
Recomendados
Mais conteúdo relacionado
Semelhante a patho(gross).pdf
Semelhante a patho(gross).pdf (20)
Mais de bnvj
Mais de bnvj (11)
Último
Último (20)
patho(gross).pdf
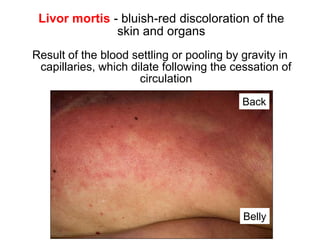
- 1. Livor mortis - bluish-red discoloration of the skin and organs Result of the blood settling or pooling by gravity in capillaries, which dilate following the cessation of circulation Back Belly it is absent where there is pressure which prevents dilation of capillaries Livor due to hyopstasis first 8-12Hrs Livor due to imbibition after 8-12Hrs (not moved)
- 2. Macerated foetus. Note the reddish discoloration of the skin. The epidermis is detached from the dermis in large laminae. Courtesy of Kaiser László, MD
- 3. Aspiration of gastric content caused obstruction of airways in the patient with deep coma (lethal condition) Trachea Main bronchi
- 4. Anemic infarct of the heart: circumscribed yellowish lesion, the margins are hyperemic
- 5. Hemorrhagic infarct of lung: wedge shaped, raised, dark-red area
- 6. 34 Hemorrhagic infarct of small bowels due to arterial occlusion and there is gas formation in lumen
- 7. Brain infarct: the necrotic area is softened and pale Internal capsule Infarcted area Caudate nucleus
- 8. Caseous necrosis • Immune-mediated distinctive form of coagulative necrosis in foci of tuberculous infection of the lung • Grossly, caseous necrosis is white and cheesy
- 9. Necrotizing pancreatitis: the pancreas is swollen and displays several yellowish foci of necrosis
- 10. Dry gangrene of the great toe
- 11. Obstruction of the CSF flow leads to pressure atrophy of the brain, with the enlargement of ventricles: hydrocephalus
- 12. Hydronephrosis: obstruction of the ureter (arrow) leads to sac- like dilation of renal pelvis and calyces, and pressure atrophy of parenchyma TUMOR
- 13. Ischemic atrophy of the kidney because the supplying renal artery was progressively narrowed
- 14. Hypertrophy of heart, triggered by action of mechanical stimuli ( workload) and vasoactive substances (e.g., angiotensin II). Free wall thickness: above 15 mm
- 15. Hypertrophy of the muscles of urinary bladder due to urethral obstruction
- 16. Steatosis: the liver is enlarged, yellow and greasy, resembles to goose liver Courtesy of E. Kemény, SZTE Pathology hypoxia-hepatotoxins obesity-diabetes alcohol-protein energy malnutrition
- 17. The hepatocytes are vacuolated; representing accumulations of neutral lipids that have been removed by lipid solvents during tissue processing Frozen section, Oil Red O
- 18. Jaundice: yellowish discoloration of skin
- 19. Dystrophic calcification of aortic valves (calcifying aortic stenosis) valsalva sinuses are rigid (Ca deposits) which cause narrowing of aorta
- 20. 7 Pulmonary edema: the lungs 2 to 3 times exceed their normal weight; sectioning reveals a foamy mixture of air, edema fluid, and RBCs Trachea Acute LHF
- 21. 9 Hydrothorax in chronic right-sided HF it should be almost colorless but blood during autopsy changed the color anthracosis
- 22. 10 Increased hydrostatic pressure in the portal venous circulation (portal hypertension) by cirrhosis of liver (shown) is an important cause of ascites
- 23. 14 Severe lymphedema of arm after mastectomy, surgical dissection of the axillary lymph nodes and irradiation of the axillary region because of breast cancer. Post-mastectomy Lymphedema
- 24. Elephantiasis. The patient suffered from morbid obesity, type 2 diabetes and congestive heart failure.
- 25. 21 Hepatic congestion: hypoxic/fatty hepatocytes around central veins are pale yellow, the better oxigenated portal parts are red.
- 26. 24 Chronic left-sided HF chronic pulmonary congestion: brown induration of lungs
- 27. Cyanotic induration of the kidney in chronic right-sided heart failure +Enlarged
- 28. Congestive splenomegaly. Weight: up to 500 gm, the organ is firm, the capsule is thickened, the malphigian corpuscles are indistinct
- 29. Peptic ulcer of the postpyloric duodenum that eroded the pancreaticoduodenal artery (arrow) and caused lethal bleeding
- 30. Classification and nomenclature of hemorrhage • Surface - External, internal • Enclosed within a tissue Suffusion (2-dimensional) Hematoma (3-dimensional); may be - insignificant (bruise) - lethal (retroperitoneal, subarachnoidal, intracerebral) Subcutaneous suffusion due to trauma
- 31. 33 Subarachnoidal hematoma rupture of cerebral a. aneurysm
- 32. Basal ganglia hemorrhage as a result of long-standing hypertension intracerebral hemmorhage (HTN crisis)
- 33. 35 Petechiae: minute, 1-2 mm hemorrhages into skin, mucous membranes or serosal surfaces, seen in thrombocytopenia, defective platelet function or clotting factor deficits
- 34. 36 Purpura: slightly larger (>3 mm) hemorrhages, may be associated with similar pathologies, as well as vasculitis Purpuras in small vessel vasculitis Sándor Husz, MD, SZTE Dermatology
- 35. 39 Hemopericardium because of myocardial rupture (lethal) blood is in the visceral layer 400 ml can be lethal
- 36. Hemocephalus: blood fills the lateral and third ventricles (the ventricular drainage was unsuccesful) Draining channel
- 37. Iatrogenic (adverse condition in a patient resulting from treatment) hematoma around the carotid artery (CA) as complication of catheterization Internal CA External CA Common CA
- 38. 9 Atherosclerosis of aorta with mural thrombi
- 39. Endocarditis. Thrombi on the leaflets
- 40. Aneurysms in the aorta filled with thrombi
- 41. Left ventricle. Apical chronic aneurysm with mural thrombus (arrow)
- 42. 17 Auricular thrombus (arrow) in a patient with atrial fibrillation
- 43. 20 Auricular thrombus: grayish-red, lines of Zahn
- 44. Direction of blood flow Venous thrombi (red or stasis thrombi) Occur in a stagnating environment, and the thrombi contain more enmeshed RBCs among sparse fibrin strands; lAppear as long, red-blue cast of the vein lumen
- 45. 26 Verrucous vegetations (arrows) on mitral valve composed of platelets and fibrin. The patient had disseminated cancer.
- 46. 34 Red thrombi in deep veins Femoral artery
- 47. Saddle embolus (arrow) impacting the bifurcation of the pulmonary Artery prevented the influx of blood into the lungs (lethal) Aorta Pulmonary vein
- 48. Thromboembolism: hemorrhagic infarcts in the terrritory of middle cerebral artery (hemorrhage due to reperfusion) Caudate nucleus Internal capsule Putamen
- 49. 55 Ruptured aneurysm of abdominal aorta leading to retroperitoneal bleading and shock (the probe indicates the rupture)
- 50. Decreased perfusion may result in the necrosis of toes
- 51. Cardinal signs of bacterial inflammation: calor (warmth), rubor (redness), tumor (swelling), dolor (pain), and loss of function Dr. Sándor Husz, SZTE Dermatology
- 52. Unilateral bacterial inflammation of rat kidney induced by ligation of ureter and i.v. injection of bacteria. The animal was sacrified on Day 2. The affected kidney displayed inflammatory exudation-induced enlargement (“tumor”)
- 53. Gross features Normally, the serous membrane is smooth and has a glistening surface. In serous inflammation, it becomes reddish and opaque. Shown: acute serous pleurisy
- 54. Lethal acute serofibrinous peritonitis: the serosa of bowels is hyperemic; the bowels adhere to each other with fibrin strands (right: normal serosa) liver
- 55. Edema of larynx induced by adverse (allergic) reaction of an antihypertensive drug administered intravenously in hypertensive crisis. Note marked swelling of laryngeal mucosa which caused upper airway obstruction and death
- 56. Laryngal edema that caused airway obstruction
- 57. Blisters in chickenpox Superinfection with St. aureus: the blisters are filled with pus (pustula) Courtesy of dr. Ildikó Kováts
- 58. Acute fibrinous pericarditis: intense hyperemia, fibrin strands
- 59. Left: fibrinous pericarditis, right: fibrinous pleurisy (parietal pleura). The thick strands of fibrin will not not be removed by fibrinolysis, and adhesions develop between serous surfaces Diaphragm Thoracic cage
- 60. Lobar pneumonia. Hepatisation: liver-like consistency because alveoli are packed with fibrin trachea
- 61. Lung: multiple abscesses as complication of pneumonia
- 62. Furuncle (boil) Dr. Sándor Husz, SZTE Dermatology
- 63. Folliculitis on the nose; carbuncle on the face Dr. Sándor Husz, SZTE Dermatology
- 64. Cellulitis: sharp, erythematous swelling of the skin Courtesy of Erika Varga, MD, Department of Dermatology, SZTE
- 65. Empyema of thorax Healing: granulation tissue secondary calcification: callus of pleura
- 66. Purulent mediastinitis (induced by descending infection of the neck) Aorta Pulm. artery Pulm.vein Pericardium Mediastinum Mediastinum
- 67. Acute purulent peritonitis: the abdominal cavity was filled with more than 2000 ml pus
- 68. Acute purulent meningitis The exudate is localized in the subarachnoid space, the meningeal vessels are engorged and stand out prominently
- 69. Acute purulent tracheobronchitis The exudate clogged the airways and caused widespread atelectasis (collapse) of the alveoli Note: tracheobronchial toilet is necessary in patients who cannot cough actively
- 70. Purulent discharge in Neisseria gonorrhoeae infection (sexually-transmitted disease, termed gonorrhoea) Dr. Sándor Husz, SZTE Dermatology
- 71. Acute hemorrhagic cystitis: the bladder mucosa is swollen, hyperemic and displays focal hemorrhages
- 72. Pseudomembranous colitis induced by C. difficile: confluent plaques of yellow fibrin and inflammatory debris adherent to a reddened mucosa
- 73. Pseudomembranous enterocolitis: in severe cases the small bowels are also affected
- 74. Amputated leg because of necrotizing fasciitis
- 75. Gas gangrene: necrotizing and gas-producing inflammation of the lower extemity involving the abdominal wall, perineum and scrotum; the gas bubbles detach the epidermis from the underlying tissues
- 76. Gas gangrene: the gas bubbles accumulated between the epidermis and the underlying tissues
- 78. Polyoma virions in the nucleus of an epithelial cell
- 80. Comment The influenza A virus subtype H1N1 infection was lethal in this young pregnant woman; she was regrettably not vaccinated Huge problem If people refuse vaccination, herd immunity does not develope Safety concerns are based on stories discovered in the media or received from the acquaintaces
- 81. LM structure of chronic abscess • The central cavity is filled with pus • The wall of abscess has an inner pyogenic membrane (granulation tissue rich in neutrophils) and an outer fibroblastic rim • Heals with fibrosis Pus in the cavity Pyogenic membrane Fibroblastic rim Subpleural lung abscess (arrow)
- 82. Multiple chronic abscesses in the liver. The patient suffered from common bile duct obstruction and purulent cholangitis
- 83. Cirrhosis of liver: chronic inflammation of the liver formation of fibrous septa, which, in turn, form nodular pseudolobules impairment of venous flow through the liver. Consequence: portal hypertension, hepatic failure
- 84. Cirrhosis of liver: nodular appearance of pseudolobules
- 85. Chronic glomerulonephritis-induced kidney shrinkage Chronic inflammation of glomeruli glomerular scarring Grossly the kidneys are symmetrically shrunken, the surface is granular (shown), and the cortex is thinned. Consequence: chronic renal failure
- 86. Honeycomb lung: inflammation or injury-induced widespread fibrosis in alveolar septa culminate in grossly evident lung fibrosis Consequence: respiratory insufficiency with hypoxemia and cyanosis Alveolar septa are widened by deposition of collagen (trichrome stain: blue).
- 87. Chronic peptic ulcer of the stomach
- 88. Venous ulceration of the leg due to poor venous drainage from the lower leg
- 89. Decubital ulcer in the sacral region
- 90. Healing by secondary intention, leading to contracture Courtesy of Prof. Dobozy Attila
- 91. Keloid Raised hyperplastic scar of the skin due to accumulation of great amount of collagen in the dermis. Common in Negroid/black people. Cosmetic problem. Shown: keloid after vaccination Courtesy of Prof. Dobozy Attila
- 92. Laryngal edema causing airway obstruction Edema of larynx induced by adverse allergic reaction of an anti- hypertensive drug administered intravenously in hypertensive crisis
- 93. Pseudomembranous-ulcerative gastritis induced by Candida Esophagus Stomach
- 94. Kaposi’s sarcoma. Tumorous nodules on the leg. Autopsy case.
- 95. Benign tumors in the uterus: expansive growth, well- defined borders, homogenous cut surface leiomyoma
- 96. Malignant tumor (bronchial carcinoma): irregular infiltrative edges, foci of necrosis, tissue destruction. Arrows: invasion of vessels
- 97. Cerebral metastasis of the bronchial carcinoma shown
- 98. Kaposi sarcoma. Tumorous nodules on the leg. Autopsy case.
- 99. Dermoid cyst of the ovary. Filled with hair, sebaceous material, and desquamated squames.
- 100. Fungating tumor in the lip; proved carcinoma histologically Courtesy of Prof. Sonkodi István, Faculty of Dentistry
- 101. Fungating carcinoma of the esophagus
- 102. Ulcerated carcinoma in the antrum of stomach: irregular margins, crater-like raised borders
- 103. Annular (napkinring-like) growth in carcinomas of the distal colon – obstructs the passage of bowel content
- 104. Papillomas of the skin • Two types: basal cell papilloma, and wart Basal cell papilloma (seborrheic keratosis) • Very common • In middle aged or older individuals • Most frequent on the trunk • Dark brown lesion with a granular surface • Often multiple
- 105. Condylomas on the glans and prepuce Prof. Attila Dobozy, Dermatology
- 106. Pedunculated polyp. LM: tubular adenoma; composed of tubular glands with dysplastic features (elongated nuclei, nuclear stratification, and architectural atypia) Stalk Bowel wall Head of the polyp
- 107. Resected bowel sample; histologically, the larger pedunculated polyp proved to be tubular adenoma with malignant transformation Head of the polyp Polyp Stalk
- 108. Unilocular serous cystadenoma of the ovary ranging more than 15 cm in greatest dimension. The outer surface is smooth; the epithelial lining of the inner surface exhibits small papillary projections. Courtesy of Bence Nagy, MD, PhD, Department of Pathology, University of Szeged
- 109. Mucinous cystadenoma of the ovary: delicate septa form cysts; mucinous material fills the cysts
- 110. Adrenal cortical adenoma: circumscribed, yellowish tumor deriving from the adrenal cortex. The tumor was hormonally inactive.
- 111. Spontaneous hemorrhage of silent adenomas blockade of CSF flow acute increase in liquor pressure death
- 112. Scirrhous carcinoma of stomach (linitis plastica) :
- 113. Signet-ring cc: tube-like thickening of the wall; LM: the mucin in the cytoplasm pushes the nucleus to te periphery
- 114. Mucinous cystadenocarcinoma of the ovari. Foci of necrosis and hemorrhage indicate malignant tumor. Invasion of ovarian surface → dissemination in the peritoneal cavity → carcinosis of peritoneum
- 115. Special skin cancer: basal cell cc (basalioma) • Most frequent among cc-s • Semimalignant • Related to chronic sun exposure • In the elderly; in the face, near the eyes and nose • Advanced lesion: ulcerated (rodent ulcer) Courtesy of Attila Dobozy, Bőrklinika
- 116. Excised breast cancer; infiltrative carcinoma with stellate appearance; gray-white strands of tumorous tissue radiate into the surrounding fat
- 117. Advanced breast carcinoma: invasion of the skin, with extensive ulceration
- 118. Glioblastoma: continuous spread through corpus callosum (butterfly tumour)
- 119. Renal cell carcinoma: continuous spread involving the cortex, the medulla and the pelvic fat
- 120. Liver metastases of colon carcinoma
- 121. Seminal vesicle Rectum Carcinoma of the prostate; arrow: extension into the paravertebral plexus
- 122. Vertebral metastases of prostatic carcinoma
- 123. Transcelomic spread: carcinosis of the greater omentum Greater omentum Greater omentum
- 124. Peritoneally disseminated ovarian carcinoma – carcinosis of peritoneum Greater omentum Stomach Stomach Liver
- 125. Enucleated eye because of retinoblastoma
- 126. ABCD of malignant melanoma Asymmetrical lesion with irregular borders Bleeding: spontaneous or upon minor trauma Color: uneven pigmentation or change in color Diameter: >6 mm Korom Irma, SZTE Dermatology
- 127. Vertical growth from the beginning: nodular melanoma Gross: deepbrown nodule LM: anaplastic tumour nests Highly malignant: hematogeneous metastases very early Korom Irma, SZTE Dermatology
- 128. Local effects Benign tumors: • Leiomyoma of the uterus: heavy menstrual bleeding, pelvic pressure/pain, frequent urination, etc. Uterine cavity Body of the uterus
- 129. Multifocal destruction of vertebrae in multiple myeloma: pain + pathological fracture
- 130. Fungating carcinoma in the lower third of the esophagus caused progressive stenosis and dysphagia Trachea Esophagus Cardia
- 131. Left: napkinring-like spread of colonic cc led to stenosis impaired the passage of stool; the frequency of passing the stool and the consistency of the stool had changed
- 132. Ulcerated carcinoma of the stomach: irregular margins, crater-like raised borders: iron-deficiency anemia and positive fecal occult blood test
- 133. Stenosing cancer of the ileocecal valve: the patient displayed change in bowel habit and iron-deficiency anemia Ileum Coecum
- 134. Invasion of pelvis by renal cell carcinoma painless microhematuria
- 135. Urinary bladder: ulcerated carcinoma on the lateral wall caused occult painless microhematuria and iron deficiency anemia Trigone
- 136. Bronchial cc. The non-tumorous bronchial mucosa (arrow) is hyperemic, swollen indicating peritumoral bronchitis caughing
- 137. Non-bacterial thrombotic endocarditis. Vegetations along the closure line of the aortic valve cups. The patient suffered from bronchial carcinoma
- 138. The vegetations caused embolic anemic infarction of the kidney (arrow) hematuria
- 139. The vegetations caused embolic hemorrhagic infarction of the small bowel bloody stool
- 140. Sacral decubital ulcer in the bed-ridden patient wearing diaper. The patient had brain infarction and hemiplegia (complete paralysis of the half of the body)
- 141. Femoral vein thrombosis; pulmonary embolism vein artery Pulm. artery Embolus
- 142. Osteoporosis: severe loss of horizontal trabeculae in vertebral bodies in the patient who suffered from brain-hemorrhage, paralysis and prolonged bed rest
- 143. 5) Ascending urinary tract infections in catheterized patients: urethritis, cystitis, acute pyelonephritis (shown)
- 144. Lobectomy because of bronchial carcinoma (arrow) in a heavy smoker Courtesy of B. Vasas, MD, Dept. Pathology, Universitiy of Szeged sq cc destructed the bronchus
- 145. 2) Induction of atherosclerosis Absorbed into the blood, cigarette smoke causes increased platelet aggregation and dysfunction of the endothelial layer of aorta and large arteries development of atheromatous plaques
- 146. Emphysema (alveolar wall destruction, enlarged air spaces) in the non-tumoral areas of the lobectomy specimen of the heavy smoker
- 147. Mucosal defects (erosions) in alcohol-abuse induced gastroduodenitis Antrum Duodenum
- 148. Hepatic steatosis: the liver is enlarged (>2000 g), soft, yellow, and greasy; LM: fat globules in the hepatocytes; reversible
- 149. Pancreas: acinar cell injury (ethanol + heavy, fatty meal) acute necrotizing-hemorrhagic pancreatitis: high mortality rate
- 150. Micronodular cirrhosis of liver
- 151. Pancreas: chronic calcifying pancreatitis: atrophied, fibrotic pancreas; irregularly dilated ducts obstructed with stones pain, malabsorption
- 152. Abnormally high deposition of visceral adipose tissue (thickness of subcutaneal fatty tissue: 10 cm), fatty liver, elevated diaphragm
- 153. Obesity-related glomerulopathy: segmental scarring of the tufts
- 154. Osteophytes in spondylarthrosis limit movements of the vertebral columns
- 155. Acute myocardial infarction Most frequent cause of death in diabetes
- 156. Cerebral infarct involving the frontoparietal region, the internal capsule and the striatum (caudate nucleus, putamen) contralateral hemiparesis Caudate nucleus Putamen
- 157. Gangrene of toe
- 158. Diabetic retinopathy: new vessels, lipid-cholesterol deposits Courtesy of Kolozsvári Lajos, SZTE Ophtalmology
- 159. Neuropathic diabetic foot ulceration: necrosis + phlegmon of sole Courtesy of R. Sipka, MD, Dept. Surgery, University of Szeged
- 160. Acute purulent pyelonephritis: several abscesses in the cortex and medulla
- 161. Mucormycosis, with spread to the orbit and CNS Courtesy of Szabó Zsuzsanna, MD, Szent László Kórház lethal within days after meninges involved
- 162. Myeloma: the tumorous plasma cell nodules destruct the bones; death in 15% of patients due to consequences of AL-amyloidosis
- 163. The amyloid deposition may not be evident grossly. In this case, the heart weight was 580 gs (normal 350 gs) LM evaluation revealed amyloid deposition
- 164. Cystic fibrosis of pancreas: fibrotic areas intermingle with cysts
- 165. Lungs of the patient who died of cystic fibrosis: purulent plugs obstruct the bronchi
- 166. The plugging of bronchi stem from obstruction and infection of the bronchi secondary to the viscous mucus secretions
- 167. Bronchiectasis, purulent bronchitis and bronchopneumonia in cystic fibrosis
- 168. Atheromatous plaque in the middle cerebral artery: raised white-yellow lesion in the intima, protruding into the lumen (formol-fixed brain)
- 169. Aorta: the plaques contain a yellow, grumous debris (arrow)
- 170. Structure of atheroma on LM • Intimal lesion • Central lipid core • Fibrous ”cap” subendothelially
- 171. Coronary occlusion due ulceration of the plaque leading to thrombosis
- 172. Cerebral infarct involving the internal capsule contralateral hemiparesis
- 173. Abdominal aorta: mural thrombi Celiac artery Superior mesenteric artery Renal artery
- 174. 24 Ruptured atherosclerotic aneurysm of the infrarenal abdominal aorta; the probe indicates the communication between the lumen and the extraaortic retroperitoneal space. The aneurysmal sac is filled with mural thrombus
- 175. Thrombosis of superior mesenteric artery: bowel infarction
- 176. Ruptured atherosclerotic aneurysm of abdominal aorta, leading to retroperitoneal bleeding and shock (the probe indicates the rupture) Iliac arteries
- 177. Saccular aneurysms in the thoracic aorta. Note mural thrombi
- 178. Degeneration of the tunica media: thinning and dilation of the aortic root, and intimal tears
- 179. Resected ascending aorta because of dissection. By the time of surgery, the process had not resulted in aortic rupture Aortic lumen Dissecting column of blood Tear Prepared by G. Nyári, MD, Dept. Pathology, Univ. Szeged
- 180. Dissection of aorta, hemopericardium Intimal tears Aortic valve
- 181. Hypertensive kidney disease • Mild, symmetric shrinkage of kidneys (nephrosclerosis), weight: 120-120 g; the surface is granular
- 182. Hypertensive heart disease. Pressure overload-induced left ventricular hypertrophy arrhythmias, chronic left-sided heart failure
- 183. Vérzések retinopathia hypertonica-ban Courtesy of Prof. Kolozsvári Lajos Hypertensive retinopathy. Ophtalmoscopic examination reveals the thickening of retinal small arteries; microhemorrhages can be present (fundus hypertonicus)
- 184. Microaneurysms undergo rupture in hypertensive crisis massive hemorrhage of the basal ganglia
- 185. Destruction of the left putamen and internal capsule by fresh hematoma
- 186. Slightly shrunken kidneys; finely granular surface
- 187. Heart weight 550 g; enlargement of the left ventricle
- 188. Kidneys: hyperplastic arteriolosclerosis Gross changes • Early changes: enlarged kidneys, pinpoint petechial cortical hemorrhages + tiny infarcts • Later, infarcts are replaced by vascular scars
- 189. Brain edema. The gyri are widened and flattened, the sulci are narrowed
- 190. Unilateral atrophy of the kidney Not shown: the atherosclerotic stenosis of the orifice of the renal artery
- 191. Takayasu arteritis, late phase. Arrows indicate fibrous narrowing of arterial orifices Aortic root Brachioceph. a Left common carotid a. Left subclavian a. Thoracic ao.
- 192. Clinical features in cranial GCA • Fever, fatigue, weight loss; sedimentation rate >50 mm/h • Palpable nodularity of the tortuous temporal artery
- 193. Brain infarcts with secondary hemorrhage in the patient who died of PAN with kidney, heart, brain and muscle involvement
- 194. GPA: cavitation of lung parenchyma, due to necrosis of small vessels and parenchyma
- 195. MPA, lungs: alveolar capillaritis bilateral air space consolidation with relative apical sparing corresponds to confluent foci of alveolar hemorrhages Courtesy of B. Radics, MD, Dept. Pathology, University of Szeged
- 196. Vasculitic purpuras Prof. Husz Sándor, Bôrklinika
- 197. Clinical features • Skin: purpuras, principally in the lower extremities • Bowels: abdominal pain, bleeding • Joints: arthritis and arthralgia • Kidneys: hematuria, proteinuria and azotemia Outcome • Depends on the extent of crescent formation; overall prognosis is good
- 198. Esophageal varices • In portal hypertension, the submucosal veins of distal esophagus undergo dilation (portocaval shunt) • Spontaneous rupture hemorrhagic shock exsanguination • Autopsy: 2000-3000 ml-s of fresh blood fills the stomach and small bowels
- 199. Venous ulceration of the leg (varicose ulcer)
- 200. Thrombosis in deep leg veins Most important consequence pulmonary embolism Femoral vein Femoral artery
- 201. Photo: 54-year-old man. Hemangiomas on his trunk
- 202. Cavernous hemangioma of the liver: the vascular channels produce sponge-like structure
- 203. Angiosarcoma of the pulmonary artery; endoluminal spread lead to occlusion
- 204. Morphologic features of concentric hypertrophy of the LV • small lumen • markedly increased wall thickness (> 20 mm) • increased mass (> 500 g) Septum Posterior wall Anterior wall Lateral wall
- 205. Morphology of dilative hypertrophy of the LV: enlarged lumen, enlarged size, slightly increased wall thickness, increased mass Septum Posterior wall Anterior wall Lateral wall
- 206. Pulmonary edema: lungs >1200 gs, congested and wet, airways contain bubbly fluid
- 207. Brown induration of lungs; atheromatous plaques in pulmonary arteries indicating sec. pulmonary hypertension collagen in alveolar septa
- 208. Morphology RV hypertrophy (thickness › 6 mm) + dilation and manifestations of chronic systemic congestion
- 209. Early phase: concentric hypertrophy of LV: wall thickness > 20 mm; weight > 500 g Septum Posterior wall Anterior wall Lateral wall
- 210. Late phase: LV hypertrophy + dilation: wall thickness < 20 mm; weight > 550 g
- 211. Occlusive thrombus (dissected with the scissor) on atheromatous plaque (arrow)
- 212. MI: yellowish area of necrosis, hyperemic border
- 213. 66 Hemopericardium due to rupture of the free wall of the LV rupture
- 214. 67 Rupture of the interventricular septum
- 216. Apical chronic aneurysm, with mural thrombus
- 217. Septum Posterior RV LV Anterior Reperfusion injury: hemorrhage in the septum, and the anterior and posterior wall; angioplasty 12 hours after the onset of symptoms
- 218. 84 Chronic IHD: dilative hypertrophy, apical fibrosis (arrow), dilated atrium, thrombus in the left auricle
- 219. Calcific aortic stenosis in congenitally bicuspid valves Subendothelial calcific masses within sinuses of Valsalva
- 220. Mitral annular calcification: regurgitation + stenosis
- 221. Thinned and enlarged leaflets, elongated and attenuated chordae tendineae, excentric LV hypertrophy
- 222. Rheumatic fever: acute verrucous endocarditis, chordae tendineae are also involved Dr. Tószegi Anna, SZTE Pathologia, 1972
- 223. Mitral stenosis: thickened leaflets, fused at the commissures; thickened chordae tendinae, dilated LA
- 224. Large vegetations on the mitral valve
- 225. Nonbacterial thrombotic endocarditis of aortic valve from a patient with adenocarcinoma of the tail of pancreas. Histology ruled out infectious endocarditis
- 226. Mechanical valve: tilting disk Bogáts Gábor SZTE Szívsebészet
- 227. Bioprothesis Bogáts Gábor SZTE Szívsebészet
- 228. Dilated CM The heart is ball-shaped; there is pronounced ventricular chamber dilation The weight of the heart was 660 g
- 229. DCM in a 2-y-old child • Extreme cardiomegaly lung compression • Congestive hepatomegaly
- 230. HCM: hypertrophy of the septum and the free wall; the volume of the LV is reduced; subaortic stenosis (arrow) is evident Note: the thickened left ventricular wall becomes stiff, prevents diastolic filling
- 231. Arrhythmogenic CM. Fibrofatty near-transmural replacement of ventricular myocardium; the lesion affected the left ventricle Courtesy of B. Radics, MD, Dept Pathol, Univ Szeged Posterior wall Septum
- 232. Diffuse mottling in myocarditis
- 233. Mural thrombi in myocarditis
- 235. Aorta Septum VSD Ao valve Anterior wall Ventricular septal defect (VSD) RC LDA
- 236. Atrial septal defect (ASD) 90% secundum type: results from deficient or fenestrated fossa ovalis in the central atrial septum • RA and RV dilation • RV hypertrophy • Dilation of pulmonary artery J.M. Kissane: Anderson’s Pathology, 1990
- 237. Ventricular septal defect (VSD) The most common congenital cardiac anomaly • Site (90%): membranous part of the septum • Dilative hypertrophy of RV • Small defects may close spontaneously J.M. Kissane: Anderson’s Pathology, 1990
- 238. Patent ductus arteriosus (PDA) The ductus (just distal to the left subclavian artery) allows blood flow between the aorta and pulmonary artery during fetal life. Normally closes within 1 and 2 days of life. PDA is associated with dilation of proximal pulmonary arteries and LV LV and later RV hypertrophy J.M. Kissane: Anderson’s Pathology, 1990
- 239. Tetralogy of Fallot (TOF) • Dextraposed aorta overriding • VSD • Pulmonary stenosis • RV hypertrophy J.M. Kissane: Anderson’s Pathology, 1990
- 240. Transposition of the great arteries (TGA) • Aorta arising from the RV • Pulmonary artery arising from the LV • A shunt (ASD or VSD or PDA) for mixing of blood J.M. Kissane: Anderson’s Pathology, 1990
- 241. Postductal coarctation (adult-type) Distal to the obliterated ductus arteriosus: • LV hypertrophy • Hypertension proximal and hypotension distal to the narrowed segment • Asymptomatic until adult life J.M. Kissane: Anderson’s Pathology, 1990
- 242. Preductal coarctation (infantile-type) • Hypoplastic aorta between the left subclavian artery and the d. arteriosus • ASD • Widely PDA • Frequently lethal J.M. Kissane: Anderson’s Pathology, 1990
- 243. Virus-induced acute serofibrinous pericarditis The pericardium is hyperemic, covered by fibrin strands
- 244. Carcinosis of pericardium; primary tumor in the lung
- 245. Biopsy diagnosis of GN • Via renal percutaneous biopsy evaluated by light microscopy (LM), immunofluorescence (IF) and elecron microscopy (EM) • Mirrors the inflammatory events occurring in all glomeruli
- 246. Severe periorbital edema in a deceased man who had the nephrotic sy
- 247. The kidney in nephrotic syndrome: the pale yellow cortex is due to lipid accumulation in renal tubules (consequence of lipiduria)
- 248. Chronic sclerosing GN: symmetric shrinkage (80-80 g); granular surface; on section, the cortex is thinned Bleeding after biopsy
- 249. Gross features in advanced disease • Diabetic nephrosclerosis: symmetrically shrunken kidneys with granular surface • Remember: diabetic nephrosclerosis, hypertensive nephrosclerosis, and chronic glomerulonephritis all lead to symmetrically shrunken kidneys
- 250. Acute pyelonephritis: multiple abscesses
- 251. Necrotizing papillitis: necrosis of pyramids
- 252. Gross:“shock kidney” enlarged, swollen kidney (~ 200 g); pale, bloodless cortex, dark medulla
- 253. The change of “shock kidney” was photographed from a deceased patient with hemorrhagic shock induced by the rupture of esophageal varices (arrows)
- 254. • Normal ureteral insertion: acts as a valve that prevents retrograde flow of the urine during micturition. • Abnormal ureteral insertion: urine refluxes in the ureter and pelvis during micturition (VUR) • May be unilateral or bilateral Kumar et al Pathologic Basis of Disease, 2005.
- 255. Abscesses in the cortex and medulla; the pelvic mucosa is hyperemic Pelvic mucosa
- 256. Confluent abscesses in the cortex of the kidney; such severe cases result in urosepsis + death
- 257. Reflux-induced chronic pyelonephritis leading to kidney shrinkage
- 258. Coarse scars overlying blunted calyces in reflux-induced PN
- 259. The sharp edges of the stone incised the urothelium of ureter during the travel hematuria
- 260. Staghorn calculus: remains localized; leads to pyelonephritic scar
- 261. Pyelonephritic scar due to stone in the calyx: obstruction + infections are keyplayers in scar formation
- 262. Hydronephrosis: dilated calyces, atrophied papillae (arrows), thinned parenchyma
- 263. 55-y-o man with sepsis induced by intrarenal abscesses. Urgent nephrectomy saved the life of the patient. The gross evaluation of the specimen revealed congenital pyeloureteral stenosis (arrow), hydronephrosis, and intrarenal abscesses Dilated pelvis Ureter
- 264. Gross Very large cystic kidneys (1000 to 4000 gs); cysts may be 3-4 cm in diameter
- 265. Enourmously enlarged kidneys elevation of the diaphragm; pulmonary hypoplasia
- 266. The cysts cause spongelike appearance
- 267. Oligohydramnios; compression of fetus By courtesy of L. Kaizer, MD, Dept Pathol, University of Szeged
- 268. Renal artery stenosis-induced atrophy of the left kidney. Note multiple small cysts in the cortex of both kidneys
- 269. ESRD with several cysts; renal cell carcinoma in the walls of the cysts (arrows)
- 270. Fresh infarct (arrow): wedge-shaped, yellow, preserved outlines
- 271. Embolism-induced vascular scars; thrombus was found in left auricle during the autopsy of the patient with the history of atrial fibrillation
- 272. End-stage kidneys: severe shrinkage (30 to 50 g each), medulla and cortex do not separate from each other, and multiple dialysis-associated cysts
- 273. Clear cell carcinoma • Solitary spherical mass; greatest dimension 6 cm • Bright yellow necrosis
- 274. Papillary carcinoma • Large solitary tumorous mass
- 275. Chromophobe carcinoma: well-circumscribed, tan-brown necrosis
- 276. Local spread. RCCs invade the parenchyma, the adipose capsule, the pelvis, the renal sinus, and the renal vein; may spread beyond the Gerota fascia
- 277. “Tumor thrombus” in renal vein (arrow), can extend into the inferior caval vein
- 278. Bronchial carcinoma. Distal to the tumor, atelectasis-associated pneumonia developes
- 279. ARDS, gross features: the lungs are heavy (1600-2000 gs), diffusely firm, red, and boggy
- 280. The lungs are solid, airless, and reddish purple
- 281. Embolic occlusion of the major pulmonary branches of the pulmonary artery
- 282. Pulmonary atherosclerosis in chronic LSHF
- 283. Emphysema: enlargement of alveolar spaces around terminal bronchioli Control lung
- 284. Emphysema Pressure atrophy of the liver where the diaphragm compressed it
- 285. Bullous E. Large subpleural blebs can develop (greater than 1 cm; usually apical). Risk of ptx!
- 286. Cylindrically dilated bronchi, which can be cut up to the pleural surface, the lumina are filled with pus, the mucosa is hyperemic. Note foci of associated bronchopneumonia (arrows)
- 287. Clubbing of fingers
- 288. Trachebronchitis in H1N1 influenza: markedly hyperemic mucosa.
- 289. Prototype • Pneumococcal pneumonia • Leads to the consolidation of an entire lobe (lobar pneumonia) or patchy consolidation of the lobe (bronchopneumonia) JCE Undervood:General and Systematic Pathology,Third edition, 2000.
- 290. Lobar pneumonia, red hepatization. The whole lobe is red, airless, with liver-like consistency.
- 291. Lobar pneumonia, gray hepatization. The whole lobe is greyish and the cut surface is dry.
- 292. Lobar pneumonia, fibrinous pleuritis. Greyish-red fibrin on the pleural surface.
- 293. Bronchopneumonia: gray-red patchy lesions slightly elevated from the cut surface. Bronchi display features of chronic bronchitis
- 294. RS virus pneumonia in an infant. The lung is heavy and red.
- 295. Bronchial carcinoma: destruction of bronchial wall (arrow), infiltration of hilar structures
- 296. Central tumor: invasion of hilum, pulmonary artery (p), and lung parenchyma; metastases in hilar lymph nodes (n) n n p
- 297. Carcinosis of pleura: grayish-white tumorous invasion of pleural surface; arrow indicates propagation via lymphatic vessels
- 298. Metastases of bronchial carcinoma in vertebrae, suprarenal glands and calvaria
- 299. Brain metastasis of bronchial carcinoma
- 300. Post-stenotic bronchiectasis Chr purulent pneumonia Large, central carcinoma Consequences of bronchial obstruction
- 301. Adenocarcinoma. Peripheral (subpleural location), simulated pneumonia on X-ray Courtesy of B. Vasas, MD, Department of Pathology, University of Szeged
- 302. Pancoast tumor. Apical tumor, infiltrated the first and second ribs. rib rib
- 303. METASTATIC TUMORS Primary sites: tumors drained by the caval system: liver, kidneys, adrenals, testis, thyroid, nasopharynx Metastatic involvement of the lungs: several tumorous foci in all lobes
- 304. Honeycomb lung. Fibrotic parenchyma surrounding the bronchi retract and create cobblestone appearance of the pleural surface.
- 305. Honeycomb lung. The dense fibrosis causes the destruction of alveolar architecture and formation of cystic spaces. Bronchi are dilated because of traction bronchiectasis. Excised pieces of lung fixed in formol. Traction bronchiectasis
- 306. Anthracosis • Common, mild, asymptomatic, in urban inhabitants, tobacco smokers • Morphology: coal dust laden macrophages along lymphatics and lymph nodes
- 307. Silicosis Gross: small fibrotic nodules, dense scars
- 308. Goodpasture sy: anti-GBM autoantibodies crossreact with alveolar basement membranes severe lung hemorrhage and symptoms of crescentic glomerulonephritis
- 309. Goodpasture syndrome Punctuated hemorrhages in the kidney Fibrin a félholdban. Crescentic glomerulonephritis; fibrin in a crescent Linear IgG along the GBM
- 310. Primary tuberculosis: Ghon complex (the inflammatory process is asymptomatic) asysmptomatic) Subpleural caseous necrosis Caseous necrosis in hilar lymph node Courtesy of Prof. T. Mikó, Sydney, Australia
- 311. Bilateral caseating tuberculotic foci in the upper lobes
- 312. Apical lung cavernas in tbc, drained by bronchus Caseous necrosis affects the the wall of bronchi, drainage of the caseous debris results in cavity (caverna) formation. Sputum (infective!!!!)
- 313. Miliary tuberculosis in lung. Cut surface of formaldehyde fixed specimen: numerous small gray-white granulomas in the lung
- 314. Bilateral pneumothorax as complication of mechanical ventilation in a patient with COPD – the lungs were collapsed, the venous return to the heart was impaired
- 315. 63 Hydrothorax in chronic right-sided HF
- 316. Dense fibrous adhesions restrict pulmonary expansion
- 317. Empyema of thorax Precipitation of the exudate leads to septations of the pleural space
- 318. Carcinosis of pleura: several tumorous nodules on the visceral pleura. Past medical history: surgically treated breast cancer
- 319. Solitary fibrous tumor of the pleura: the cut surface is solid
- 321. Carcinoma of larynx: fungating tumor destructs the vocal cords
- 322. Thyroid cartilage Thyroid cartilage The entire circumference of glottic mucosa can be infiltrated by cancer
- 323. Supraglottic tumor: ulcerated carcinoma in the epiglottis
- 324. Cleft lip (cheiloschisis) Unilateral Bilateral
- 325. Bilateral cleft lip Prof. Füzesi Kristóf, SZTE Pediatrics
- 326. Terminated pregnancy because of trisomy 13 (Patau’s sy): severe clefting of the lip and palate Dr László Kaizer, SZTE Pathology
- 327. Robbins and Cotran Pathologic Basis of Disease, 2006
- 328. Early complications •Acute purulent pulpitis (severe toothache) •Extension of infection throughout the pulp necrosis of pulp loss of tooth •Extension of infection into apical periodontium: acute apical abscess subperiosteal abscess osteomyelitis drainage through the oral mucosa („gumboil”) or to the adjacent facial skin
- 329. Late complications • Periapical granuloma: necrotic tissue at the apex of the root canal foramen, surrounded by granulation tissue infiltrated by lymphocytes and plasma cells. • Cystic degeneration and epithelialization of the granuloma radicular cyst
- 330. Recurrent aphthous stomatitis (canker sores) Aphtha (arrow) shallow ulcer on the inner surface of the lips, buccal mucosa or the tongue surrounded by hemorrhagic rim Prof. Sonkodi István, SZTE Faculty of Dentistry
- 331. Oral candidiasis (thrush) White pseudomembranes on the lingual mucosa Prof. Sonkodi István, SZTE Faculty of Dentistry
- 332. Irritation fibroma Pedunculated nodule on the apex of the tongue Prof. Sonkodi István, SZTE Faculty of Dentistry
- 333. Peripheral giant cell granuloma (epulis) in the gingiva Prof. Sonkodi István, SZTE Fogászati Klinika
- 334. Leukoplakia on the tongue - histology revealed in situ cc in the patient Prof. Sonkodi István, SZTE Fac. of Dentistry
- 335. Esophageal atresia and tracheoesophageal fistula Most common variant (C): blind upper segment, and fistula between the lower segment and the trachea. Feeding leads to aspiration pneumonia
- 336. Esophageal atresia and tracheoesophageal fistula Blind upper segment (yellow arrow and probe) and fistula between the lower segment and the trachea (red arrow)
- 337. Congenital diaphragmatic hernia. Stomach, and bowels and spleen in the thoracic cavity. The left lung is hypoplastic (arrow)
- 339. Megaesophagus: dilation of the esophagus proximal to LES, and also formation of a pulsion diverticulum
- 340. Esophageal varices Tortuously dilated submucosal veins of the lower esophagus in response to portal hypertension
- 341. Candidiasis (psuodemembranous esophagitis) in agranulocytosis
- 342. Fungating carcinoma in the lower third of the esophagus Cardia
- 344. Acute hemorrhagic-erosive pangastritis: hyperemic mucosa with punctate hemorrhages and multiple brownish-black erosions. Cardia
- 345. Acute ulcers in the postpyloric duodenum.
- 346. Acute hemorrhagic-erosive pangastritis probably induced by NSAID intake. The 65-y-old patient with severe coronary atherosclerosis, and arthrosis of hip consumed NSAIDs to releave pain. Massive gastric bleeding (hematemesis, melena) occurred which led to prolonged hypotension and, in turn, subendocardial myocardial infarcts. The patient died of acute left- sided heart failure. Cardia
- 347. CNS trauma-associated acute stress ulcers in the postpyloric duodenum. The ulcers led to hematemesis, weak pulse, tachycardia, hypotension; the patient ceased. During the autopsy, 3000 ml blood was found in the intestines.
- 348. Large peptic ulcer on the lesser curvature of the stomach; note round shape and sharp margins
- 349. Perforated antral ulcer (probe)
- 350. Autoimmune metaplastic atrophic gastritis (AMAG)-associated multiple hyperplastic polyps (P), polyps with dysplasia (D), and carcinomatous transformation (Cc) Courtesy of Bence Kővári, MD and Orsolya Oláh, MD, Dept. of Pathol, University of Szeged P P P D D Cc
- 351. Advanced gastric carcinoma: large fungating tumorous mass (line); metastasis in the lymph nodes of greater omentum (M) M M Courtesy of István Németh, MD, Dept. of Pathol, Univ. Szeged
- 352. Gastric carcinoma with two ulcer craters (arrow)
- 353. Antral gastric carcinoma infiltrating the mucosa and gastric wall Courtesy of Prof. László Tiszlavicz and Levente Kuthi, MD; Dept. of Pathol, Univ. of Szeged
- 354. Linitis plastica (leather bottle stomach): the stomach wall is thicker and more rigid because of cancerous infiltration The stomach can’t hold as much and does not move as it should
- 355. Krukenberg tumor: bilateral ovarian metastasis of signet-ring cell carcinoma Courtesy of András Vörös, MD, Dept. Pathol, Univ. Szeged
- 356. Perforated duodenal peptic ulcer: duodenal content irritated the serosa and induced hyperemia
- 357. Purulent peritonitis: creamy exudate covers the bowels and mesentery
- 358. Diffuse purulent peritonitis caused by perforation of acute ulcer of the stomach 2000 ml of pus was found in the abdominal cavity Diaphragm E.Coli Kleb. pneumo Strep. pneumo
- 359. Carcinosis of omentum; the patient had pancreatic carcinoma diagnosed during autopsy
- 360. Extreme large umbilical hernia
- 361. Invagination (intussusception) The a ag a e ( e e c e ) he d a loop, like the finger of an inverted glove
- 362. Volvulus-induced hemorrhagic infarction of the cecum and ascending colon. Arrows: not affected colon and ileum
- 363. Border of the necrotized and non-necrotized ascending colon
- 364. Luminal cause of intestinal obstruction: gallstone ileus. Proximal to obstruction, the small bowel is dilated
- 365. Consequences of intestinal obstruction The bowels proximal to the obstruction undergo dilation their wall becomes thinned their lumen is filled with large amount of fluid and gas
- 366. Ileus due to rectal carcinoma X-ray of the abdomen: distended small bowel loops and stomach filled with fluid and gas. Note fluid levels. Courtesy of Morvay Zita, SZTE Radiology
- 367. Consequences of intestinal obstruction The bowels proximal to the obstruction undergo dilation their wall becomes thinned their lumen is filled with large amount of fluid and gas Elevation of the diaphragm + Strangulation-induced bowel infarction peritonitis
- 368. Thrombosis of superior mesenteric artery (not shown) hemorrhagic infarction/gangrene of the small bowel + generalized distension of bowels indicating vascular ileus cecum Asc.Colon Transverse Colon Small Bowels Sup. Mes. a. thrombus --> Infarct in Colon --> vascular ileus and distention of Colon and SI
- 369. Shigella infection Distal colonic inflammation with shallow ulcers Colitis
- 370. Fulminant Clostridioides difficile colitis: the colon is markedly distended, confluent pseudomembranes cover the mucosa
- 372. Pseudopolyps and broad-based ulcers in ulcerative colitis
- 373. Serpentine fissures and cobblestone-like mucosa in CD (large bowel)
- 374. CD: Serpentine fissures and cobblestone-like mucosa CU: broad-based ulcers, pseudopolyps
- 375. Gross features that differ between CD and UC C disease Ulcerative colitis Bowel region Ileum + colon Rectum > distal colon > entire colon Distribution Skip lesions Continuous Broad-based ulcers and pseudopolyps Not characteristic Yes Serpentine fissures and cobblestone appearance Yes Not characteristic Transmural stricture Yes Rare Wall appearance Thick Thin Fistulae Yes No
- 376. Diverticulosis. The mucosal surface is ridged due to hypertrophy of the underlying muscle. Mucosal hyperemia indicates diverticulitis.
- 377. Tubular adenomas About half are found in the rectosigmoid; may be single or multiple Usually <10 mm and pedunculated >10 mm: areas of intramucosal carcinoma can be present (invasion of the lamina propria with no extension through the muscularis mucosae into the submucosa)
- 378. Two polyps. The smaller proved to be adenoma; the larger proved to be adenoma with malignant transformation: stalk-invasive adenocarcinoma and metastases in mesocolonic lymph nodes were observed Mesocolonic LN
- 379. Villous adenomas Most often in the rectum; solitary, sessile, diameter: up to 10 cm Composed of villi (finger-like protrusions lined with dysplastic columnar epithelium) Adenocarcinoma frequently arises in VA- s > 4 cm
- 380. Villous adenoma with malignant transformation: adenocarcinoma infiltrates the submucosa Villous Adenoma >4cm Two points of communication between Mucosal Dysplastic glands and dysplastic glands in submucosa creating the large Adenocarcinoma
- 382. Cc of the sigmoid bowel: annular (napkinring-like) growth. Lymph node metastasis in mesocolic adipose tissue R. Colon --> Fungating Into Serosa --> T3?
- 383. Carcinoma of the cecum: exophytic, fungous mass is characteristic
- 384. Rectal cc leading to ileus: extremely dilated colon proximal to the obstruction
- 385. Ca ci a f he ile cecal al e: he a ie a eak e induced by iron-deficiency anemia Ileum Carcinoma
- 386. Neuroendocrine tumor in the ileum close to the Bauchin valve T a c L , SZTE Pa a
- 387. Mural tumor in the wall of the small intestine causing subileus. Histology disclosed GIST
- 388. Ulcerophlegmonous appendicitis. The peritoneal surface is covered by fibrinopurulent exudate. Formol-fixed material
- 389. Congenital megacolon; before resection of the aganglionic segment P f. F e K f, SZTE Ped a c
- 390. Jaundice (icterus) Yellow discoloration of the skin, sclerae, and mucous membranes due to increased levels of bilirubin in circulation (> 40 umol/L) Caused by cholestasis, hemolysis or genetic disease
- 391. Chronic hepatitis C virus infection led to cirrhosis of liver: nodular alteration of the parenchyma
- 392. Alcoholic steatosis: the liver is enlarged, soft, yellowish, the edges are rounded
- 393. Autopsy of an obese woman with type 2 diabetes, hypertension, dyslipidemia, elevated ALT, AST, and bilirubin. Conversion of non-alcoholic steatohepatitis to cirrhosis was found
- 394. Female patient with the medical history of 10 years of primary sclerosing cholangitis. The normal lobular structure was replaced by fibrosis.
- 395. Hemochromatosis. Fibrous pancreas and cirrhotic liver. The brownish colour of organs is because of hemosiderin deposition
- 396. Cirrhosis Fiborus septa convert the normal liver architecture into structurally abnormal nodules (pseudolobules) HCV infection usually induces macronodular cirrhosis 5 cm alcohol - micronodular
- 397. Esophageal varices Dilated veins in submucosa in the distal esophagus; can rupture at any time
- 398. Focal nodular hyperplasia In young women (no evidence of a relationship with oral contraceptive use) Nodule-forming hyperplastic response of hepatocytes to focally increased blood flow Uncapsulated tumorlike lesion with a central stellate scar
- 399. Cavernous hemangioma Red-blue, soft nodules consist of endothelial cell lined vascular channels and stroma Blind percutaneous needle biopsy may cause severe intra-abdominal bleeding
- 400. Morphology Gross: usually in cirrhotic liver Unifocal Multifocal Diffuse
- 401. Multifocal hepatocellular carcinoma in cirrhotic liver
- 402. Intrahepatic cholangiocarcinoma, multifocal variant no cirrhosis + history adenocarcinoma = Largeduct iCCA
- 403. Metastases in the liver; the patient died of hepatic failure
- 404. Several metastatic foci in the liver
- 405. Cholesterol stones: from black to yellowish brown; multiple; faceted surface owing to tight apposition Gallbladder Cystic duct Hepatic duct Common bile duct
- 407. Pathogenesis Crystallization of cholesterol (nucleation) can be induced by • Bile supersaturated with cholesterol • Gallbladder hypomotility and/or defective gallbladder emptying • Hypersecretion of gallbladder mucus Cholesterol can no longer remain dispersed and nucleates into cholesterol monohydrate crystals
- 408. Cholesterol monohydrate crystals Precipitation of Ca++-salts Cholesterol stone
- 409. Ulcerophlegmonous cholecystitis: hyperemic mucosa covered with multiple ulcers; the wall is edematous
- 410. Thinned mucosa, thickened gallbladder wall, cholesterol stones
- 412. Hydrops: the gallbladder is markedly enlarged, the muscular wall is thinned
- 413. Carcinoma developed in chronic calculous cholecystitis. Note infiltrating growth pattern Tumorous Thickening Of GB wall Continuous spread to liver parenchyma
- 414. Carcinoma of the gallbladder. Hematogeneous metastases in the liver. Liver Metastases with spontaneous Necrosis
- 415. Muliple liver abscesses; the obstruction was managed by stenting the common bile duct
- 416. Green liver in obstructive jaundice The patient had carcinoma of the head of pancreas; the tumor infiltrated and obstructed the common bile duct; liver metastases
- 417. Carcinoma of the cystic duct, the hepatoduodenal ligament and the hepatic duct (probe) Diffusely infiltrating type Liver, Nutmeg or steatotic?
- 418. Stimulation Secretion to the duodenum Normal site of trypsinogen activation Acinus Calcium regulation • Hypercalcemia • Alcohol Trypsin related mutations • PRSS1+: activation of trypsinogen • CTRC+: ineffective trypsin degradation • SPINK1+: ineffective blockade of active trypsin Duct Duct cell secretion • CFTR Duct obstruction • Gallstone • Duct stones • Tumor • Mucus Genetic and environmental factors that affect acinar cells or ducts Modified from Muniraj et al. Disease-a-Month 60:530-550, 2014
- 419. Classification according to the severity of acute pancreatitis Clinically • mild - morphologically acute interstitial pancreatitis: interstitial (IS) edema + foci of enzymatic necrosis in the acini by LM • moderately severe - morphologically acute necrotizing pancreatitis: IS edema and gross foci of enzymatic necrosis • severe - morphologically acute necrotizing-hemorrhagic pancreatitis: the entire pancreas is involved; confluent foci of necrosis and hemorrhage; foci of enzymatic fat necrosis in the extrapancreatic collections of fat, such as the mesentery of the bowel and the omentum
- 420. Moderately severe - acute necrotizing pancreatitis IS edema and gross foci of enzymatic necrosis I idiopathic G Gallstones E Ethanol T Trauma S Shock M Mumps A Autoimmune S Scorpion Sting H HyperTG/Ca E ERCP D Drugs
- 421. Severe - acute necrotizing-hemorrhagic pancreatitis. The entire pancreas is involved; confluent foci of necrosis and hemorrhage
- 423. Severe pancreatitis. Foci of enzymatic fat necrosis in the mesentery of bowels Duoddeno-Jejunal Flexure
- 424. Complications in severe pancreatitis • SIRS (systemic inflammatory response sy)-induced shock • Bacterial superinfection of necrotic pancreatic tissue abscess(es) sepsis • Disruption of large ducts can result in unilateral pleural effusion, enlarging peripancreatic fluid collection, or pancreatic ascites • > 4 weeks: pseudocyst formation (1 to 15 cm): massive liquefactive necrosis enclosed by granulation tissue; + infection of pseudocysts pancreatic abscesses
- 425. Pathogenesis Still not understood; TIGARO classification of risk factors • Toxic-metabolic: chronic alcohol abuse (mostly in middle-aged men), hypercalcemia, chronic renal failure, etc. • Idiopathic • Genetic-induced: SPINK1 gene mutation or PRSS1 gene mutation or CFTR gene mutation (no extrapancreatic manifestations of cystic fibrosis) • Autoimmune • Recurrent acute pancreatitis • Obstruction of pancreatic duct by stone or tumor or congenital abnormality (pancreas divisum [1 papilla minor + 1 accesory duct])
- 426. Alcoholic chronic pancreatitis: atrophied, markedly fibrotic pancreas, irregularly dilated ducts obstructed with Ca- carbonate stones + pseudocysts (not present in this patient) =Chr. Calcifying Pancreatitis
- 427. Carcinoma (cc) in the pancreatic head, infiltrating the papilla of Vater and the common bile duct (cbd). Distal to the tumor, obstructive pancreatitis developed. The Wirsungian duct is markedly dilated and tortuous W W cc cbd
- 428. Cc of the pancreas: hard, poor-defined mass; difficult to distinguish from chronic pancreatitis
- 429. Hematogeneous metastases in the liver
- 432. Immunopathology of severe SARS-CoV-2 lung disease Inflammatory lung injury: impaired innate antiviral defense, overactivated innate immune response Upper airways: evasion of IFN-I response → robust viral replication → infection extends to the lung Uncurbed viral replication Weak IFN-I response Cytopathic damage to pneumocytes, endothelial cells → DAMPs DAMPs overactivate alveolar macrophages Weak viral clearance Weak CD8+ cytotoxic T cell response Influx of activated monocytes, neutrophils Alveolar edema, hyaline membranes, alveolar collapse Progressive diffuse alveolar damage and ARDS + death Adapted from Med Res Rev 2020; 1-28
- 433. 71-y-o male patient with hypertension, chronic ischemic heart disease and lethal SARS- CoV-2 lung disease Diffuse gray-white consolidation, admixed with hemorrhage; thrombi in pulmonary vessels (arrows). Formol-fixed specimen. Infected in nursing home 14 days prior to death. Fracture of femur, operated urgently 9 days prior to death. Fever and progressive ARDS started 2 days prior to death. Autopsy performed by B. Radics, MD, Department of Pathology, University of Szeged
- 434. Timeline of Covid-19 Modified from New Engl J Med 2020;383:2451-60 Onset of symptoms Median days from infection -5 8 13 -4 -3 -2 -1 0 1 6 5 4 3 2 7 9 10 11 12 14 15 16 17 18 Incubation period Airways: viral replication evades IFN-I response and extends to alveoli Fever Cough Fatigue Anorexia Myalgias Mild or moderate pneumonia, dyspnea Severe pneumonia, ARDS, hypoxemia + hypercytokinemia, coagulopathy, shock 19
- 435. Plasma Water 92% Proteins 7% Albumin 58% Globulins 37% Fibrinogen 4% Regulatory proteins 1% Other solutes 1% Electrolytes (Na, K, etc.) Nutrients (glucose, amino acids etc.) Respiratory gases Waste products Red cells (erythrocytes) 4-5.5 million/ L Buffy Coat Platelets (thrombocytes) 150.000-400.000/ L White cells (leukocytes) 4.500-11.000/ L Neutrophils (54-62%) Lymphocytes (25-33%) Monocytes (3-7%) Eosinophils (1-3%) Basophils (0-0.75%) 45% 55% COMPOSITION OF BLOOD Packed red cell volume: Hematocrit
- 436. BONE MARROW Red marrow: active, blood cell forming In adults: flat bones (pelvis), vertebrae Yellow marrow: inactive, fatty tissue → it may turn red again in cases of blood loss (adaptation), or in myeloid neoplasias (leukaemias)
- 437. BONE MARROW Top: in AML, the diaphysis is replaced by leukemic red bone marrow. Bottom: normally, the diaphysis of femur is filled with yellow fatty bone marrow. red tumorous bone marrow seen in aml and a l l it's a sign of bone mineral haematopoiesis suppression leading to anemia thrombocytopenia and sometimes granulocytopenia ( leukemic leukaemia) JML has many subtypes one of them is PML associated with translocation 15:17 between PML L Gene and rara play which could be as viewed as a hey good prognostic sign since atra could be used with arsenic trioxide to treat it and a special sign of the subtype is the dic due to the procoagulant release while another subtype with differentiating monocytic can cause leukaemia cutis
- 438. In certain diseases, the HSCs can travel in the blood from the bone marrow in one bone to another bone and may settle in the liver and spleen (extramedullary hemopoiesis)
- 439. Aspiration of the bone marrow yields a bone marrow cytological smear
- 440. Trephine (Jamshidi) biopsy to investigate the constituents of bone marrow yields a tissue core of bone marrow
- 441. Diseases of blood, hematopoietic and lymphoid system Red blood cell disorders White blood cell disorders Coagulation system disorders Anemia Erythrocytosis Leukopenia Reactive leukocytosis Neoplasms Thrombocytopenia Thrombocytosis Coagulopathies Pancytopenia (anemia, leukopenia, thrombocytopenia ”Clot or bleed”
- 442. Pallor of skin Pale Skin is a sign of Anemia there are many causes of anywhere I like to think of them as as deficiency anaemia iron deficiency B12 B9 deficiency then we can talk about the factory the bone marrow and diseases affecting the bone marrow such as aplastic anaemia tumor infiltration suppression by irradiation then we can talk about the red blood cells themselves haemoglobin could be affected in thalassemia and sickle cell anaemia the memory could be defective in spherocytosis and elliptocytosis enzyme deficiencies such as pyruvate kinase gcpd H deficiencies then we can talk about hemolytic anemias such as autoimmune hemolytic anaemia malaria induced microscopic an geopathic hemolytic anaemia ( TTP dic( and finally we can talk about blood loss which could be acute in case of traumatic injuries or chronic in case of gynecology renal or GI pathologies
- 443. - Iron deficiency - Anemia of chronic disease - Thalassemias - Sideroblastic anemia Anemia Microcytic Normocytic Macrocytic Reticulocyte count Low High - Megaloblastic anemia * B12 deficiency * Folate deficiency - Non-megaloblastic *Alcoholic liver disease *Other liver diseases Marrow failure • Aplastic anemia • Myelofibrosis • Myelophthisis • Marrow suppression (drugs, chemotherapy, radiation) Chronic renal failure Anemia of chronic disease Acute blood loss Hemolytic anemias • Sickle cell anemia • G6PD deficiency • Hereditary spherocytosis • Autoimmune hemolitic anemia
- 444. Acute Massive bleeding from ruptured blood vessels: Traumatic wounds (eg.: car accidents) Ruptured aortic aneurysm Ruptured esophageal varices Gastric or duodenal ulcer Ectopic pregnancy Etc. Loss of intravascular volume (>20% loss of blood) hemorrhagic shock and may lead to death If the patient survives hemodilution (movement of fluid into the vascular space) normocytic normochromic anemia Tissue hypoxia EPO RBC production with reticulocytosis normali ation within 3-4 weeks Chronic GI tract (ulcers, polyps, tumors, IBD, angiodysplasias, hemorrhoids, etc.) Gynecological (heavy or frequent menstrual bleeding, metrorrhagia abnormal uterine bleeding) Urological (kidney or bladder cancer) IRON DEFICIENCY ANEMIA ANEMIA OF BLOOD LOSS: HEMORRHAGE
- 445. • Iron in food (2 forms): – Heme iron (bound to Hb and myoglobin – in meat) – Fe2+ (ferrous) – Non-heme iron – free iron molecules in Fe3+ (ferric) • Plant-based foods (spinach, beans, lentils) IRON METABOLISM
- 446. IRON METABOLISM Fe HCl HEME IRON NON-HEME IRON Fe3+ Fe2+ Fe2+ Ferri-reductases Fe2+ Heme-transporter Fe2+ DMT-1 HCl Fe2+ Fe2+ Fe3+ Transferrin (iron transporter) Duodenal cell Blood Target tissues Ferroportin Hephaestin Erythropoiesis Liver Hepcidine - Storage of iron: intracytoplasmic ferritin and hemosiderin (eg.: in macrophages) Iron loss by shedding of epithelial cells Transferrin-receptor Stomach Duodenum Muscle Ferritin Intake: 10-20 mg/day
- 447. Gross morphology: yellow fatty marrow at sites of red bone marrow (sternum)
- 448. Petechial hemorrhages in severe thrombocytopenia
- 449. Myelophthisis: Prostate carcinoma metastases in spine and femur (bottom: normal trabecular structure after formol fixation) Lung, pancreas and Breast can also metastasise to bone
- 450. Hb Globin Amino Acids Heme Biliverdin Bilirubin Heme oxygenase Biliverdin reductase Fe2+ A Bilirubin / albumin complex MACROPHAGE I di ec bi i bi c j ga ed bi i bi Stercobilin Ha g bi HEMOLYSIS RBC c F ee he g bi Pink serum <120 days INTRA- VASCULAR EXTRA- VASCULAR
- 451. CAUSES OF VITAMIN B12 DEFICIENCY B12 Parietal cell Intrinsic factor (IF) B12-IF complex IF receptor Ileum Stomach Blood Colon Transcobalamin II Target tissues Storage in the Liver a e B12 Vegeterians Poor diet absorption (malabsorption) - production of IF - Gastrectomy - Pernicious anemia - ileal absorption: - Ileal resection - Ileal inflammation: Crohn- disease - Consumption by intestinal bacteria or tapeworms
- 452. PERNICIOUS ANEMIA B12 Parietal cell Intrinsic factor (IF) B12-IF complex IF receptor Ileum Stomach Blood Colon Transcobalamin II • Definition: – A subtype of B12 deficiency induced megaloblastic anemia • Cause: – Autoimmune disease against the parietal cells and intrinsic factor – IF B12 absorption – Chronic atrophic corpus gastritis with intestinal metaplasia (AMAG) risk of gastric cancer Auto- antibodies
- 453. Diseases of blood, hematopoietic and lymphoid system Red blood cell disorders White blood cell disorders Coagulation system disorders Anemia Erythrocytosis Leukopenia Reactive leukocytosis Neoplasms Thrombocytopenia Thrombocytosis Coagulopathies Pancytopenia (anemia, leukopenia, thrombocytopenia ”Clot or bleed”
- 454. CLASSIFICATION BASED ON NORMAL CELL LINES • Myeloid neoplasms – Acute myeloid leukaemias (AML) – Chronic myeloproliferative neoplasms (MPN) – Myelodysplastic syndromes (MDS) • Lymphoid neoplasms – Precursor lymphoid neoplasms (ALL) – Mature lymphoid neoplasms • Mature B-cell neoplasms • Mature T- and NK-cell neoplasms – Hodgkin lymphoma • Histiocytic neoplasms
- 455. MYELOID NEOPLASMS: CLASSIFICATION Maturation arrest + ↑↑ replication Defective maturation Proliferation of terminally differentiated myeloid cell lines Secondary maturation arrest + ↑ replication 1) Acute myeloid leukemias 3) Chronic myeloproliferative neoplasms 3) Myelodysplastic syndromes New oncogenic mutations
- 456. Grossly, the sites of yellow bone marrow are infiltrated by tumorous red bone marrow. Top: in AML, the diaphysis is replaced by leukemic red bone marrow. Bottom: normally, the diaphysis of femur is filled with yellow fatty bone marrow.
- 457. CML Polycythemia vera Essential thrombocytosis Primary myelofibrosis Clinical features Peak age 50-60 yrs 40-60 yrs 70 yrs 70 yrs Splenomegaly Yes (Massive) Yes 30% (slight) Yes (Massive) Bone marrow Panhyperplasia (predominantly granulopoiesis) Panhyperplasia (predominantly erythropoiesis) Isolated megakarycytic hyperplasia with large megakaryocytes in clusters Panhyperplasia with fibrosis Peripheral blood Erythrocytes Mild anemia Erythrocytosis (polycythemia) Mild anemia Mild anemia Granulocytes Markedly increased Norm.-mildly increased Normal (slightly increased) Normal to moderately increased Platalets Normal to moderately increased Normal to moderately increased Markedly increased (giant thrombocytes) Inreased to decreased Genetics Philadelphia chromosome (BCR/ABL rearrangement) JAK2 activating mutation JAK2 activating mutation; MPL activating mutation JAK2 activating mutation MPL activating mutation
- 458. Myelofibrosis (right): osteosclerosis of the marrow spaces of sternum. Left: normal sternum
- 459. Myelofibrosis Note extreme splenomegaly induced by extramedullary hemopoiesis (myeloid metaplasia). The arrow indicates spontaneous infarction of the spleen parenchyma. The patient died of consequences of transformation to acute myeloid leukemia. Liver Spleen Stomach
- 460. Non-Hodgkin lymphoma: enlarged lymph nodes, the cut surface is homogeneous, grayish-white lymphoma that could be Hodgkin's or non-Hodgkin's hodgkin's lymphoma is characterized by contiguous surprised lymphadenopathy that is usually the cervical region it is characterised by symptoms such as fever night sweats and weight loss also characterized by presence of certain cells such as reed-sternberg cells hodgkin's cells and lacunar cells it has Ford main subtypes for the classical hodgkin's lymphoma the nodular sclerosing mixed hypercellularity lymphocyte rich and deleted while then non Hodgkin lymphoma could be further classified based on whether the tumor is aggressive2 or indolent
- 461. Marginal zone lymphoma in the stomach and the regional lymph nodes (formol-fixed specimen) Pancreas Stomach this is a GI lymphoma most common GI landform what is the diffuse large b-cell lymphoma and then the marginal zone lymphoma and then the celiac disease associated t-cell lymphoma they are associated with chronic inflammation aka helicobacter pylori infection or celiac disease they are highly aggressive
- 462. Marked enlargement of the hilar and paratracheal lymph nodes; the disease was diagnosed as DLBCL during autopsy Larynx Trachea Tongue
- 463. Superior vena cava sy caused by an agressive tumor; autopsy revealed enlarged paratracheal, hilar and mediastinal lymph nodes; T-cell lymphoma was confirmed
- 464. Erosions of cancellous bone of calvarium in myeloma
- 465. Erosions of cancellous bone of vertebrae in myeloma myelomas are tumors arising from mature plasma cells that produce immunoglobulin light chain bence-jones protein that leads to renal failure and gastric property and bence Jones proteinuria it is also associated with hypercalcemia due to the stimulation of osteoclast through cytokines you can also cause anaemia and Bone defects presenting as pathological fractures the disease starts as monoclonal gammopathy of uncertain significance asymptomatic myeloma then symptomatic over to myeloma it is characterized by by m-protein Spike and the produced immunoglobulins could act as autoantibodies and generally they are dysfunctional so we will have hypogammaglobulinemia
- 466. Toxoplasma-lymphadenitis Ingestion of oocysts from cat feces; the protozoon disseminates in the human body; the inflammatory response, including lymphadenitis, destructs the parasites).
- 467. Markedl enlarged pleen ( 1000 g) in ad l Myelofibrosis CML CLL
- 468. Myelofibrosis. Note extreme splenomegaly induced by extramedullary hemopoiesis (myeloid metaplasia). The arrow indicates spontaneous infarction of the spleen parenchyma. The patient died of consequences of transformation to acute myeloid leukemia. Liver Spleen Stomach
- 469. Invasive thymoma: The surgical resection margin (blue) is infiltrated by the tumor
- 470. litterer siwe disease affect children, filtration of skin spleen liver bone marrow can be lethal third disease is is hand-schuler-christain having a triad of exopthalmus diabetes insipidus calvarial bone defects
- 471. P of. Ba P l, Ne o ge Diffuse brain edema: ventricular spaces are severely narrowed
- 472. 1. Subfalcine herniation Unilateral mass lesion forces the ipsilateral cingulate gyrus to be compressed underneath the falx cerebri focal necrosis and hemorrhage in the herniated tissue + compression of the anterior cerebral artery Kumar, Cotran, Robbins: Basic Pathology 2003 Subfalcine herniation
- 473. 2. Transtentorial herniation Transtentorial herniation • Expansion of the hemisphere the uncal gyrus of hippocampus is herniated underneath the free edge of the cerebellar tentorium
- 474. 2. Transtentorial herniation Transtentorial herniation •The ipsilateral oculomotor nerve undergoes compression: ipsilateral fixed pupil • Posterior cerebral artery compression occipital infarction, cortical blindness • Cerebral peduncle compression upper motor neuron signs • Brainstem compression cardiorespiratory failure, death
- 475. 3. Tonsillar herniation Tonsillar herniation Transtentorial herniation The cerebellar tonsils are forced into the foramen magnum and compress the respiratory and cardiac centers within the medulla cardiorespiratory failure, death
- 476. Compression of cerebellar tonsils and medulla oblongata by the foramen magnum Green=Deep lesion Red= Necrotic features
- 477. Striped hemorrhages in the pons in response to tearing of small vessels(Duret hemorrhages) Secondary hemorrhages to a space occupying leion Can be seen in Tonsillar herniation
- 478. Hydrocephalus Preparation of late P of D . Gell Albe SZTE Anatomy Department
- 479. Hydrocephalus: severe enlargement of the ventricles, atrophy of the brain Usually Atrophy of the brain leads to ventricular enlargement But in this case the enlargement of the ventricles is huge so maybe the ventricular enlargment (Primary Hydrocephalus) preceeded and cause pressure atrophy of the brain
- 480. Sec. (compensatory) hydrocephalus The increase in CSF volume occurs following brain atrophy: HC ex vacuo The intracranial pressure is normal
- 481. Fracture contusion with necrosis of GM and WM, hemorrhage and brain oedema Coup Contre-coup
- 482. The branches of middle meningeal artery run between the dura mater and the skull
- 483. Epidural hematoma • Temporal bone fracture rupture of middle meningeal artery accumulation of arterial blood between the dura and the skull: EH • Lucid interval followed by a rapid in intracranial pressure P of. Ba P l, Ne o ge
- 484. The bridging veins between the dura mater and the arachnoid membrane
- 485. The middle cerebral artery is the most frequent site of occlusion in association with atherosclerosis
- 486. Thromboembolism: several infarcts with secondary reperfusion hemorrhage in the territory of the middle cerebral artery Caudate nucleus Internal capsule Putamen of lentiform nucleus Supplied by Ant. cerebral a. Midline shift is also present Cavity of Septum pallucidum "Cavum Septi Pellucidi" It is normaly present in fetuses and closes on its own, finding it in adults is not a pathologcal finding per se, but rather an antomical variation, sometimes could be considered as a marker of neural maldevelopment.
- 487. Cerebral infarction: wedge-shaped softening of the parietal lobe and the internal capsule Caudate nucleus Thalamus infarction Globus pallidus infarction Whitesh yellowish necrotic area with irregular border and surrounded by edema Blurring of WM and GM on left side compared to the well demarcated right side Caudate is infarcte GP is spared
- 488. Hypertensive hemorrhage in the left hemisphere, lacunar state in the right basal ganglia Formol-fixed brain Huge hemorrhagic lesion "Apoplexy"
- 489. Hypertensive patient with psychomotor slowness: bilateral lacunar infarcts in the deep WM focal myelin loss From psychomotor slowness it could progress so vascular dementia
- 490. Fresh hematoma distructs the putamen, the WM of parietal lobe, and the internal capsule Midline shift
- 491. Hemocephalus in the fourth ventricle - lethal Extension to subarachnoidal space --> Subarachnoidal hemorrhage Substantia Nigra could be seen as a thin dark line Maybe some signs of Duret Hemorrhage
- 492. Multiple hemorrhages in blastic crisis
- 493. Berry aneurysm of the circle of Willis
- 494. Subarachnoid hemorrhage due to ruptured berry aneurysm
- 495. Glioblastoma. Distortion of the temporal WM and thalamus, note foci of necrosis, cystic change and hemorrhage Heterogenous appearance "Glioblastoma Multiforme"
- 496. Glioblastoma. Butterfly pattern of spread through the corpus callosum
- 497. Cerebellar metastasis of breast carcinoma (autopsy disclosed the primary tumour) Well circumscribed Lung cancer and melanoma are most likely to present with multiple metastasis, whereas breast, colon, and renal cancers are more likely to present with a single metastasis primary brain tumors could be pilocytic astrocytoma diffuse astrocytoma anaplastic astrocytoma glioblastoma oligodendrogliomas ependymoma medulla blastoma meningioma schwanoma and neuroblastoma
- 498. Parasagittal meningioma Falx cerebri Found incidentaly Hard to excise since it is near the Falx cerebri Tendency to recur
- 499. Gray-tan, firm plaques in the WM of brain and spinal cord; commonly beside the lateral ventricles; optic nerve is frequently involved Multiple Sclerosis "MS"
- 500. The plaques are located in the white matter: well-circumscribed, glassy, gray-tan, irregularly shaped lesions Multiple Sclerosis "MS"
- 501. Alzheimer disease. Cortical atrophy, characterized by narrow gyri and widened sulci (meninges had been removed)
- 502. The medial structures of the temporal lobe display marked atrophy. Note compensatory ventricular enlargement – HC ex vacuo Sup. and Middle Temporal Gyrus Atrophied Cingulate Gyrus Relatively preserved Middle Frontal Gyrus Atrophied
- 503. Gross: depigmentation of the substantia nigra and locus coeruleus
- 504. Acute purulent meningitis of the brain and the spinal cord Engorged veins
- 505. Multiplex brain abscess, pyocephalus internus; the patient was hypertensive, the reason why lacunar state was also observed Pyocephalus internus Lacunar infarcts Abscess
- 506. Chronic abscess of the spinal cord
- 507. Anencephaly - lethal • The calvaria and the hemispheres are absent • The base of the skull is covered by a mass of vascular granulation tissue (area cerebrovasculosa) D . Kai e L , SZTE Pa h g
- 508. Encephalocele Malformed CNS tissue extends through a defect in the cranium Occurs in the occipital region or in the posterior fossa Lethal D . Kai e L , SZTE Pa h g
- 509. Neuro - Fejlődési rendellenesség - Spina bifida Myelomeningocele and rachischisis D . Kai e L , SZTE Pa h g
- 510. Holoprosencephaly: incomplete separation of hemispheres D . Kai e L , SZTE Pa h g
- 511. Agenesis of corpus callosum D . Kai e L , SZTE Pa h g
- 512. Phyllodes tumor
- 513. BC Screening Before the advent of breast cancer screening programs breast cancer was mainly detected as a symptomatic disease. In the era of BC screening many cases are detected in an asymptomatic (non- palpable) stage; many in the non-invasive or in situ ha e
- 514. Carcinoma of cervix Specimen removal termed: Hysterectomy and salpingo-oopherectomy
- 515. Carcinoma of cervix
- 516. Carcinoma of cervix
- 517. Cervical cancer in advanced stage causing hydronephrosis
- 518. Leiomyoma Uterine Cavity Solitary circumscribed leiomyoma If located submucosaly they cause bleeding If intrnurally then it can block/narrow lumen of fallopian tubes Rarely they rise subserosaly bulging out of the contours of uterus
- 519. Serous cystadenocarcinoma Cysts are visible on the cut surface "Next image"
- 520. Serous cystadenocarcinoma Cysts with Papillary ingrowth pattern
- 521. Mucinous cystadenoma, multicystic Gelatinous substance remains in the cyst after the cut Mucin flowed out
- 522. DERMOID CYST filled with hair, sebaceuous material
- 523. DERMOID CYST
- 524. Urolithiasis of the bladder Note inflammatory hyperemia of trigone Ureter Ureter
- 525. Autopsy case of multifocal, cauliflower-like exophytic bladder tumor (the 78-y-old patient had iron deficiency anemia). Histologic evaluation revelealed nonmuscle-invasive papillary UCC. Lateral wall Posterior wall Trigone Ureter
- 526. Muscle invasive UCC: the layers of bladder (mucosa, submucosa, muscularis propria) are invaded by the cancer Detrusor muscle Serosa Mucosa
- 527. Slices of radical cystectomy specimen fixed in formol. Muscle-invasive UCC; the tumor has invaded the perivesical fatty tissue (arrow) Courtesy of F. Sükösd, SZTE Pathology
- 528. 54-year-old, smoking male evaluated because of weakness. Iron deficient anemia and microhematuria were found; abdominal ultrasound scans revealed a tumorous mass in the renal pelvis. The symptoms were caused by papillary UCC (arrow), evidenced by the pathological examination of the nephrectomy specimen Courtesy of L. Kuthi, SZTE Pathology
- 529. UCC of the ureter: the exophytic tumor clogged the lumen and caused hydronephrosis (next slide)
- 530. The tumor caused dilation of the ureter and hydronephrosis
- 531. Control of pregnancy by ultrasound examination of the fetus. Oligohydramnios, abdominal cyst?, bilateral hydronephrosis were observed, and the pregnancy was interrupted. The autopsy identified the posterior urethral valve and the extreme dilation of the bladder as the consequence of urinary tract obstruction developed in the fetus. Courtesy of L. Kaiser, SZTE Pathology
- 532. Gonorrhoea • 2-7 days after exposure: acute purulent urethritis • Complications: purulent prostatitis, seminal vesiculitis, epididymitis Late consequences: • Urethral stricture urinary tract obstruction • Fibrosis of the prostate • Fibrosis of the epididymis; if bilateral: obstructive azoospermia Dr. Husz Sándor, Dermatology
- 533. Venereal ulceration of the glans penis • Genital herpes: HSV2, HSV1 (increasing incidence due to practice of oral sex); painful vesicles ulcer + inguinal lymphadenitis • Firm chancre: Treponema pallidum; painless firm ulcer + painless inguinal lymphadenitis; heals with a subtle scar; 2 months later: secondary syphilis: gen. lymph node enlargement, mucocutaneous lesions • Soft chancre (chancroid): Hemophilus ducreyi; common in Africa and Southeast Asia; painful soft ulcer + painful inguinal lymphadenitis with central abscesses
- 534. Firm (luetic) chancre: painless ulcer at the site of initial inoculation Dr. Husz Sándor, SZTE Dermatology
- 535. Phimosis Abnormally small orifice in the foreskin; does not permit the retraction of the foreskin over the glans penis Füzesi Kristóf, SZTE, Pediatrics
- 536. Condyloma acuminatum (venereal wart). Cauliflowerlike lesions involving the coronal sulcus, the glans, and inner prepuce Dr. Husz Sándor, Dermatology
- 537. Penile intraepithelial neoplasia. Plaques on the glans, prepuce and orifice. Dr. Husz Sándor, Dermatology
- 538. Carcinoma of the penis Dr. Husz Sándor, Dermatology
- 539. Partial penile amputation because of invasive SCC of preputium, coronal sulcus and glans. Formol-fixed specimen. Courtesy of L. Kuthi, SZTE Pathology
- 540. 62-y-old man with type 2 diabetes who suffered from a large abscess of prostate (arrow) and purulent cystitis and died of urosepsis. E. coli grew from the exudate. L. Kuthi, Department of Pathology
- 541. Morphology Gross • Nodular enlargement (60-100 g; normal: 20 g), • The nodules have no capsule
- 542. Frequent: the hyperplastic nodule elevates the trigone and compresses the internal urethral meatus. Note trabecular hypertrophy and acute cystitis
- 543. Obstruction of urinary flow caused by hyperplastic nodule
- 544. Nodular hyperplasia of prostate, obstruction of urinary flow, bilateral ureterectasis, pyelectasis and hydronephrosis. The patient had renal failure Courtesy of L. Kuthi, SZTE Pathology Prostate Bladder
- 545. Infection of residual urine in the bladder: acute cystitis, ascending pyelonephritis
- 546. Morphology Gross • PCCs arise multifocally in the peripheral posterior zone of the prostate, facilitating palpation during rectal digital examination • Appear as multifocal firm, grayish- yellowish masses (arrow)
- 547. Urinary bladder Carcinoma invading the periprostatic tissues; the prostatic urethra is narrowed (arrow).
- 548. Continuous spread: involvement of seminal vesicles. Lymphatic metastases (arrow) along the iliac arteries Rectum Seminal vesicle
- 549. Prostatic carcinoma: hematogeneous metastases in the spine (retrograde venous spread)
- 550. Twisting of the spermatic cord hemorrhagic necrosis of the testis; orchiectomy had to be performed Füzesi Kristóf, SZTE, Pediatrics
- 551. Varicocele (marked) and small seminoma were verified during the evaluation of 26-y-old man with oligospermia
- 552. Seminoma invading the paratesticular structures: homogeneous, lobulated cut surface
- 553. Non-seminomatous GCT involving almost the entire testis, invading the extratesticular structures, and spread along the spermatic cord. The heterogeneous cut surface indicates extensive necrosis within the tumor; the feature of NSGCTs
- 554. Non-seminomatous mixed GCT (this case: seminoma + embryonal cc + teratoma) T E S
- 555. Phyllodes tumor
- 556. BC Screening • Before the advent of breast cancer screening programs breast cancer was mainly detected as a symptomatic disease. • In the era of BC screening many cases are detected in an asymptomatic (non- palpable) stage; many in the non-invasive or „in situ” phase
- 557. Malar rash Erythema affecting the facial butterfly (malar) area (bridge of the nose and cheeks); upper eyelids and nasolabial folds are not involved Husz Sándor, Dermatology
- 558. Photosensitivity Dermatitis at sites exposed to sunlight Pokorny Gyula, Rheumatology
- 560. Confluent foci of lethal pulmonary hemorrhage in SLE, not verified clinically 23-year-old female. Coughs for 2 weeks, dyspnoe, weakness and pain in her knees and shoulders. Low grade fever. Chest X-ray: bilateral patchy opacities; left-sided pleural effusion. Proteinuria 2+, urinary sediment: 25 RBCs, se-creatinin 180 umol/L; Hematocrit: 26
- 561. 5 manifestations were present simultaneously Coughs, dyspnoe, bilateral patchy opacities pulmonary hemorrhage Weakness and pain in her knees and shoulders polyarthritis Low grade fever active disease Left-sided pleural effusion pleurisy Proteinuria 2+, urinary sediment: 25 RBCs, se-creatinine 180 umol/L lupus nephritis Hematocrit: 26 anemia
- 562. Radiographic hallmark of RA: erosions in joints Pokorny Gyula, Rheumatology Normal joints
- 563. Pokorny Gyula, Rheumatology Fusiform swelling of the joints
- 564. Progressive pulmonary fibrosis Cobblestoned pleural surface owing to the retraction of fibrosis along the interlobular septa
- 565. Dermal fibrous thickening: prevents movements of fingers Prof. Pokorny Gyula, Rheumatology Scleroderma Skin thickinenin of both hands extending proximal to metacaropphalengeal joints
- 566. Prof. Pokorny Gyula, Rheumatology Thickening and tightness of the skin mask-like face c c
- 567. Raynaud’s phenomenon due to small vessel obliteration. Gangraene of toes autoamputation Ondrik Zoltán, SZTE, Internal Medicine
- 568. Clinical syndromes of pituitary disease Anterior pituitary syndromes Posterior pituitary syndromes - Nonfunctional adenomas / carcinomas - Metastases - Surgery, irradiation - Inflammation - Ischemic necrosis - Pituitary haemorrhage (apoplexy) - Hypothalamic diseases (rare) Hyperpituitarism Hypopituitarism Local mass effects - Functional adenomas - Functional carcinomas (very rare) - Hypothalamic diseases (rare) Diabetes insipidus ADH deficiency Syndrome of inappropriate ADH secretion (SIADH) ADH excess ↑ secretion of trophic hormones ↓ secretion of trophic hormones
- 569. Gross: Nonfunctional adenoma bulges from the sella (autopsy case) Macroadenoma more than 1 cm Downward extension to inferior sella turcica
- 570. Cross section of the adenoma Cavernous sinus Carotid Carotid Tumor Tumor Oculomotor nerve Carotid Carotid Grayish tan with cystic degeneration Necrosis and Hg can be seen Irrguular shape Infiltrate or compress neighbouring structures