 10 h fresh-frozen plasma, which immediately corrects the hemostatic defect • Coagulation Disorders Associated with Liver Failure - liver is central to hemostasis because it is the site of synthesis and clearance of most procoagulant and natural anticoagulant proteins and of essential components of the fibrinolytic system - - presence of prolonged TT, normal fibrinogen, and FDP levels suggests dysfibrinogenemia ; Dysfibrinogenemia is a relatively common finding in patients with liver disease due to impaired fibrin polymeratization - Thrombocytopenia is common in patients with liver disease and may be due to congestive splenomegaly (hypersplenism), or immune-mediated shortened platelet life span (primary biliary cirrhosis). In addition, several anatomic abnormalities secondary to underlying liver disease further promote the occurrence of hemorrhage - Normal levels of FV and low levels of FVII suggest vitamin K deficiency. - Vitamin K levels may be reduced in patients with liver failure due to compromised storage in hepatocellular disease, changes in bile acids, or cholestasis that can diminish the absorption of vitamin K. Replacement of vitamin K may be desirable (10 mg given by slow intravenous injection) to improve hemostasis.
- 28. DISSEMINATED INTRAVASCULAR COAGULATION • Explosive and life-threatening bleeding disorder or a relatively mild or subclinical disorder. • obstetric catastrophes, metastatic malignancy, massive trauma, and bacterial sepsis • Tumors and traumatized or necrotic tissue release tissue factor into the circulation • Endotoxin from gram-negative bacteria activates several steps in the coagulation cascade • direct effect on the activation of Hageman factor (factor XII), endotoxin induces the expression of tissue factor on the surface of monocytes and endothelial cells. • stimuli cause the deposition of small thrombi and emboli throughout the microvasculature • early thrombotic phase of DIC is then followed by a phase of procoagulant consumption and secondary fibrinolysis • early thrombotic phase of DIC is then followed by a phase of procoagulant
- 29. consumption and secondary fibrinolysis. Continued fibrin formation and fibrinolysis lead to hemorrhage from the coagulation factor and platelet depletion and the antihemostatic effects of fibrin degradation products • Most patients have extensive skin and mucous membrane bleeding and hemorrhage from surgical incisions or venipuncture or catheter sites. • peripheral acrocyanosis, thrombosis, and pregangrenous changes in digits, genitalia, and nose—areas where blood flow is markedly reduced by vasospasm or microthrombi • laboratory manifestations include thrombocytopenia and the presence of schistocytes or fragmented red blood cells that arise from cell trapping and damage within fibrin thrombi; prolonged PT and PTT and thrombin time and a reduced fibrinogen level from depletion of coagulation proteins; and elevated fibrin degradation products (FDP) from intense secondary fibrinolysis • D dimer immunoassay, which measures cross-linked fibrin derivatives (i.e., those that have been in blood clots), is a more specific FDP assay • Low fibrinogen levels in DIC predict more bleeding
- 31. TREATMENT OF DIC • an attempt to correct any reversible cause of DIC; (2) measures to control the major symptom, either bleeding or thrombosis; and (3) a prophylactic regimen to prevent recurrence in cases of chronic DIC. • abruptio placentae or acute bacterial sepsis, prompt delivery of the fetus and placenta or treatment with appropriate antibiotics will reverse the DIC syndrome • metastatic tumor causing DIC, control of the primary disease may not be possible " long-term prophylaxis • fresh frozen plasma to replace depleted clotting factors and platelet concentrates • acrocyanosis and incipient gangrene or other thrombotic problems " anticoagulation with intravenous heparin • use of heparin in the treatment of bleeding : still controversial ; reduce thrombin generation and prevent further consumption of clotting proteins, it should be reserved for patients with thrombosis or who continue to bleed despite vigorous treatment with plasma and platelets
- 32. • Therapy will only stabilize the patient, prevent exsanguination or massive thrombosis, and permit institution of definitive therapy •